
Introduction
A common and historically based belief is that an increased susceptibility to multiple or severe infectious diseases, especially caused by unusual pathogens, is the most common manifestation of inborn errors of immunity (IEI) [1]. During the past decade an increasing number of reports pointed to other clinical phenotypes which, when missed, might lead to serious complications [1–4].
Skin plays an important role in immune homeostasis [5]. Errors in inborn mechanisms of specific antigen response resulting in faulty production of cells or substances regulating skin protection and manifested as inflammatory conditions of variable intensity have been collected under a common name of “primary atopic disorders” (PADs) [6]. Severe atopic dermatitis (AD) or eczema, erythroderma, and urticaria belong to leading features of PADs. Without specialized laboratory methods, differentiation of similar cutaneous manifestations of various origin is sometimes impossible. Skin biopsy, although evaluated by an experienced pathologist, might also not help to establish the diagnosis or suggest potentially most effective treatment.
An increasing awareness of the association between skin problems and faulty function of the immune system, as well as novel drugs able to target defective mechanisms, have an enormous impact on patient’s prognosis. Several attempts have been made to introduce diagnostic criteria that will facilitate establishing the diagnosis. Hanifin-Rajka criteria [7] are most frequently used for diagnosis of AD. Their reported sensitivity and specificity fall around 87.9–96% and 77.6–93.7%, respectively [8]. Although AD is generally considered a Th2-associated disease, it is increasingly recognized as multifactorial and heterogeneous [9]. Several criteria have been developed for inborn errors of immunity [10], but until currently there has been no specific laboratory test or definite criterion for diagnosis of PADs. In case of hyper-IgE syndrome caused by dominant negative variants in STAT3 gene (HIES), the prominent representative of PADs generally associated with Th17 deficiency, the diagnosis is based on selected clinical and laboratory criteria [11]. Some criteria included in widely accepted NIH or STAT3 scores [12, 13] are difficult to verify in young and very young children, as the characteristic features develop with age.
Interpretation of most laboratory parameters is usually straightforward as based on generally accepted criteria and reference ranges. This however did not apply to evaluation of Th2 or Th17. Until recently their identification required analysis of cytokines produced in cell cultures or induced intracellularly [14, 15]. Both methods remained poorly standardized and produced results difficult to interpret [16]. Description of differential expression of surface receptors characterizing effector T helper cells depending on their function [17] remained unpractical for diagnostic purposes especially in children, due to lack of normal age-related reference ranges. This study has been initiated to verify whether a simple, widely available, and relatively cheap flow cytometric test performed in whole blood samples may generate diagnostically useful data.
Aim
For this purpose, we collected peripheral blood samples from healthy subjects and patients suffering from model diseases: AD and Job’s syndrome. Skin lesions in both diseases may look extremely similar, especially in very young patients, when other clinical manifestations of HIES developing with age cannot be manifested. Considering that treatment modalities differ in both diseases, discrimination between them may become urgent. Samples from healthy subjects have been used to establish age-related reference ranges. Samples from patients with mixed atopic/seborrheic dermatitis (MD) were additionally used to verify the discriminating potential of the established reference ranges.
Material and methods
The healthy control group was composed of 42 subjects of various ages, without history of allergy, atopy, skin lesions of any kind, or medication. The patient cohort included 40 subjects with severe skin lesions admitted to the Outpatient Immunology Clinic of the Children’s Memorial Health Institute, Warsaw (Poland) between 2018 and 2021. Among them, twelve patients were diagnosed as hyper-IgE Job’s syndrome (STAT3 DN) based on results of molecular tests, 19 patients were suffering from clear atopic [7, 8], while remaining nine – from mixed atopic/seborrheic dermatitis. All patients have been examined by an experienced physician. Generally accepted SCORAD scale [18] was used to describe the patients’ skin condition. The score above 50 was considered an inclusion criterion for patients from AD and MD groups. Any concomitant systemic treatment (chronic antibiotics, steroids, cyclosporine, or biological treatment, e.g. anti-IL4 or anti-IL13 antibody) was considered an exclusion criterion. All HIES patients received prophylaxis with co-trimoxazole (18 mg/kg daily) before entering the study. This treatment was initiated when the first clinical suspicion of the diagnosis was raised. One HIES patient was treated with voriconazole due to aspergilloma in pneumatocele. NIH [19] and STAT3 scores [13] were used to describe other clinical features, as required by the diagnostic criteria of Job’s syndrome. Other laboratory and clinical data have been retrieved from medical documentation.
Peripheral blood samples were used for identification of target cell populations based on differential expression of chemokine receptors specific for each of the analysed cell subsets. Th1, Th2, Th9, Th17, Th17.1, Th22, and ThG, as well as circulating follicular helper cell subsets TFH1, TFH2, TFH17, and TFH17.1 were analysed by flow cytometry as described by Mahnke et al. and Wingender [20, 21]. Details of the procedure are presented in Supplementary file.
Informed consent from the patient (if adult) or his/her parent/legal guardian (in case of patients under 16 years of age) has been obtained for participation in the study, conducted in accordance with the Helsinki Declaration. The institutional review board of the Children’s Memorial Health Institute has approved the study (28/KBE/2018), supported by statutory grant no. S175/2018.
Results
Normal course of effector T helper cell development from birth to adulthood was evaluated based on the analysis of flow cytometric results obtained in peripheral blood samples from 42 healthy subjects, aged 2 weeks to 41.4 years. The negative history of atopy, allergy, immune dysregulation, or any other defect affecting skin condition, resulting in elevated serum IgE immunoglobulin levels or eosinophil count were required as inclusion criteria. Results were split among 5 age groups, i.e. < 2 years of age (n = 11), 2 to 5 years (n = 4), 5–10 years (n = 6), 10–16 years (n = 8), and above 16 years of age (n = 13).
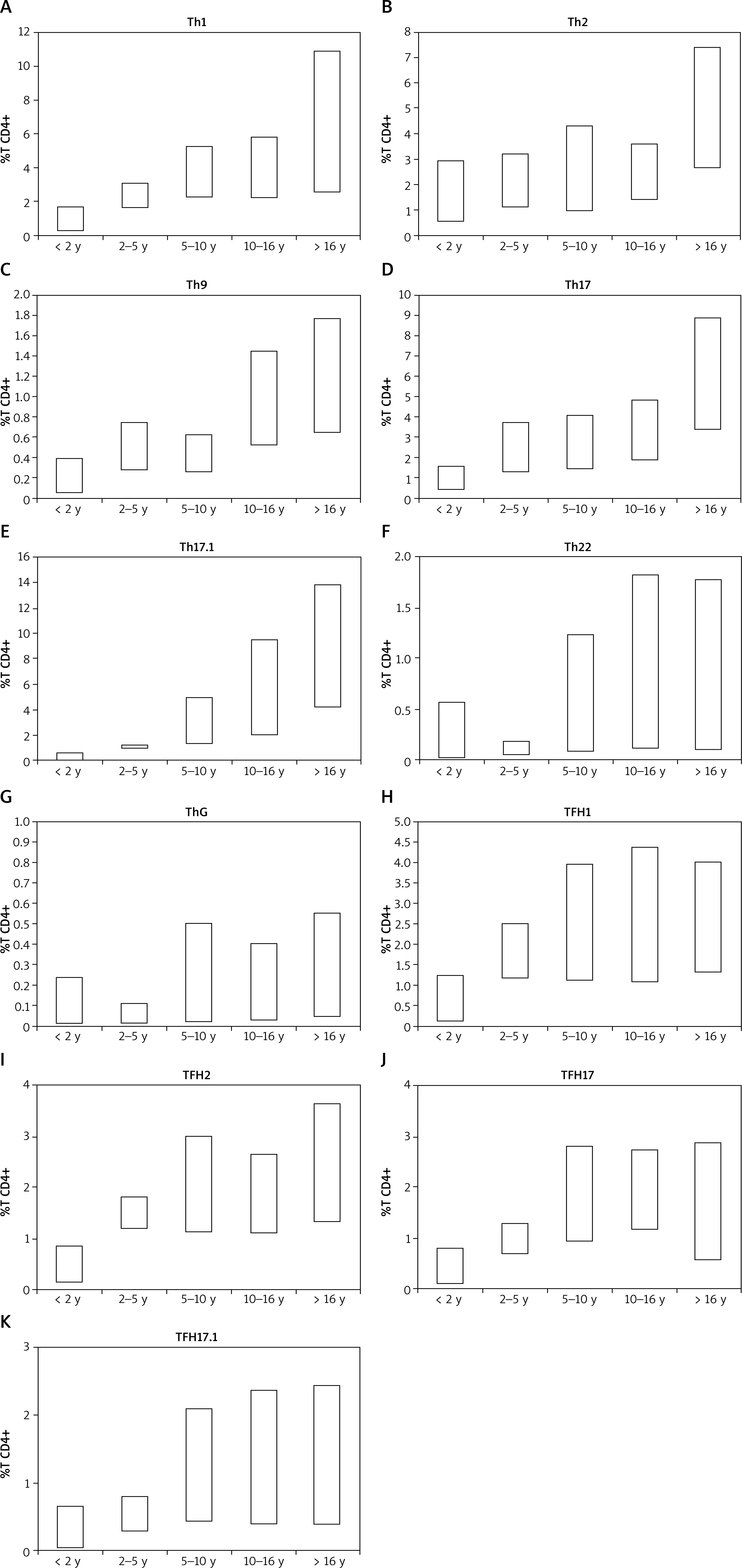
Subpopulation-specific expression of CD3, CD4, CD45RA, and chemokine receptors CCR10, CD183 (CXCR3), CD185 (CCR5), CD194 (CCR4), CD196 (CCR6) was used to define Th1, Th2, Th9, Th17, Th17.1, Th22, ThG, and circulating follicular TFH1, TFH2, TFH17, and TFH17.1 subsets. Age-related reference ranges for relative content of each of the analysed populations were calculated as falling between 5th and 95th percentile. Except for Th22 and ThG, all analysed lymphocyte subsets composed increasing-with-age populations. An unexpected drop in proportion of Th22 and ThG was observed in children between 2 and 5 years old (Figure 1). Detailed data on reference ranges are presented in the supplementary file.
Figure 1
Distribution of cytokine-producing T helper subsets based on differential expression of chemokine receptors using multicolour flow cytometry. Normal values were defined as falling between 5th and 95th percentile
The patient group was composed of 40 patients referred to the Outpatient Immunology Clinic in the Children’s Memorial Health Institute between 2018 and 2021, with significantly inflamed skin and/or elevated serum IgE. Patients have been assigned into one of three groups: hyper-IgE STAT3 DN (HIES), finally composed of 12 patients, atopic dermatitis (AD, n = 19), or mixed seborrheic/atopic dermatitis (MD, n = 9) based on medical data, diagnostic criteria (NIH and STAT3 scores, SCORAD evaluation), and results of molecular testing [12, 13, 18]. Data regarding patients’ selected clinical and laboratory features are presented in Tables 1 and 2.
Table 1
Clinical characteristics of patients included in the study group in relation to NIH and STAT3 scores. HIES denotes patients with molecularly confirmed STAT3 DN variant
Table 2
Individual results of laboratory parameters (effector T helper cell subsets, IgE and eosinophil count) of patients included in the study. Bold denotes results above normal range, italics – below normal range
All 12 patients with Job’s syndrome carried a loss-of-function variant in the STAT3 gene and all except one (HIES3) demonstrated reduced Th17 below the age-related reference ranges defined in this study (Supplementary Table S1). All patients with reduced Th17 demonstrated also reduced TFH17. Nine patients presented also reduced Th9 lymphocytes. Three patients, including the patient with normal Th17, demonstrated an elevated Th2 population, despite housing a pathological variant of the STAT3 gene. The diagnostic criteria based on several clinical parameters, with NIH score of 30 considered diagnostic, were met by 11 patients, while Woellner’s criteria (STAT3 score) – only by 8 patients. All 4 patients who did not reach the diagnostic score (NIH/STAT3 score above 30) were evaluated before reaching 10 years of age. Other laboratory biomarkers, such as elevated IgE and eosinophilia, were above reference ranges in 11 of 12 patients. Detailed data are shown in Table 2.
Thirteen (68.4%) patients from the AD group demonstrated elevated Th2, and none reduced Th17 cells. In 18 patients from this group the NIH/STAT3 scores were below 30. Two patients demonstrated low Th9, but all had normal Th17 and low NIH/STAT3 scores. In a single patient (AD7) with elevated scores (NIH 36/STAT3 33.3), neither Th17 or Th9 fell below reference ranges. Results of molecular testing in this patient were negative for known pathological variants of STAT3.
The MD group was composed of very young children, mostly below 2 years of age. None of them met the diagnostic criteriafor HIES or AD at the time of cell subset testing, despite significantly elevated IgE and eosinophilia (5 and 7 patients, respectively) (Table 2). None of the patients demonstrated reduced Th17 lymphocytes. In three of them TH2 values were above the established reference ranges.
Next, we analysed the diagnostic usefulness of the developed reference ranges. For this purpose we calculated the negative and positive predictive values (NPV, PPV), and sensitivity of Th2 and Th17 identification according to generally accepted formulas. Considering that in our model none of the patients from either AD or MD group was found to have reduced Th17 cells, discrimination between STAT3 DN and other types of dermatitis used in our model was associated with 100% PPV, 97% NPV, and sensitivity of 92%.
Th2 above the established age-related reference ranges were identified in 14 patients from the AD group as well as 3 patients from HIES and MD groups. As result, the elevated Th2 was associated with 68% PPV, 71% NPV, and 74% sensitivity for diagnosing AD.
Discussion
Dermatitis belongs to the most common clinical manifestations of several diseases such as allergy affecting up to 20% of all children. Cutaneous inflammation may also accompany potentially lethal conditions, such as some primary atopic disorders [22]. In most cases, symptoms are observed during the first 5 years of patient’s life [23]. Although AD is usually diagnosed clinically [24], complex mechanisms of skin immunity, variability of atypic phenotypes [6, 25] and similarity to conditions resulting from different pathomechanisms may cause a significant delay in establishing the diagnosis of potentially lethal disease.
Hyper-IgE syndrome (Job’s syndrome) (MIM #147060), caused by dominant negative mutations in the STAT3 gene (MIM #102582), is the prototypic monogenic disease with leading skin manifestations, elevated serum IgE, and eosinophilia [26, 27]. Diagnostic criteria for the disease, the so-called NIH and STAT3 scores, are based mostly on clinical features. Many of them are not associated directly with the immune system. Non-immunological manifestations, such as characteristic facial dysmorphia, scoliosis, retained primary teeth, joint hyperextensibility, bone fractures after minimal trauma, craniosynostosis, might not be demonstrated in very young children [11]. Cutaneous manifestation may accompany or precede dangerous symptoms, such as malignancy [12, 28], or fatal bacterial or fungal infections [12, 29]. For these reasons, timely diagnosis and initiation of appropriate treatment is of utmost importance.
According to current recommendations, the diagnostic workup of inborn errors of immunity associated with allergy and atopy include inter alia evaluation of Th2, Th17, and circulating follicular T helper cells [6]. Until recently, the methods of their enumeration were laborious and poorly applicable in routine daily patient’s work-up. Identification of effector T helper subsets based on differential expression of selected chemokine receptors was described a while ago [30], but lack of age-related reference ranges applicable to the paediatric population limited the practical use of this approach. This study has been initiated to determine age-related reference ranges for individual cytokine-producing T helper lymphocyte subsets, as well as to verify their usefulness in clinical environment. For this purpose the authors chose patients assigned to either of two model diseases: Job’s syndrome (HIES group – 12 patients with molecularly confirmed disease-causing mutation in the STAT3 gene) and AD, diagnosed according to widely accepted criteria [7]. The ability to discriminate between both groups of patients was additionally verified in 9 very young patients with mixed atopic and seborrheic dermatitis. Scores used for the diagnosis of Job’s syndrome [12, 13] were defined for all patients from the study cohort.
The generally accepted NIH score above 30, a criterion considered diagnostic for HIES, was not met by 1 patient with confirmed molecular diagnosis of Job’s syndrome. Four patients did not meet Woellner’s criteria [13]. This means that the NIH score as a diagnostic criterion of HIES was associated with 92% PPV, 96% NPV, and 92% sensitivity – similar to evaluation of Th17 in the context of the developed reference ranges. Woellner’s criteria on the other hand were associated with 89% PPV, 89% NPV, and 67% sensitivity. Such results cannot be considered unexpected in the paediatric population, as the criteria used to calculate the scores are based on symptoms that can be verified mostly in older children [13]. In the authors’ opinion, neither NIH nor STAT scores are sufficiently sensitive to offer young patients a timely diagnosis and introduction of an appropriate treatment. Such insensitivity seems to be corrected by evaluation of Th17 lymphocytes.
The study was performed in two directions: testing healthy subjects to develop normal reference ranges and verification of the results in the context of available data from the literature and in terms of clinical usefulness. The development of normal age-related reference values for the analysed cell subsets required collection of samples from healthy control subjects. These have been extremely carefully selected in terms of the history of allergy, atopy, dermal lesions, or immunological dysregulation. The numbers of patients in individual age groups might not be considered fully satisfactory. However, the inclusion criteria for healthy controls have been set up very strictly, in order to make them reliable. It must be taken into consideration that nowadays it is extremely difficult to find absolutely healthy people, off any medication, without any signs of allergy or atopy (affecting a large population of otherwise healthy people) or infections in younger children. Despite these drawbacks, we were able to confirm general observations regarding age-related changes in distribution of Th1, Th2, and Th17 subsets [31–33], with increasing-with-age proportions of Th1, Th2, an Th17 [31–33] (Figure 1) and Th2 skewing in small children [34] (Figure 2).
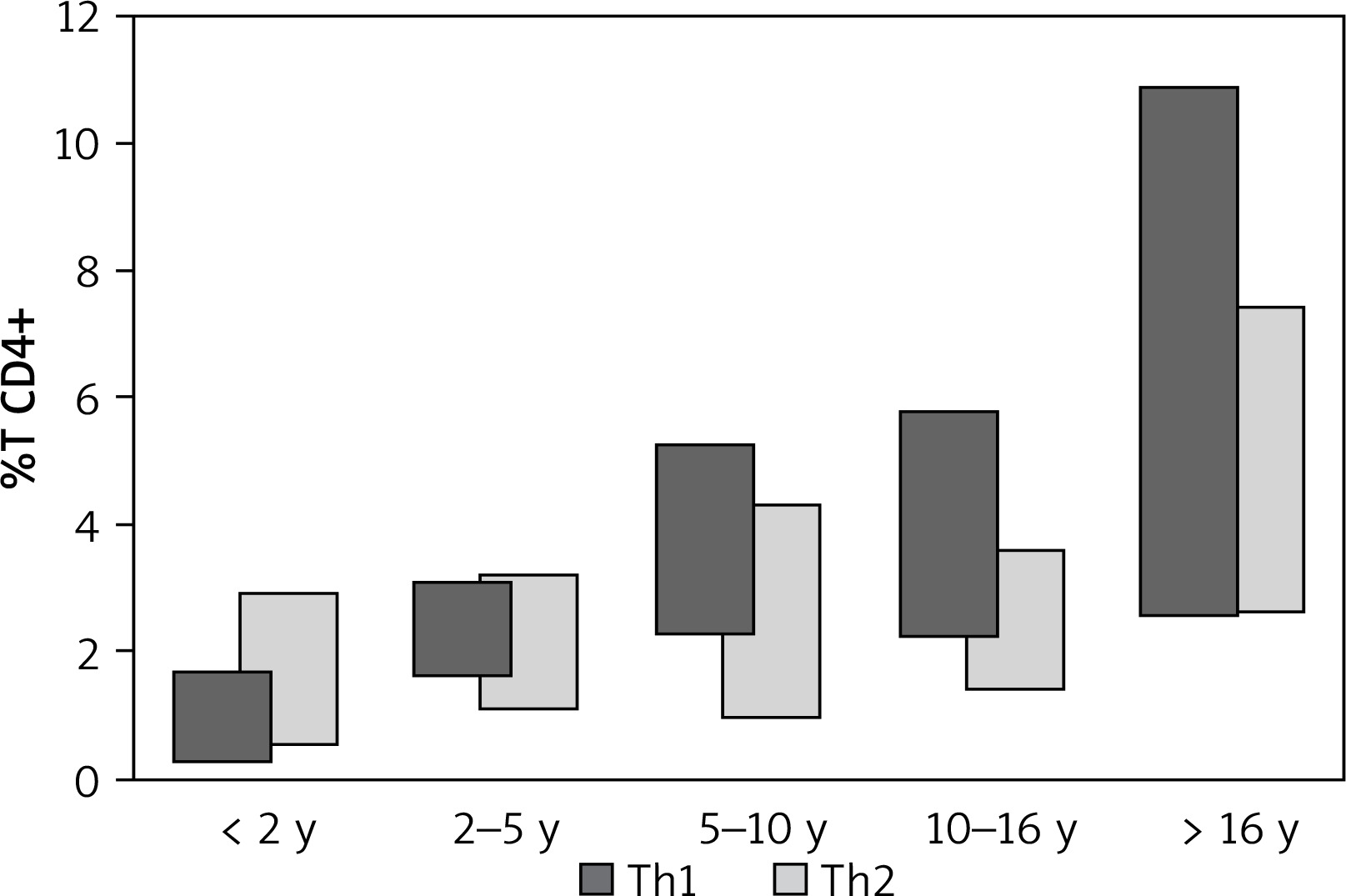
Figure 2
Comparison of Th1 and Th2 in healthy controls across analysed age groups. Th2 compose a more numerous population than Th1 in very young children (below 2 years of age), resulting in low Th1:Th2 ratio in this age group. Both populations become more numerous with age, but at a different rate, resulting in with increasing with age Th1:Th2 ratio
Although we have not found detailed data on Th9, Th17.1, or ThG distribution in healthy people, the obtained results seemed logical. It has been demonstrated that IL-22 producing T helper cells are present in peripheral blood and that they compose a small population [33] – this observation has been confirmed in our healthy control group. Explanation of reduced proportions of Th22 in patients 2–5 years old however needs further studies. We have no explanation for a similar observation in relation to ThG cells, as to our knowledge there are no studies in this field.
During the course of this study, we have identified only one paper referring to normal age-related reference ranges in children, with a similar approach to identification of cell subsets as in our study [35]. The reported age groups were comparable or even less numerous, with data referring to children below 2 years of age based on results obtained in samples from 2 children. Moreover, results have been presented only in the form of absolute cell counts [35]. Such an approach may be sometimes misleading, especially in children, due to e.g. lymphopenia or lymphocytosis secondary to various conditions.
The second part of the study aimed at verification of the clinical applicability of the developed reference ranges. Results in the study group confirmed reports of universal reduction of Th17 in HIES patients [26, 28, 36], but also allowed to demonstrate a similar reduction in TFH17 cells and slightly lower association with Th9 reduction.
In 2019, Zhang et al. published a paper describing reduction of Th9 in patients with Job’s syndrome and demonstrating the role of STAT3 and IL-21 production in human Th9 differentiation [37]. This observation was confirmed in 9 patients from the HIES group. Th9 were reduced also in 2 patients from the AD group. One of them had NIH score of 26 and Woellner’s score of 18.32, which are below the previously set diagnostic cut-offs. Nevertheless, screening for a mutation in the STAT3 gene produced negative results. Considering that there were no other clinical indications suggesting Job’s syndrome, the patient was diagnosed as suffering from AD and despite normal Th2 lymphocytes received anti-IL-31Rα treatment at the age of 11 years. Positive response confirmed that his disease was associated with Th2 response. Only 1 patient from the MD group demonstrated marginally reduced Th9, but none – reduced Th17.
We were also able to confirm indirectly the observation published by Ma et al. [38] that generation of TFH cells is dependent on STAT3, as TFH17 deficiency was observed in all patients with reduced Th17. However, the development of TFH17 must be dependent also on other mechanisms that have not been analysed in this study, as they have been reduced also in 4 patients with AD and one with MD. Considering therefore 69% PPV, 96% NPV, and 92% sensitivity for reduction of TFH17 as characteristic for HIES, this parameter could be used only in the context of its high NPV.
The analysis of the relationship between aberrant levels of effector cell subsets and applicability of the developed normal age-related ranges for effector T helper cell subsets, produced in authors’ opinion at least satisfactory results: most patients from the AD group (13 of 19) demonstrated elevated Th2, as expected [39], while most from the HIES group – reduced Th17 [13]. The single patient with normal Th9, Th17 may belong to a scarce group of patients that do not demonstrate Th17 deficiency [40]. Allergy diagnosed in 3 patients from the HIES group (HIES3, 8, 10) might probably explain the elevated Th2 subset. Severe atopic lesions observed in HIES3 patient, or invasive aspergilloma experienced by HIES8 patient [41] also might contribute to Th2 elevation.
It is widely accepted nowadays that AD is a multifactorial disease, and that the patients may present with varying phenotypes. Most recent treatment guidelines for atopic eczema [42, 43] describe drugs used in treatment of the disease in correlation with the mechanism of their action. Some patients may require different treatment than others. In this context results of cytokine-producing T helper cell distribution may offer explanation why some patients will or will not benefit from a given therapy. The observation that as many as 14 patients from the AD group, but only two from MD or one in STAT3 groups, were found to have elevated ThG cells, may demonstrate the role of GM-CSF in inflammatory responses [44]. It may be therefore suspected that this group of patients might benefit from treatment with namilumab or other anti-GM-CSF treatment [44].
Evaluation of cytokine-producing cells has a long history in immunological laboratory diagnostics. Irrespective of the method of their identification, interpretation of results requires normal reference ranges. Having in mind that similar skin conditions might have different molecular background and long-term consequences, lack of widely available molecular diagnostics may significantly affect patient prognosis. Therefore, we need a fast, easy, available, reliable, and preferably cheap laboratory surrogate method to introduce patient-tailored treatment. This characteristic is met by determination of effector T helper subsets by flow cytometry and has been applied in several studies. Interpretation of results required however normal ranges, which were either absent, based on limited data, or provided retrospectively. Such an approach may be applied in research studies, but clinical diagnostics requires day-to-day analysis of results. This is difficult when normal reference ranges are not available. Multiple studies reported an age-related variation in Th1 and Th2, but few refer to Th17 reported to increase in adults [33] or in older age [31]. Data on other T helper cell subsets are even less available. We have demonstrated that even though the tested age groups were not numerous, the interpretation of the defined age-related normal subset ranges brought quite good discrimination between Job’s syndrome and other patients from the applied model. It must be however kept in mind that high PPV for Th17 reduction in HIES based on the presented results must be interpreted with extreme caution due to a limited number of subjects in the healthy group. Nevertheless, testing more healthy subjects is still worth further studies to make the data more reliable, and perhaps to find explanation for unexplainable at the moment reduction of ThG and Th22 in the prepuberty period. For this purpose, it would be wise to combine efforts from several laboratories. Such collaboration would help to develop reference ranges based on large groups of healthy subjects, meeting the same strict conditions as applied in our study.
All efforts have been made to create homogenous study groups, but we cannot fully exclude the effect of treatment on results of the analysed cell subsets. All HIES patients were on co-trimoxazole prophylaxis, including 1 patient who received voriconazole for severe lung condition. None of the patients from AD or MD study groups received systemic treatment, but all were treated with various topical drugs, including steroids and cyclosporine. None of these drugs could be withdrawn for ethical reasons.
Conclusions
We have confirmed that the presented method of Th17 and other effector cytokine-producing cell subset identification and interpretation of results in the context of age-related reference ranges defined during this study offers comparable and reliable results that can be used for discrimination of STAT3 and non-STAT3-deficient patients. We have also confirmed that Th9 and TFH17 cell development is impaired in most patients with Job’s syndrome. In order to improve the diagnostic rate and shorten the delay in obtaining the diagnosis we would suggest evaluation of other than Th17 cell subsets in combination of NIH and Woellner’s criteria, having in mind that in young children several clinical features may not be demonstrated. Moreover, we suggest that individual results of effector T helper cells distribution might probably be useful in selection of potentially most effective biological treatment.







