
Purpose
Primary and recurrent malignancies of the vagina, vulva, or urethra are rare diseases [1], with approximately 70 women diagnosed per year in Australia [2]. Treatment with surgery is difficult due to proximity of organs at risk. The American Brachytherapy Society have provided guidelines or consensus documents for treating primary vaginal disease [1] and salvage treatment for endometrial recurrences [3]. Brachytherapy (BRT) has been shown to be beneficial for local control for both primary [1, 4-12] and recurrent [5-9, 13-19] disease of the vagina, with acceptable risk of toxicity.
External beam radiotherapy (EBRT) with a brachytherapy boost is recommended due to risk of lymphatic involvement [20], although there are reports of a single-modality being used [11, 15, 21, 22]. Higher EQD2 total doses were delivered with external beam radiotherapy, followed by a brachytherapy boost [15]. External beam radiotherapy also reduces the volume of gross target prior to brachytherapy. Patients who received combined EBRT and BRT presented with better overall survival [3, 15]. Also, local control was found to be favorable with combined EBRT and BRT [23, 24]. Brachytherapy (alone or in combination with EBRT) was reported to benefit overall survival compared with EBRT alone [25].
Recommendations from the published literature can be summarized as follows: 1. For disease depths less than 0.5 cm, intracavitary brachytherapy is suitable, and 2. Thicker lesions require interstitial brachytherapy [4]. If an intracavitary approach is used, multiple channels work better than single-channel vaginal cylinders [26]. Intracavitary brachytherapy can be delivered using either single- or multi-channel applicators; however, single-channel applicator usage is limited for vaginal cancers due to inability to effectively shape the dose [27]. Albano et al. [28] described a method for taking a mould of the vagina to manufacture a customized applicator for intracavitary brachytherapy. Interstitial brachytherapy can be delivered using either a free-hand or template technique [1, 15, 22]. Additionally, combined interstitial and intracavitary brachytherapy has been used for vaginal cancers.
Dosimetric comparisons of interstitial and multi-channel vaginal applicators have found that interstitial brachytherapy provides lower doses to organs at risk, but for circumferential disease, multi-channel vaginal applicators deliver a better dose to vaginal mucosa [30, 31].
Magnetic resonance imaging (MRI) and 3D planning are recommended for planning vaginal brachytherapy [27]. Organ at risk toxicity for gynecological brachytherapy has been extensively studied in the setting of cervix cancer. Dose-volume histogram parameters, such as D0.1cc, D1cc, and D2cc, have been found to be predictive of toxicity, including correlation with a grade of toxicity [32-37]. Kasibhatla et al. recommended limiting a rectal dose to less than 76 Gy for interstitial brachytherapy for advanced gynecological malignancies [38]. Severe urethral toxicity has been correlated with D0.1cc [39]. Sigmoid toxicity is usually not a concern for vaginal brachytherapy, due to the distance between recto-sigmoid junction and the vagina. Murakami et al. found that re-irradiation and vaginal D2cc were significant predictors of vaginal ulcers in interstitial brachytherapy for gynecological malignancies [40].
This report presented a single-institution’s pattern of practice, dosimetry results, and clinical outcomes for patients with unresectable malignancies of the vagina, vulva, or urethra, receiving brachytherapy delivery using customized vaginal moulds with or without interstitial needles.
Material and methods
Following an examination under anesthesia and often an MRI, patients received pelvic external beam radiotherapy. During the initial examination under anesthesia, most of patients received gold seeds to mark the size and location of the original tumor.
External beam radiotherapy was delivered using either a 4-field box conformal technique with 18 MV or volumetric arc radiotherapy, using either 6 MV or 10 MV. The prescriptions were 45-50.4 Gy in 25-28 fractions. Two patients (of 21 reviewed) had previous radiation treatment to the pelvis and did not receive external beam radiotherapy prior to their brachytherapy. One of these patients had previously had an unrelated rectal cancer, with external beam radiation (50 Gy/25 fractions, 22 months previously). The other had a vaginal cylinder brachytherapy following primary endometrial cancer (21 Gy/3 fractions, prescribed to a depth of 5 mm, 5.5 years previously), and was then treated again for a recurrence.
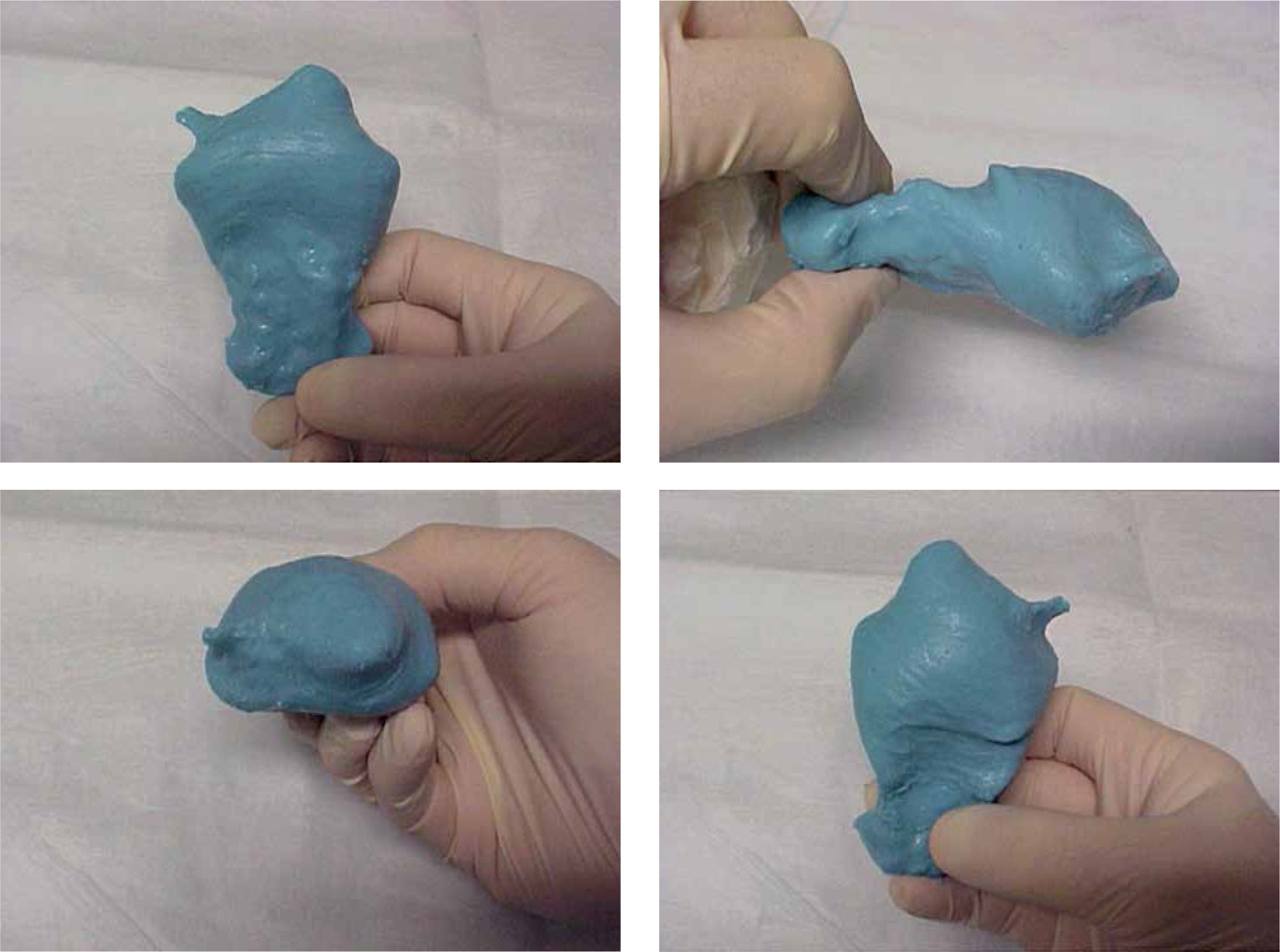
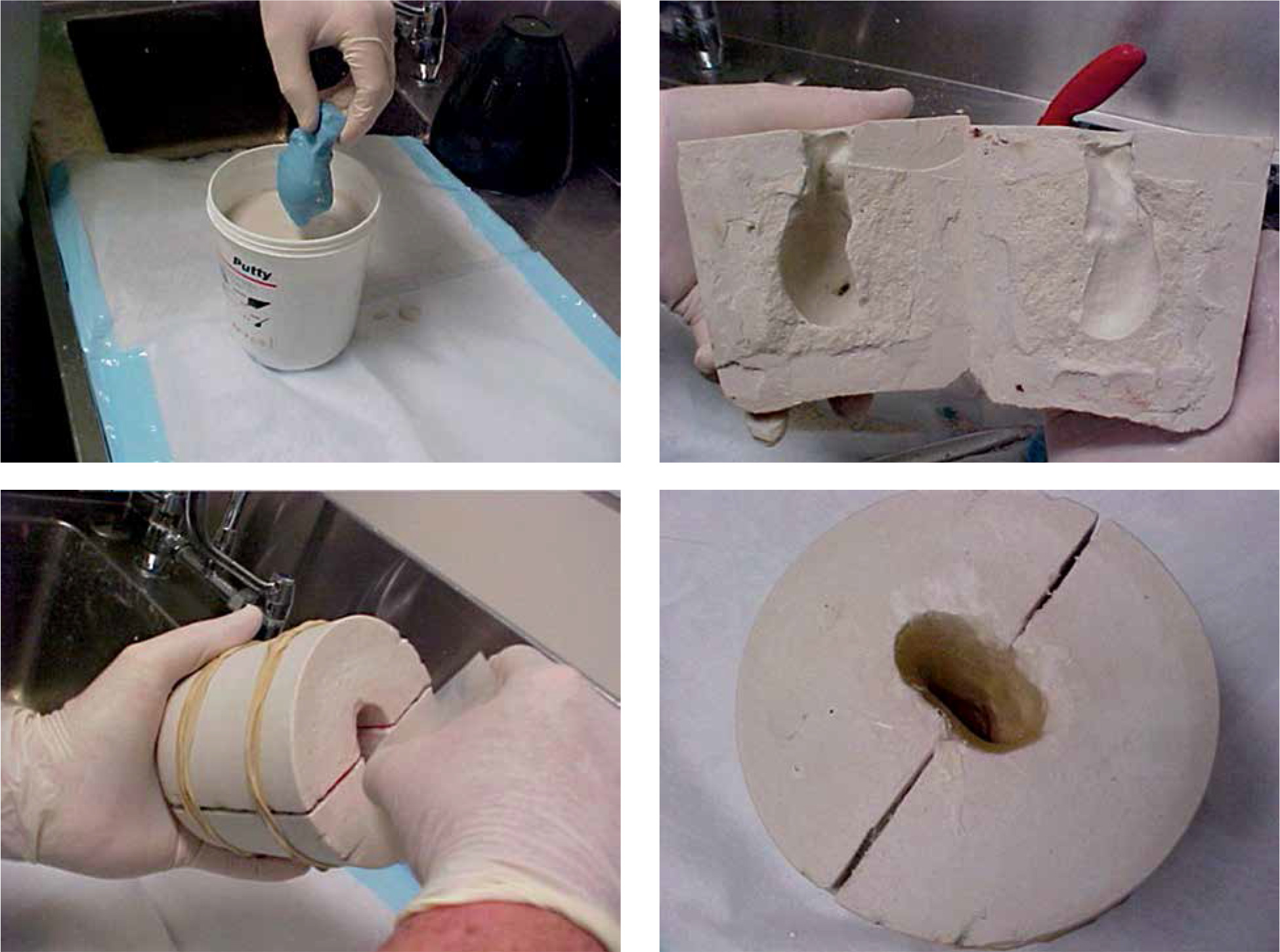
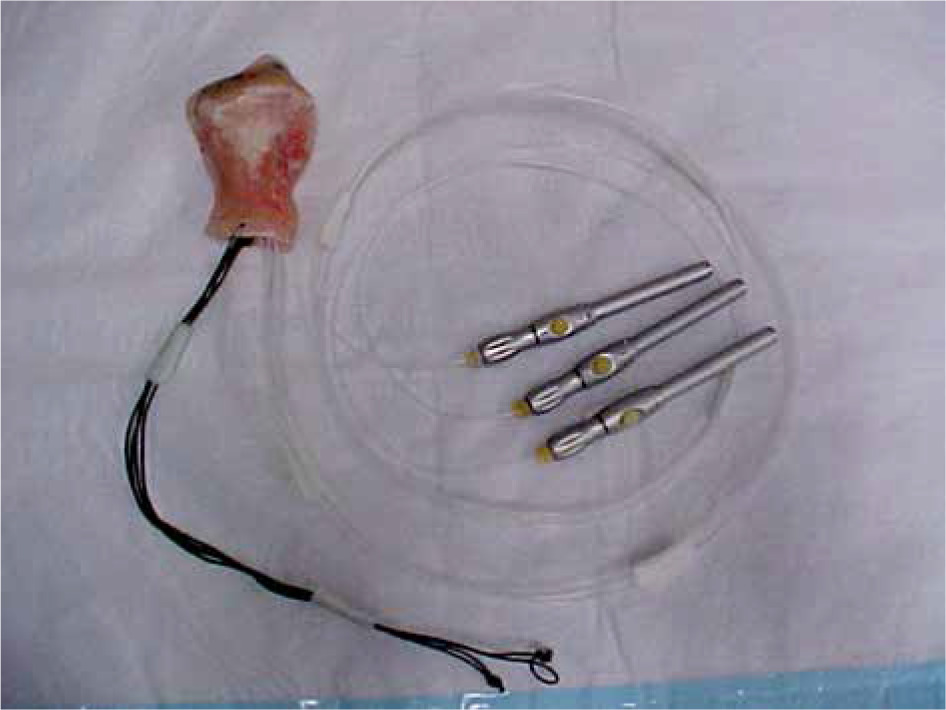
Brachytherapy was performed as a boost, following external beam radiotherapy. The patient was anesthetized, and an examination was performed. A mould for a customized applicator was made using a similar technique, as described by Albano et al. [28]. Dental alginate was applied to form an impression of the vaginal canal (Figure 1). This mould was then placed in quick setting gypsum plaster. Then, the plaster mould was used to create a thin acrylic applicator shell conformal to the vaginal canal. 4.7 French catheters were inserted into the acrylic mould in such a way, as to enable the dose distribution to be conformal to clinical target volume. Wax filling was applied to stabilize the catheters within the mould. Figure 2 shows a mould construction process. Figure 3 presents a completed customized applicator.
Whenever required, interstitial needles were placed along the lateral vaginal wall near the clinical target volume, using a free-hand technique. Interstitial needles were inserted prior to the mould, so the oncologist could palpate the path of needles from within the vaginal canal. The mould was inserted into the patient and surgically stitched into place.
After recovering from anesthetic, the patient had a computed tomography (CT) scan at which, radio-opaque CT marker wires were inserted into all channels within the mould and needles. If MRI was required (and not contraindicated), the markers were removed prior to imaging. MRI was not performed if there was a lack of residual tumor evident during the examination under anesthesia, or if MRI was contraindicated for the patient. T2 fast spin echo sequences were performed with axial, sagittal and coronal planes.
CT and MR images (if applicable) were fused using rigid image registration, matching the mould applicator, needles, and gold seeds. Organs at risk and clinical target volumes were delineated on MRI (if available, otherwise CT), whilst CT was used for an applicator reconstruction.
Using BrachyVision (Varian Medical Systems, Palo Alto, USA), a plan was generated to deliver a prescription dose to clinical target volume (CTV) D90% ≥ 75 Gy total dose EQD2, while maximizing conformity and limiting the dose to organs at risk, with dose constraints to D0.1cc and D2cc of the bladder, rectum, and sigmoid-colon, and D0.1cc to the urethra. Dwell time optimization was performed using a combination of volumetric and/or graphical optimization techniques. Dose formalism described by the American Association of Physicists in Medicine Task Group 43 was applied for dose calculations [29]. Total EQD2 bladder and rectum planning objectives were D2cc ≤ 90 Gy and D2cc ≤ 75 Gy, respectively.
After a quality review, the plan was approved by a radiation oncologist, and treatment was delivered using a Varisource iX (Varian Medical Systems, Palo Alto, USA). The patients usually remained in hospital overnight and two additional fractions were given the following day (if four fractions were applied, patient stayed two nights), allowing a minimum of six hours between fractions. A combination of verification measurements, including protruding needle length, verification CT scan, and fluoroscopic imaging were performed prior to each additional fraction as appropriate for each case.
For this audit, medical records of the patients were accessed to determine treatment response, disease recurrence (local or distant), and toxicity as well as dosimetric data, such as CTV D90 and D98 for bladder and rectum D2cc and D0.1cc, and urethral D0.1cc. Dose homogeneity within CTV and dose conformity were calculated using dose homogeneity index (Eq. 1) [41] and simplified conformity index (Eq. 2) [42].
Where DHI was the dose homogeneity index, VCTV,150 was the volume of the CTV that receives 150% of the prescribed dose, VCTV,100 was the volume of the CTV that receives 100% of the prescribed dose, CI was the conformity index, VCTV was the volume of the CTV, and Vref was the volume of the 100% isodose.
Results
Twenty-one consecutively treated patients were reviewed, following a treatment between 2010 and 2018. Table 1 shows details of diagnoses for the patients’ cohort of this study. The mean follow-up was 4.0 years (range, 1.6-9.2 years), and the mean age was 70 years (range, 54-88 years).
Table 1
Diagnosis for patients treated with customized mould and/or needles
| Number of patients | Diagnosis |
|---|---|
| 11 | Endometrial recurrence |
| 7 | Vagina primary |
| 1 | Cervix recurrence |
| 1 | Urethra primary |
| 1 | Vulva primary |
Ten patients were treated using only channels within the customized mould. For eleven patients, free-hand interstitial needles were used in addition to the channels within the mould. For one patient, all dwell positions were in interstitial needles, with the customized mould being used only to stabilize the vaginal anatomy. The average number of channels per patient was 5, with a range of 2-12 (including interstitial needles). When interstitial needles were required, either 2 or 3 needles were inserted.
Six patients were planned using CT imaging only, and the remaining patients had CT and MR imaging for planning. CT enabled catheter reconstruction within the mould.
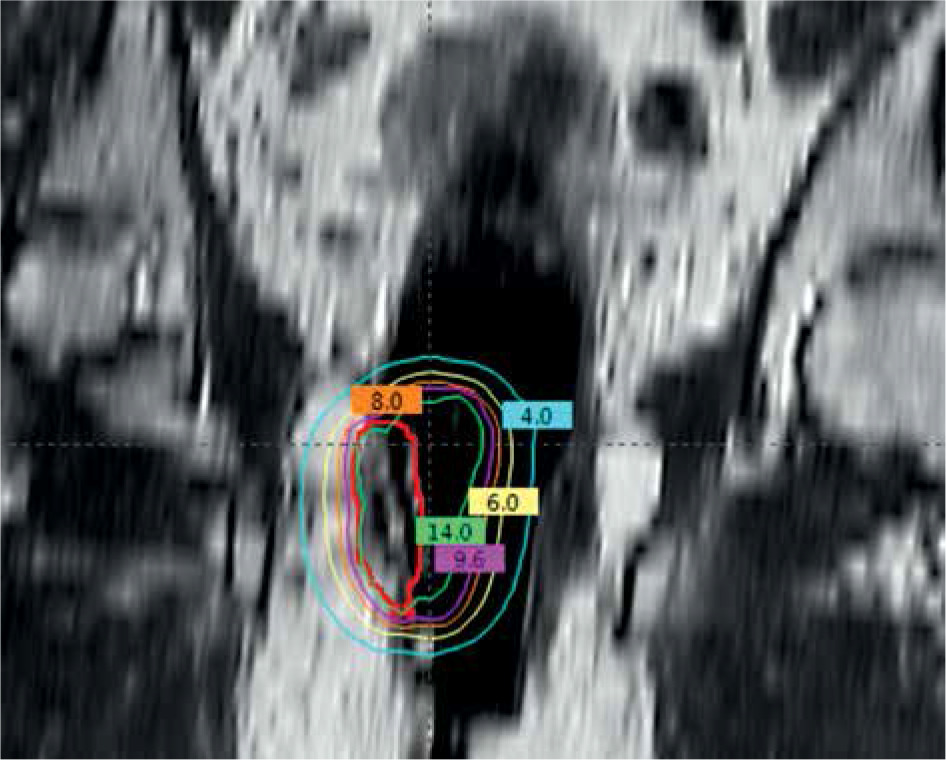
EQD2 values were calculated assuming an α/β ratio of 10 for target volumes and 3 for late responding normal tissue. Sixteen patients were treated over three fractions and five patients received four fractions. The average CTV volume was 14.3 cm3 (range, 1.5 cm3 to 47.3 cm3). CTV and organ at risk plan quality metrics (PQM) and toxicity are presented in Table 2. Figure 4 shows an example of an MR image with the customized applicator, CTV, and isodoses.
Table 2
Plan quality metrics and toxicity
Fig. 4
A frontal view showing an MR image with customized applicator in situ. Clinical target volume (CTV) is displayed with red contour, and isodoses are also shown
Local disease control was achieved for 67% of the patients. Disease-related adverse outcomes included two incomplete responses, leaving residual vaginal tumor and local recurrences in five patients, and one out of field recurrence in the groin. One of the local progression cases died 28 months after brachytherapy. One patient with a recurrence had a vaginal resection and continues to remain disease-free at 31 months.
It can be assumed that the vaginal mucosa proximal to CTV received the prescribed dose. Two patients developed vaginal ulcers, one responded to hyperbaric oxygen therapy, one resolved with time, and 10 patients reported mild vaginal telangiectasia, fibrosis, or stenosis.
Two of the patients in this series had previous pelvic radiation treatment. One received a prophylactic cylinder brachytherapy treatment of 21 Gy in 3 fractions, and one had previous EBRT for a rectal carcinoma.
Discussion
Using a combination of customized molded applicators and free-hand interstitial needles, acceptable doses to both the target and organs at risk were achievable. Given the challenging anatomical positions of some of these tumors, combined with limitations of curvature in the source path, there were often very limited dwell positions that could be used to deliver the dose, which affected the conformity of the doses around the small volumes.
Ideally, a direct dosimetric comparison of a multi-channel applicator plan using the mould technique would be performed as a planning study to determine which of the two gives the highest quality of the plan. However, this was not achievable with the data available, as the shape of the vagina was different between the two types of insertions.
There are many uncertainties related to brachytherapy for vaginal malignancies. Given the rarity of these tumors, most data comes from small single-institution studies. This leads to a lack of consensus for prescription doses and fractionation as well as contouring uncertainties. A range of practice related to contouring clinical target volumes for recurrent endometrial treatment has been reported, including variation in reporting and prescription to CTVs and variation with different imaging techniques (CT and MRI) [3].
Two patients in this series had a history of previous pelvic radiotherapy. Sadozye et al. [43] reviewed re-irradiation in the setting of recurrent gynecological cancers and concluded there were significant uncertainties regarding treatment modality and doses in this setting. Kamrava et al. [3] suggested that there were greater uncertainties in a re-treatment setting as well as higher risk of toxicity and overall worse outcomes [3]. Yoshida et al. [44] reported higher vaginal mucosa reactions for re-irradiation. A single-institution audit of re-irradiated gynecological malignancies found that it gave a reasonable chance of long-term local control and acceptable organ at risk toxicity [14]. Whilst not statistically significant, the two patients in the current series who developed vaginal necrosis were the two who previously received radiotherapy to the pelvis. Ling et al. [45] concluded that if OAR doses were limited, successful salvage could be achieved for 40% of patients with recurrent vaginal disease, similar to the results reported in this series. Raziee et al. [46] found that re-irradiation provided a safe and effective salvage option for over a quarter of patients.
The most significant prognostic factor was reported to be the FIGO tumor stage, with other prognostic factors being the size and location of tumor [11]. Higher doses have been shown to improve local control for recurrent endometrial cancer [47-50]. 3D image guidance also seems to be assisting in local control outcomes [13, 51, 52].
Chronic side effects from radiotherapy for vaginal cancers are relatively rare. Grade 1-4 side effects have been reported for bladder and rectum at ≤ 2% and up to 6% for vaginal side effects [11]. Moreover, dilator use has been shown to decrease vaginal stenosis [53, 54].
There are also different methods reported to produce customized moulds. Nilsson et al. used a two-part putty [55]. However, further work is warranted investigating the use of 3D printing in the treatment of vaginal malignancies [56, 57].








