
Actinic keratoses (AK) usually present as multiple, erythematous, or yellow-brown, dry, scaly lesions in the middle aged or elderly. Acantholytic actinic keratosis (aAK) is a rare histological subtype and has been regarded as a precursor of acantholytic squamous cell carcinoma (SCC) [1, 2]. Here, we present a rare case of acantholytic actinic keratoses on the face.
A 73-year-old woman came to our hospital and presented with a 2-year history of erosive and crusted lesion/lesions on her right face. The patient was a farmer with no pre-existing medical conditions. Physical examination showed an erosive erythema with numerous scabs and scales on the surface. A red halo and pigmentation can be seen around the lesion (Figure 1 A). Dermoscopic examination showed erythema forming a pink-reddish vascular pseudonetwork surrounding hair follicles, yellowish-white scales, thin and wavy vessels surrounding the follicles, and follicular openings filled with keratotic plugs (Figure 1 B). These structures conformed to the typical “strawberry” pattern of AK. The histologic examination of a skin biopsy revealed well-circumscribed abnormal epidermal thickening with extensive hyperkeratosis and parakeratosis (Figure 2 A). Epidermal acantholysis with diffuse atypia of keratinocytes involved the spinous layer and granular layer. Obvious elastotic degeneration in the dermis with lymphocyte infiltration was observed (Figure 2 B). Based on history and histological features, a diagnosis of aAK was made. Surgical debridement was complete and followed by aminolaevulinic acid-photodynamic therapy (ALA-PDT) every 2 weeks. Complete regression was obtained after 5 sessions, with no recurrence in the following 12 months.
Figure 1
A – Clinical appearance of the patient. Erosive erythema with numerous scabs and scales on the surface. A red halo and pigmentation can be seen around the lesion. B – Dermoscopic image of the “strawberry” pattern observed in the lesions
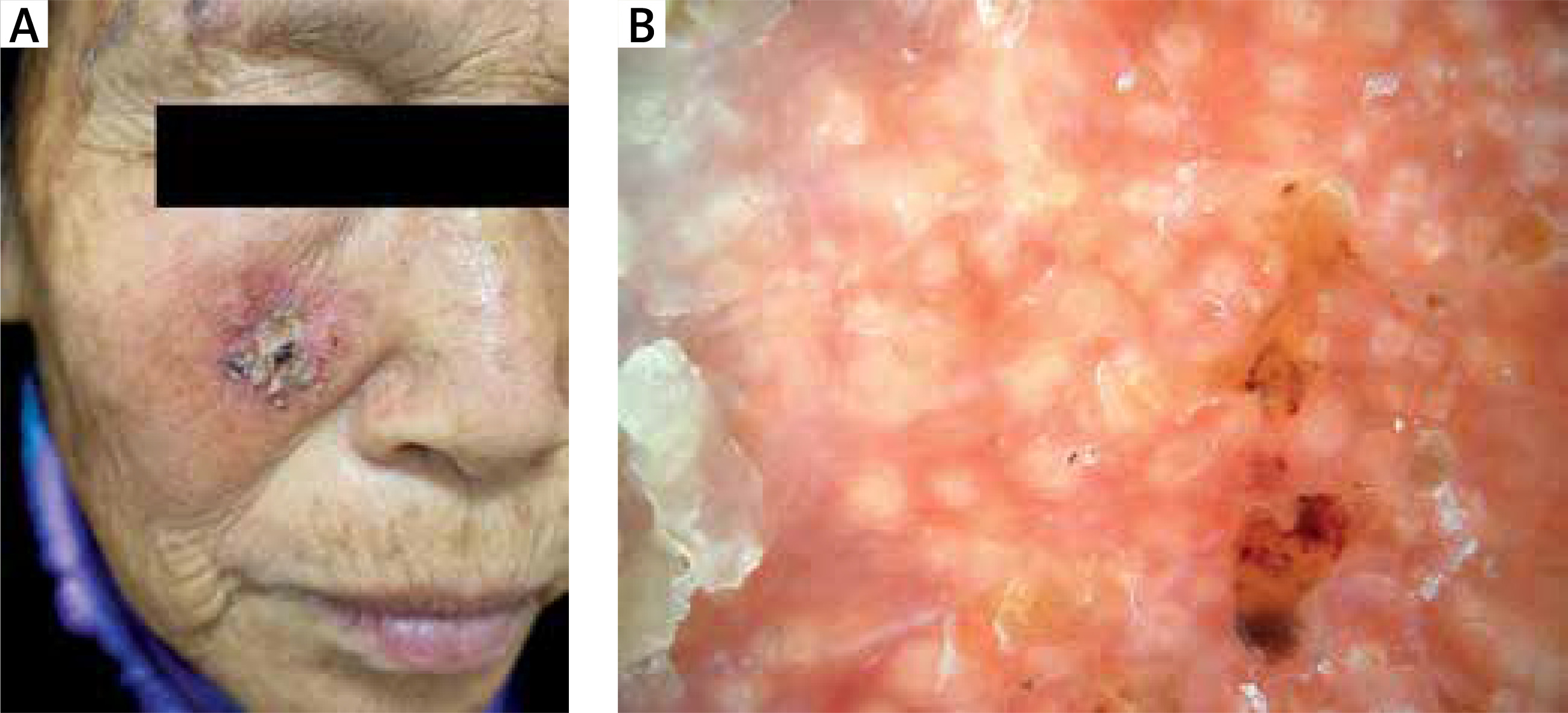
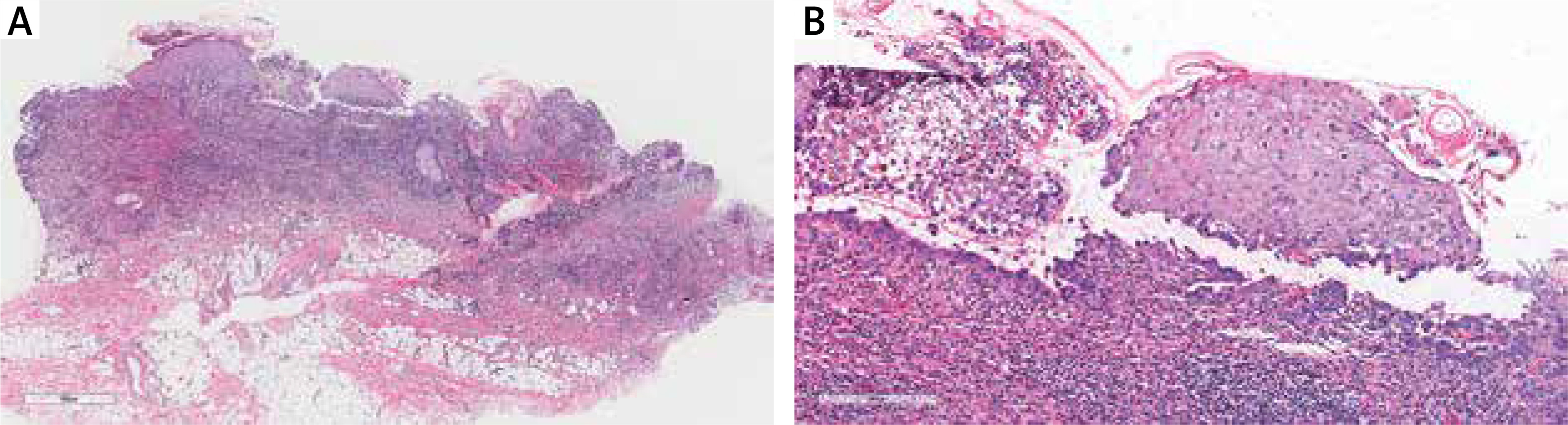
Figure 2
Histopathologic findings of the lesion. A – Well-circumscribed abnormal epidermal thickening with extensive hyperkeratosis and parakeratosis (H&E stains, original magnification ×40). B – Epidermal acantholysis with diffuse atypia of keratinocytes involved the spinous layer and granular layer (H&E stains, original magnification ×400)
AK mostly develops as a consequence of long-term UVR exposure in the susceptible elderly individuals [1]. It is characterized by dysplastic epidermal lesions that have the potential to progress to cutaneous SCC. A frequently seen subtype is the hyperkeratotic AK. Acantholytic AK is an uncommon pathological type of AK [1]. It is characterized by marked acantholysis, acantholytic or pseudoglandular pattern results, which may show a marked resemblance to lesions of Darier’s disease. Therefore, histology remains the gold standard for the diagnosis of aAK.
Clinically, aAK has no difference from any other type. They may be sharply demarcated and gradually transformed from lesional to normal skin. Histopathologically, all variants demonstrate keratinocyte atypia with disruption of normal maturation and loss of polarity, nuclear pleomorphism and hyperchromatism. Acantholytic AK demonstrate dyscohesion of keratinocytes within the epidermis, often appreciated/noted within downward buds of keratinocytes [1]. In our case, typical clinical findings suggest the possibility of AK, though further pathological examination is necessary to predict the prognosis.
Acantholysis is the loss of cohesion between keratinocytes as a result of dissolution of intercellular connections, sometimes resulting in an intraepidermal vesicle. The three major acantholytic disorders of the skin are Darier’s disease (DD), Hailey-Hailey disease (HHD), and Grover’s disease (GD) [3]. Acantholysis may occur in many epidermal inflammatory and neoplastic diseases, so it is not a specific phenomenon and needs to be carefully identified. Acantholysis in cutaneous tumours is often caused by rupture of the desmosomal junctions associated with absence of normal molecules on the surface of tumour cells. Some literature suggests that acantholysis is a precursor of progression and malignancy of skin tumours, so close follow-up is critical in this pathological pattern of diseases [3].
Options for therapy of AK include chemotherapeutic agents, surgical procedures, and photodynamic therapy [4]. Biopsy may be indicated if a lesion has not responded to more conservative therapy, if the dermatologic surgeon is concerned that a lesion may truly represent SCC, or if it is deemed that the cosmetic result warrants the procedure. ALA-PDT has an excellent therapeutic effect while potentially preventing the recurrence of AK [5].
In conclusion, we presented this rare case with such distinctive features in order to strengthen awareness of this rare variant and highlight the early biopsy of asymptomatic skin lesions in elderly patients.







