








Introduction
Laparoendoscopic inguinal hernia repair has significant advantages over open surgery. Patients mostly benefit from lower risk of surgical-site infection and postoperative pain, faster recovery and better cosmetic effect. The technique therefore is frequently applied for patients with no contraindications to general anesthesia or laparoendoscopy (such as inability to tolerate pneumoperitoneum). The current belief is that cardiovascular and pulmonary-related comorbidities as well as uncorrectable coagulopathy (bleeding disorders included) are also contraindicated [1–7]. Congenital bleeding disorders are quite rare diseases characterized by deficiency of certain blood coagulation factors. These deficiencies result in a tendency to spontaneous or perioperative bleeding, the intensity of which is proportional to the coagulation factor deficiency. The most common congenital bleeding disorders are hemophilia A (factor VIII deficiency), hemophilia B (factor IX deficiency), and von Willebrand disease (vWD) (a complex disorder the components of which may include abnormalities of von Willebrand factor function, quantity or quality of factor VIII, and reduced platelet count). Depending on the severity of the clotting factor deficiency, hemophilia may be severe (factor VIII or IX activity < 1 IU/dl), moderate (1–≤ 5 IU/dl) or mild (> 5– < 50 IU/dl). vWD is classified into types 1, 2, and 3. Type 1 vWD is generally the mildest and type 3 the most severe. Forms of type 2 are intermediate in severity [8–11]. In the perioperative period patients with congenital bleeding disorders require specific pharmacological treatment, most often consisting in supplementation of the deficient coagulation factor. Perioperative hemostasis is quite a challenge for the multidisciplinary team (surgeon, hematologist) because even if the correct concentration of deficient factors is maintained, there remains a high risk of bleeding complications. Therefore, due to fear of life-threatening bleeding, open surgical techniques are frequently applied because hemostatic control is easier than with laparoendoscopic techniques, although the latter are more beneficial for patients [6, 8–16].
Aim
The primary goal was to evaluate the risk of hemorrhagic complications and hernia recurrence in patients with congenital bleeding disorders and without hemorrhagic diathesis subjected to totally extraperitoneal inguinal hernia repair (TEP-IHR). Secondary goals were to compare postoperative pain, analgesic drug demand, operative time, hospital stay and recovery in these two groups of patients.
Material and methods
This prospective study comprised patients admitted for elective inguinal hernia repair in the period 2010–2018. The study group (hemophiliacs, H group) consisted of patients with congenital bleeding disorders; the control group consisted of patients without bleeding disorders (non-hemophiliacs, NH group). Patients operated on in the same week were assigned to the appropriate study groups. Men over 18 years of age with primary or recurrent, unilateral or bilateral inguinal hernias were included into the study. Excluded from the study were patients after pelvic surgery from midline incisions below the umbilicus or with irreducible or incarcerated inguinal hernia or inguinoscrotal hernias. The participants were asked to give written informed consent and the study was approved by the local ethics committee. Obligatory antibiotic prophylaxis was administered at 2 g of cefazolin in a single dose. Prophylaxis of thromboembolic events (nadroparin 0.3 ml, s.c.) was conducted for patients with no bleeding disorders. Patients with bleeding disorders were given clotting factor concentrates (CFCs) for 8 days, intravenously every 12 h at an adjusted dose. Hemophilia A patients were given factor VIII (at a dose calculated to achieve the concentration of 80–100 IU/dl on surgery day, 60–80 IU/dl on days 1–3, 40–60 IU/dl on days 4–7). Hemophilia B patients were given factor IX to achieve the concentration of 60–80 IU/dl on the day of surgery, 40–60 IU/dl on post-operative days 1–3, and 30–50 IU/dl on days 4–7. Von Willebrand disease patients were given von Willebrand factor and factor VIII in the same mode as hemophilia A patients [8, 10–14].
On surgery day, hemophilia A and vWD patients used approximately 50 IU/kg of clotting factor, and in hemophilia B patients the amount was approximately 40 IU/kg. During the next 7 days, the clotting factor dose was adjusted following the outcome of morning concentration measurement. Repair surgery was performed with TEP technique using the Ultrapro mesh implant (Ethicon, Diegem Belgium) with fixation only for defect size larger than 3 cm (AbsorbaTack Fixation Device (Covidien, Dublin Ireland). Pain intensity was assessed on the Numerical Rating Scale (NRS) and paracetamol was used to relieve pain. Patients were allowed to walk and drink 4–6 h after the procedure. Discharge occurred not earlier than 24 h after the operation and depended on the patient’s general condition. Study data were collected on the 1st, 2nd, and 7th days and 1 and 3 months after the procedure. All patients were warned against heavy lifting for a month and after that no restrictions on physical activity were imposed. For patients with bleeding disorders, the hemostatic effect of RT was assessed intraoperatively by determining bleeding intensity during the procedure as well as occurrence of bleeding complications in the postoperative period. All TEP-IHR procedures were performed under general anesthesia, using a conventional three-port midline technique without the use of a balloon dissector [17]. In direct inguinal hernia procedures, the extended transversalis fascia was retracted and ligated with absorbable sutures. In indirect inguinal hernia procedures the hernial sac was completely dissected from the spermatic cord. Type of hernia was determined intraoperatively using the EHS (European Hernia Society) groin hernia classification. No drainage of the surgical site was performed [18].
Statistical analysis
The statistical analysis was performed using Prism 7.0 (GraphPad, La Jolla, CA, USA). The D’Agostino-Pearson normality test was used to assess the data distributions. The unpaired t-test was used for patient age group comparison. The Mann-Whitney U-test was applied to compare the groups of data that did not meet the assumptions of the parametric test. The χ2 test was used for comparison of qualitative variables. Results were considered statistically significant when p < 0.05 in all the analyses.
Results
Seventy-eight patients reported for elective surgery, including 27 patients with bleeding disorders. Five patients were excluded from the study group with hemorrhagic disorders (H group): 3 due to scrotal hernia, and 2 declined to participate. The H group consisted of 22 patients. A control group comprised 51 patients without bleeding disorders (NH group), but 6 were excluded from the study: 2 due to contraindications to general anesthesia and 4 due to scrotal hernia. Finally, the NH group consisted of 45 patients. All patients of the H group and 43 (95.6%) of the NH group reported for the scheduled follow-up examination. The results of 22 H group patients and 43 NH group patients were subject to analysis. The results of the search and the process of screening for inclusion in the study are illustrated in the study flow chart (Figure 1). No statistically significant differences in the distribution of traits between the study groups were found except for health condition assessed by the American Society of Anesthesiologists Physical Status Classification System (ASA) (Table I). The H group comprised 16 hemophilia A patients (HA patients) (6 severe, 10 mild), 3 severe hemophilia B (HB patients) and 3 von Willebrand (vWD patients) (2 patients with type 1 and 1 with type 2a).

Table I
Characteristics of the patient population. Data are presented as number of patients (n) and percentages (%)
| Parameter | H group (n = 22) | NH group (n = 43) | P-value |
|---|---|---|---|
| Age [years] median, range | 51, 19–70 | 49, 26–75 | 0.3041a |
| BMI [kg/m2]: | 0.0426b | ||
| Normal (18.5 ≤ BMI ≤ 24.9) | 13 (59.1%) | 22 (51.2%) | |
| Overweight (25 ≤ BMI ≤ 29.9) | 6 (27.3%) | 17 (39.5%) | |
| Obese (BMI > 30) | 3 (13.6%) | 4 (9.3%) | |
| Previous surgery: | 0.8036b | ||
| Yes | 8 (36.4%) | 17 (39.5%) | |
| No | 14 (63.6%) | 26 (60.5%) | |
| ASA class: | < 0.001b | ||
| I | 0 (0%) | 21 (48.8%) | |
| II | 16 (72.7%) | 17 (39.5%) | |
| III | 6 (27.3%) | 4 (9.2%) | |
| Unilateral hernias | 16 (72.7%) | 29 (67.5%) | 0.6622b |
| Bilateral hernias | 6 (27.3%) | 14 (32.5%) | |
| Recurrent hernias | 4 (18.2%) | 9 (20.9%) | |
| Total number of operations | 28 (100%) | 57 (100%) | |
| Hernia side: | 0.8003b | ||
| Right sided | 17 (60.7%) | 39 (68.2%) | |
| Left sided | 11 (39.3%) | 18 (31.8%) | |
| Hernia type – EHS classification: | |||
| Lateral: | 17 (60.7%) | 38 (66.6%) | 0.9885b |
| I | 5 (17.8%) | 11 (19.3%) | |
| II | 10 (35.7%) | 23 (40.3%) | |
| III | 2 (7.1%) | 4 (7.0%) | |
| Medial: | 9 (32.1%) | 19 (33.3%) | 0.7685b |
| I | 1 (3.6%) | 3 (5.3%) | |
| II | 5 (17.8%) | 9 (15.8%) | |
| III | 2 (7.1%) | 7 (12.3%) |
Factor supplementation
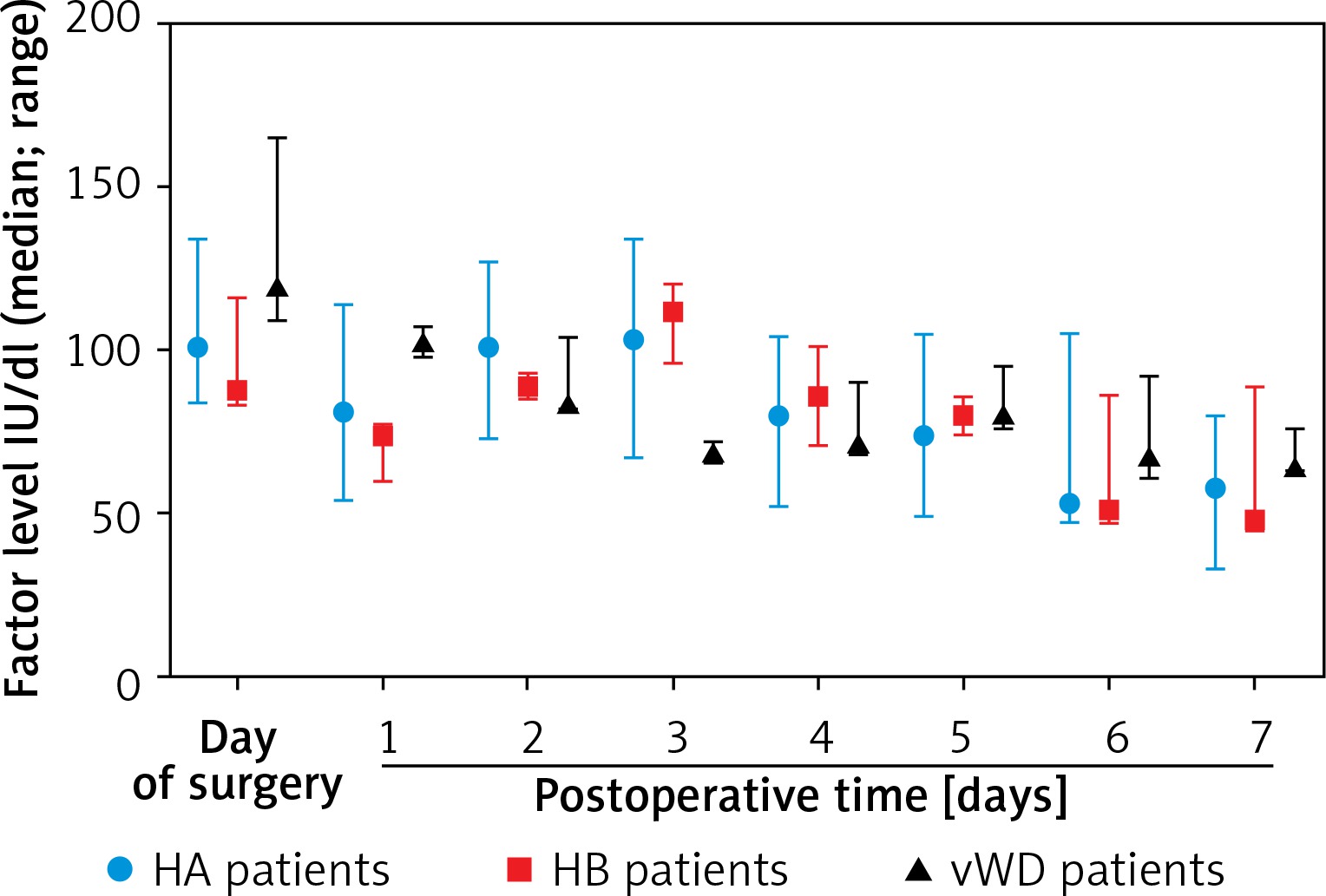
On surgery day the median clotting factor supplementation was as follows: in HA patients 100 IU/kg (82, 41), in HB patients 152 IU/kg (135, 197), in vWD patients 56 IU/kg (51, 78). On postoperative days 1–3, the median factor supplementation was: in HA patients 86 IU/kg (28, 122), in HB patients 135 IU/kg (36, 197), in vWD patients 40/IU/kg (17, 57). On postoperative days 4–7, the median factor supplementation was as follows: in HA patients 27 IU/kg (0, 80), in HB patients 34 IU/kg (0, 72), in vWD patients 20 IU/kg (0, 57) (Table II).
Table II
Median clotting factor supply for 1 kg of body weight per day
Median clotting factor levels are presented in Figure 2.
In hemophiliacs the RT hemostatic effect assessed intraoperatively was found to be very good. In both H and NH groups, none of the patients experienced life-threatening bleeding and none required red blood cell transfusions or reoperation due to bleeding complications. No statistically significant differences between the study groups were found with regard to incidence of postoperative bleeding complications. Local hematomas were observed in 11 patients (4 (18.2%) from the H group and 7 (13.9%) from the NH group) and subcutaneous hematomas in 8 (3 (13.6%) from the H group and 5 (11.6%) from the NH group) (Table III). In the H group patients who developed local hematomas (1 with severe hemophilia B, 2 with severe hemophilia A and 1 with mild hemophilia), the achieved concentration of deficient clotting factors was within recommended values. The difference in factor VIII levels between hemophilia A patients with hematomas and other hemophilia A surgical patients was statistically insignificant (mean 75.7± 17.4% vs. 89.3± 14.11%, p = 0.1066, Mann-Whitney test). No such calculations were performed for hemophilia B due to the small number of patients (three). No delayed bleeding was observed for patients in the H group. No hernia recurrence in the study groups was recorded during 3-month follow-up. No statistically significant differences between H and NH groups were recorded with regard to median duration of unilateral and bilateral TEP-IHR; 66 vs. 67 min and 127 vs. 105 min, respectively. Peritoneal tears were observed with comparable frequency in both groups, with no statistically significant difference (Table IV). Return to preoperative level of activity occurred on the third postoperative day. In the NH group however it was observed more frequently (p = 0.037) and more patients returned to the preoperative level of activity earlier than in the H group (i.e. 3rd day). Duration of postoperative hospitalization in the H group lasted 7 days and was significantly longer (p < 0.0001) as compared to the NH group (3 days) (Table IV). On postoperative days 1, 2, and 7 most patients reported pain intensity at the surgical site (0-6 according to NRS) (Figure 3). During the first and third month, pain was reported sporadically by single patients. During the first month, the pain intensity reported by H group patients was significantly greater than that reported by the NH group – 1 (0, 6) vs. 0 (0, 4) (p = 0.0210), respectively. At the 1st, 2nd and 7th days and the 3rd month, the differences in pain intensity between study groups were statistically insignificant (Mann-Whitney U-test).
Table III
Hemorrhagic complications
| Parameter | H group (n = 22) | NH group (n = 43) | P-value |
|---|---|---|---|
| Local hematoma: | 4 (18.2%) | 7 (13.9%) | 0.6548b |
| Umbilicus | 1 (4.5%) | 0 (%) | |
| Groin | 1 (4.5%) | 2 (4.6%) | |
| Spermatic cord/scrotal | 2 (9%) | 5 (11.6%) | |
| Subcutaneous hematoma | 3 (13.6%) | 5 (11.6%) | 0.0526b |
Table IV
Overall comparison of surgery-related and outcome parameters
| Parameter | H group | NH group | P-value |
|---|---|---|---|
| Duration of operation unilateral hernias [min]: median (range) | 66 (51–106) | 67 (40–130) | 0.8373a |
| Duration of operation bilateral hernias [min]: median (range) | 127 (76–172) | 105 (81–168) | 0.1654a |
| Peritoneal laceration: | 0.1882b | ||
| Yes | 9 (40.9%) | 25 (58.1%) | |
| No | 13 (59.1%) | 18 (41.9%) | |
| Analgesic consumption in 1st postoperative week: median (range)* | 1.5 (0–3) | 1.0 (0–3) | 0.8409a |
| Return to pre-operative activity [days]: median (range) | 3 (1–5) | 3 (0–5) | 0.037a |
| Length of postoperative stay [days]: median (range) | 7 (6–8) | 3 (1–5) | < 0.0001a |
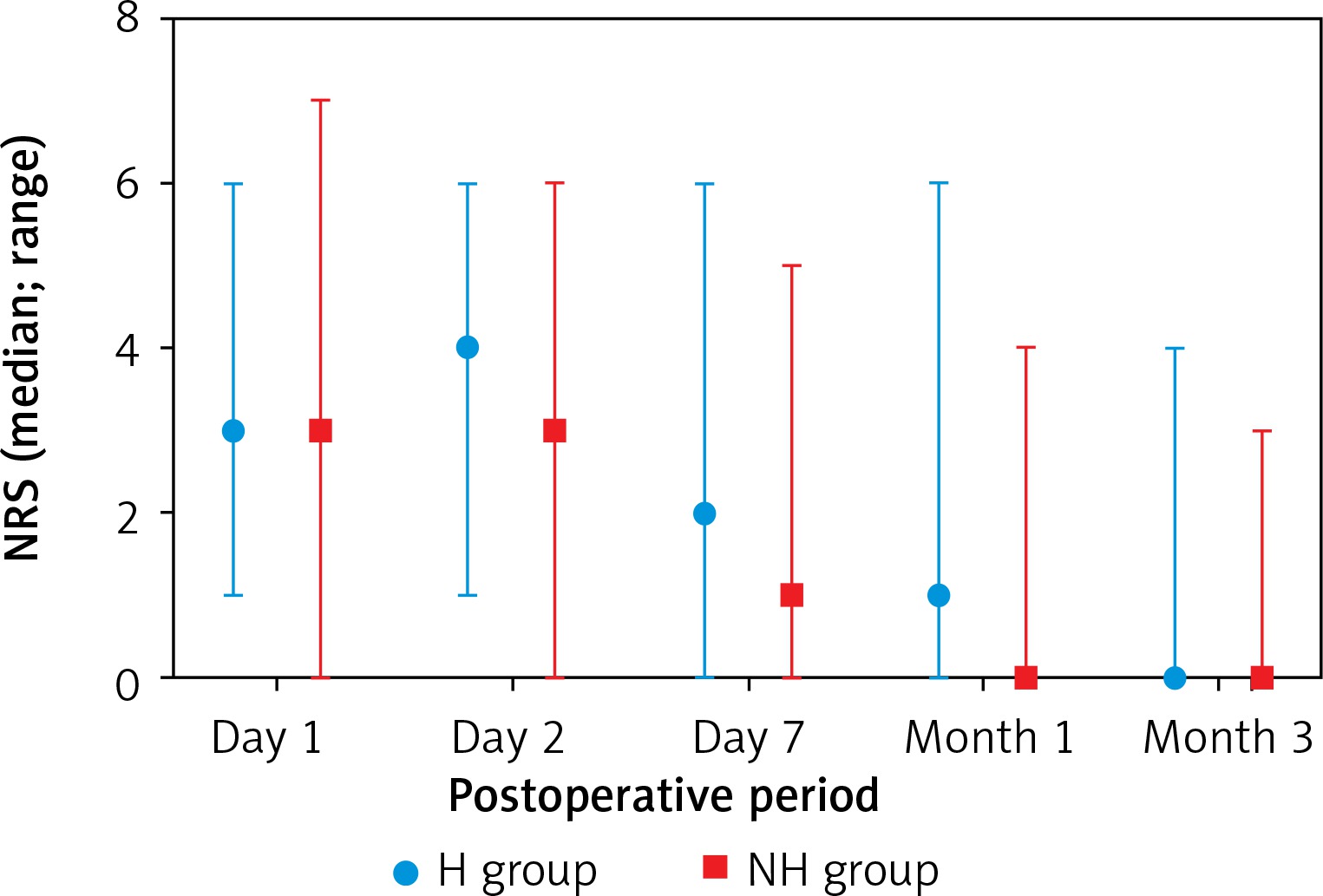
No statistically significant difference was recorded between the groups with regard to the amount of analgesic (paracetamol g per/day) administered on the 1st, 2nd and 7th days following surgery (H vs. NH; 1.5 (0, 3) vs. 1.0 (0, 3)), median (minimum level, upper level) Mann-Whitney test. As concerns analgesic management in the 1st and 3rd months following surgery, differences in the demand for painkillers were not assessed due to the low number of patients who reported pain.
Discussion
From the historical perspective, surgical management of patients with congenital hemorrhagic disorders has always been burdened with high risk of failure. In the mid-20th century life-threatening bleeding and deaths were reported for 66% of hemophilia patients as a result of minor or major surgical interventions [8, 19–23]. Nowadays, in these patients substitution of deficient blood clotting factors is applied in the perioperative period to improve hemostatic control [8, 12, 14, 23]. Although the use of clotting factor concentrates has markedly reduced the percentage of bleeding complications to 10% and the mortality rate to 4.5%, hemophilia patients are still at higher risk of bleeding, delayed wound healing and postoperative infections. If surgery is required, the open approach is frequently selected as offering a better chance of achieving local hemostasis than the laparoendoscopic technique, although the latter is associated with better outcome (faster recovery, less operative trauma, cosmetic benefits, reduced postoperative pain, shorter hospital stay) [6, 8, 15, 16, 21, 24–26]. Although the dose and duration of CFC administration remain controversial, in 2010, we performed several pioneer TEP-IHR procedures in close cooperation with hematologists and according to the guidelines for hemophiliacs undergoing surgery. No significant technical difficulties were reported and no bleeding complications occurred. Postoperative follow-up demonstrated the procedures to be successful for preventing hernia recurrence. Our above observations and the results of the works published at that time allowed us to state that the use of laparoendoscopic techniques in patients with congenital bleeding disorders is feasible and effective and is not associated with a higher risk of adverse events than open approaches [5, 12, 16, 23, 25]. Therefore, in the years that followed we conducted a study whose primary goal was to establish the safety and efficacy of the use of TEP-IHR (with replacement therapy) in patients with congenital bleeding disorders. Like Goldmann et al. in 2010 [25], we reported no deaths, but our study included patients scheduled for inguinal hernia elective surgery. It is therefore difficult to compare our results directly to literature records that refer to less homogeneous groups of patients. However, according to literature data, the mortality rate for surgical patients with bleeding disorders and ongoing replacement therapy (RT) ranges from 1.4% to 9% [19–22]. We observed no life-threatening bleeding complications or need for red blood cell (RBC) transfusions in patients with bleeding disorders. The incidence rate for local hematomas did not differ significantly between the H group and NH group – 18.2% and 13.9% respectively. Our results are consistent with those presented in similar studies which evaluate surgical management of hemophilia patients with RT support [5, 25–34]. However, the percentage of local hematomas for both H and NH patients is higher than that reported in the literature for corresponding groups of patients: 5–10% for patients with bleeding disorders [5, 24, 26] and an average of 8% for patients with no hemorrhagic disorders [26, 29–31]. Duration of unilateral and bilateral hernia surgery in the study groups was similar and there was no significant difference in median duration. This leads to the conclusion that hemorrhagic disorder in patients undergoing TEP-IHR with adequate RT support does not impede surgery. Prolonged hospitalization for our study patients with hemorrhagic disorders was justified by the need to control RT. Return to preoperative activity was mostly observed on the third postoperative day. In the NH study group however the frequency was significantly higher, which may be explained by the different health status. Delayed return to preoperative activity in the H group may be associated with hemorrhagic disorder and in some cases with arthropathy as one of the complications of hemophilia. Pain intensity and the need of analgesics during the first postoperative week were low and did not differ significantly between study groups. This is consistent with the results of TEP-IHR evaluation studies [7, 26, 29–34]. The significantly higher pain intensity reported by patients with bleeding disorders 1 month after surgery is difficult to interpret because we do not know of any similar studies which evaluated postoperative pain in patients with and without bleeding disorders. The advantage of our study is that it was conducted prospectively with a control group in patients with hemorrhagic disorders, operated on due to one disease – inguinal hernia. On the other hand, its disadvantage is the small number of participants. It should be noted however that surgical management of patients with bleeding disorders is a great challenge and procedures of this type are seldom performed, so the study outcome usually regards relatively small and often heterogeneous groups of patients. It would therefore be warranted to verify the results provided by our interdisciplinary team on a larger group of patients from other hemophilia comprehensive care centers.
Conclusions
In hemophilia and von Willebrand patients with clotting factor supplementation totally extraperitoneal inguinal hernia repair is not associated with higher risk of bleeding complications than in patients without bleeding disorders.
In hemophilia and von Willebrand patients totally extraperitoneal inguinal hernia repair with clotting factor supplementation is feasible and as effective for prevention of hernia recurrence as in patients without bleeding disorders.
In hemophilia and von Willebrand patients totally extraperitoneal inguinal hernia repair with clotting factor supplementation is burdened with a comparable demand for painkillers but with higher pain intensity as in non-hemophiliac patients.
Hospitalization and recovery in hemophilia and von Willebrand patients were recorded as significantly longer than for non-hemophiliac patients.