
We present a case of a right heart catheterisation following a transcatheter bicaval valve implantation in a patient with persistent NYHA class II-III heart failure 6 months after a TricValve device implantation. Evaluation from the femoral access confirmed normal venous pressure without significant persistent V-wave in the inferior vena cava (IVC). Measurements of superior vena cava (SVC) were performed trough a left basilic vein access. Jugular or right upper limb access were not available in the patient because of a history of high-dose chest radiation. A Swan-Ganz catheter was advanced through the struts of the prosthesis (Figure 1). Simultaneous registration of right atrium (RA) pressure from femoral vein access and SVC from left basilic vein access confirmed the persistence of elevated V-wave in SVC pressure and that it was influenced by dysfunction of the superior prosthesis rather than catheter interference. This prosthesis dysfunction may have been responsible for elevated pressure in the SVC exceeding that of the RA. There was no evidence on physical examination to suggest the development of superior vena cava syndrome. The minor V-wave measured in the IVC explains the reduction in lower extremities oedema and hepatic congestion in the patient. It is probable that a longer duration of treatment is necessary to achieve greater neurohormonal blockade and sustained reduction in right-sided pressures, thereby facilitating improvement of symptoms such as dyspnoea [1–3].
Figure 1
A – 1. Assessment of the superior cava valve through superior access. 2 – Evaluation of the inferior cava valve via femoral access. 3 – Evaluation of the right atrium using both accesses. B – Indicated by arrow: assessment of the superior cava valve through the left basilic vein, advancing through the struts of the prosthesis
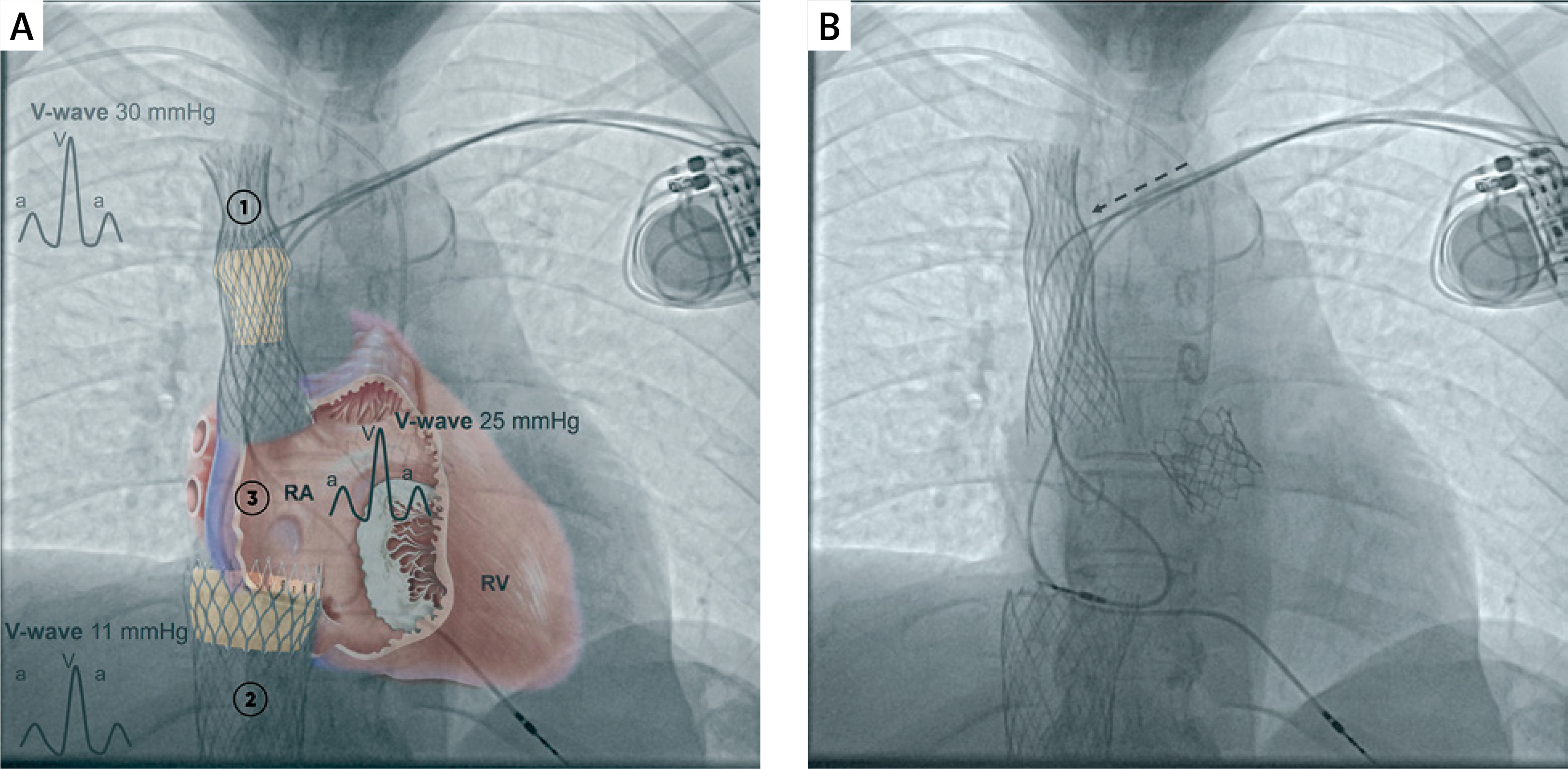
Our case highlights the importance of assessing both prostheses with double access, because a single femoral access does not allow to differentiate between catheter interference or valve disfunction. Therefore, we recommend measuring the V-wave in the SVC via superior access using a femoral access for the IVC, and the right atrium (refer to numbers 1, 2, 3 in the image).







