
Introduction
Adequate antiplatelet treatment is crucial for ischaemic risk reduction in patients following acute coronary syndrome (ACS). However, the recent real-world data reveal poor adherence to the guidelines-recommended approach in Poland.
Thus, we present here a comprehensive review of antiplatelet treatment in successive phases of ACS treatment: pre-hospital, in-hospital and post-hospital. We also report the up-to-date antiplatelets usage statistics from Polish registries to highlight the points of care which should be immediately improved.
The role of antiplatelet treatment in patients with acute coronary syndrome
The occurrence of an ACS is an independent factor for poor prognosis in both short and long term observation. In-hospital mortality due to ACS in Poland, in the years 2009–2012, was at the level of 10.5% (6.3% in patients undergoing percutaneous coronary intervention (PCI)), and mortality within 1 year after ACS was at the level of 19.4% (12.3% in the PCI treated group) [1]. The most common cause of death in this group of patients are recurrent cardiovascular events. The highest risk of adverse events, including recurrent myocardial infarction, is observed during the first months after ACS. The risk decreases gradually, reaching a plateau after about 3 years [2]. Stent thrombosis is responsible for 76.3% of the recurrent myocardial infarctions in a 30-day observation and for 43.2% of the cases in an observation from 1 to 36 months after the coronary event [3]. Other causes of recurrent ACS are: the rupture of atherosclerotic lesions other than the primary culprit lesion, in-stent restenosis or progression of the coronary artery disease. A higher proportion of recurrent myocardial infarction was observed in patients with the ACS treated conservatively [4].
An efficient way to reduce the risk of recurrent myocardial infarction is an appropriate antiplatelet therapy. The standard of care after ACS, regardless of the method of its treatment (invasive vs. conservative), is dual antiplatelet therapy (DAPT) with acetylsalicylic acid (ASA, loading dose of 150–300 mg orally, followed by a maintenance dose of 75–100 mg orally; ASA may also be administered intravenously (loading dose 75–150 mg)) and one of the adenosine diphosphate P2Y12 receptor inhibitors (Table I) [5]. According to the current guidelines, the antiplatelet drug of choice in ST-elevation myocardial infarction (STEMI) and non-ST elevation acute coronary syndrome (NSTE-ACS), in the absence of contraindications, should be one of the new P2Y12 inhibitors, i.e. ticagrelor or prasugrel (Class I A recommendation for STEMI; I B for NSTE-ACS) [6, 7]. Despite these recommendations, according to the Polish Registry of Acute Coronary Syndromes (PL-ACS), in 2018 clopidogrel was still the most commonly used P2Y12 inhibitor in Polish patients with ACS.
Table I
Characteristics of P2Y12 inhibitors available in Poland (modified on the basis of 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation [7])
| Parameter | Clopidogrel | Prasugrel | Ticagrelor |
|---|---|---|---|
| Chemical class | Thienopyridine | Thienopyridine | Cyclopentyl-triazolopyrimidine |
| Dosage | Loading dose 600 mg, then 75 mg/day | Loading dose 60 mg, then 10 mg/day | Loading dose 180 mg, then 90 mg twice a day |
| Dosage in CKD: | |||
| Stage 3 (eGFR 30–59 ml/min/1.73 m2) | No dose adjustment | No dose adjustment | No dose adjustment |
| Stage 4 (eGFR 15–29 ml/min/1.73 m2) | No dose adjustment | No dose adjustment | No dose adjustment |
| Stage 5 (eGFR < 15 ml/min/1.73 m2) | Limited data | Limited data | Limited data |
| Reversibility of combination | Irreversible | Irreversible | Reversible |
| Activation | Prodrug, with variable liver metabolism | Prodrug, with predictable liver metabolism | Active drug, with additional active metabolite |
| Onset of loading dose effecta [h] | 2–6b | 0.5–4b | 0.5–2b |
| Duration of effect [days] | 3–10 | 7–10 | 3–5 |
| Withdrawal before surgery [days] | 5c | 7c | 3–5c |
| Plasma half-life of active P2Y12 inhibitord | 30–60 min | 30–60 mine | 6–12 h |
| Inhibition of adenosine reuptake | No | No | Yes |
| Main contraindications | |||
It should be emphasised that ticagrelor and prasugrel have a stronger antiplatelet effect and less inter-individual variability in their potency [8, 9]. The PLATO trial showed that ticagrelor, compared to clopidogrel, reduces the risk of recurrent myocardial infarction by 16% (HR = 0.84 (0.75–0.95)), as well as death from any cause by 16% (HR = 0.84 (0.72–0.96)) in 1-year observation [8]. These evidence-based data seem to be confirmed in everyday clinical practice based on the Swedish SWEDEHEART registry, which showed in 2016 that in the group of patients with myocardial infarction the use of ticagrelor instead of clopidogrel was associated with a decrease in the risk of recurrent myocardial infarction by 11% (corrected HR = 0.89 (0.78–1.01)) and a decrease in the risk of death by 17% (corrected HR = 0.83 (0.75–0.92)) [10]. In the TRITON trial prasugrel was more effective than clopidogrel in reducing rates of composite primary end-point (death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke – HR = 0.81; (0.73–0.90); p < 0.001) [9].
However, it should be emphasised that the bleeding risk associated with the use of new P2Y12 receptor inhibitors is higher [8, 9]. Recently published results from a real-world, retrospective, large-cohort study conducted in US and Korea revealed that in a propensity-score matched population net adverse clinical events ratio (composite endpoint consisting of ischaemic events – recurrent myocardial infarction, revascularization or ischaemic stroke and haemorrhagic events – haemorrhagic stroke or gastrointestinal bleeding) did not differ between the ticagrelor and clopidogrel groups [11]. Among the secondary endpoints there were also no significant differences in the occurrence of ischaemic events, but haemorrhagic complications were significantly more frequent in the ticagrelor group. These inconsistencies between randomized trials, where ticagrelor was clearly better than clopidogrel, and carefully analysed data from real-world registries may have many reasons. One possible explanation is less precise P2Y12 inhibitor choice in everyday practice. For example, in the described real-word data analysis 3% of patients received a combination of ticagrelor and an oral anticoagulant, which is contraindicated according to the current guidelines. The other reason may be the higher rate of new generation P2Y12 inhibitors’ discontinuation rate, due to adverse effects or economic reasons. Finally, it has to be stressed that technical aspects of PCI have changed significantly since the results of PLATO and TRITON were published, which itself significantly reduced thrombotic complications following the procedure, thereby reducing possible advantages from use of more potent P2Y12 inhibitors.
Therefore, it is necessary to individualise the antiplatelet therapy in patients with ACS in terms of both the choice of P2Y12 receptor inhibitor and the duration of the therapy.
Pre-hospital phase of ACS
Evidence from clinical trials is insufficient to give universal, precise guidelines for the time of DAPT initiation in the pre-hospital phase of ACS. However, the available observations seem to justify the earliest possible initiation of DAPT in patients with STEMI [5, 12]. On the other hand, the latest guidelines regarding the management of NSTE-ACS do not recommend routine pre-treatment with P2Y12 inhibitors (class III A recommendation) [7].
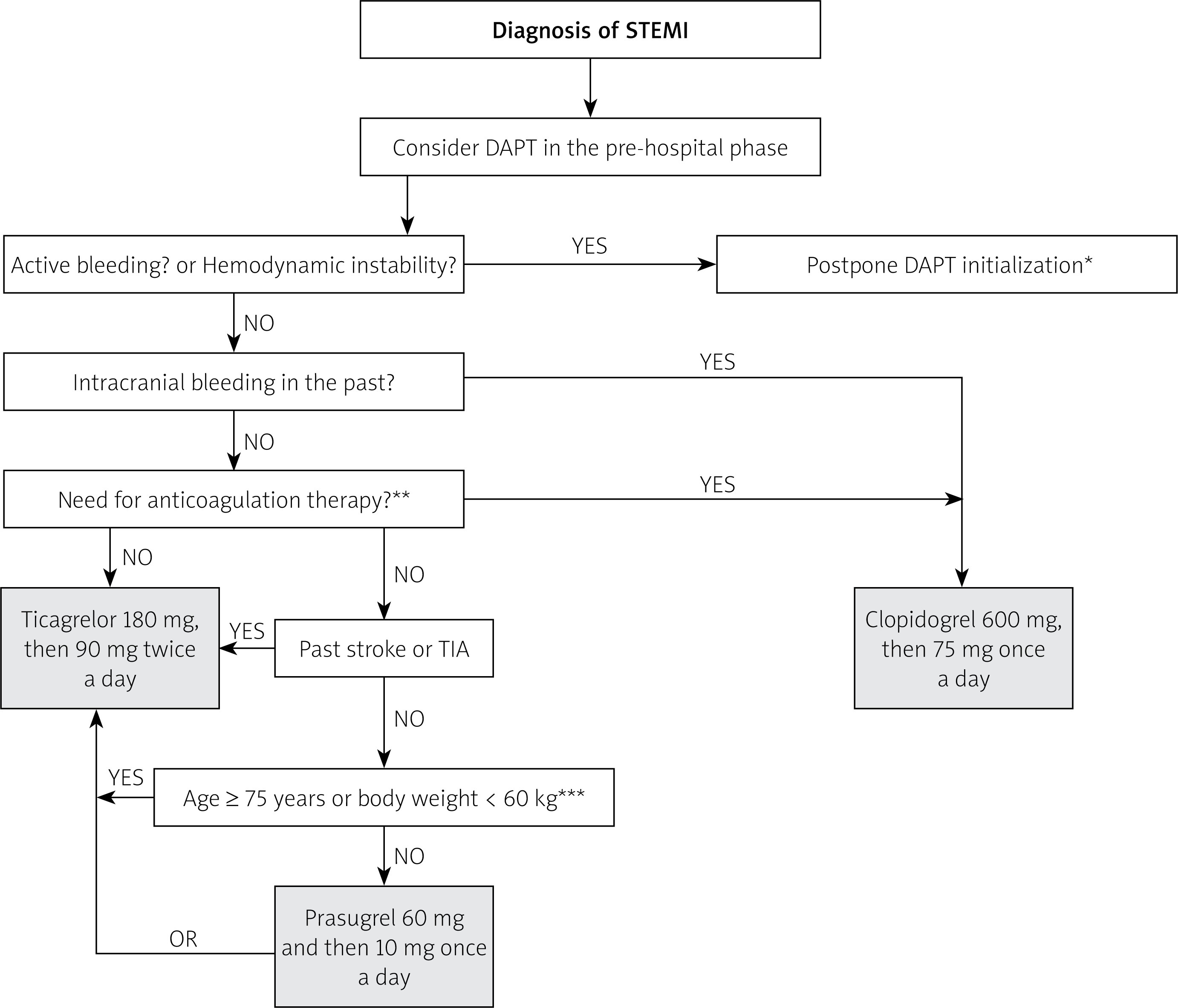
In clinical practice, the diagnosis of STEMI is based on ECG and typical clinical symptoms. Therefore, most patients with STEMI can be identified at the pre-hospital stage and, if eligible for primary PCI (time to PCI ≤ 120 min since diagnosis), they should be immediately loaded with DAPT consisting of ASA and ticagrelor or prasugrel (clopidogrel is limited to cases where other P2Y12 inhibitors are contraindicated – see simplified algorithm in Figure 1 presenting the rules of pre-hospital P2Y12 selection) [6]. Under the Directive of the Ministry of Health of 20th April 2016, such authorisation is also granted to paramedic teams, who after the teletransmission of the ECG tracing and confirmation of the STEMI diagnosis, can administer ticagrelor or clopidogrel and acetylsalicylic acid before arriving at the hospital [12]. Prasugrel was not mentioned in this document. For patients eligible for thrombolysis (time to PCI > 120 min since diagnosis), which is rarely performed in Poland, the P2Y12 receptor inhibitor of choice is clopidogrel in a loading dose of 300 mg (then 75 mg/day) in patients under the age of 75 or a loading dose of 75 mg (then 75 mg/day) in patients aged 75 or over [6].
Figure 1
Simplified P2Y12 inhibitors treatment strategy for use in pre-hospital phase of ST-elevation myocardial infarction (STEMI)
STEMI – ST-elevation myocardial infarction, TIA – transient ischaemic attack. *DAPT should not be started in pre-hospital phase in actively bleeding patients; the approach should be individualized during the in-hospital phase according to the bleeding type. In haemodynamically unstable patients DAPT has to be considered carefully during the in-hospital phase since mechanical complications of STEMI or aortic dissection needs to be excluded first. **Patients with atrial fibrillation or flutter, artificial mechanical heart valves, venous thromboembolism. ***In particular cases of these patients, where the benefits of prasugrel prescription overcome increased bleeding risk, the maintenance dose of 5 mg/day may be used after loading with 60 mg.
The diagnosis of NSTE-ACS based on tests available outside the hospital is much more difficult and rarely possible without the result of troponin serum concentration. Other causes of chest pain such as pneumothorax, hypertensive crisis, aortic dissection or anaemia (leading to myocardial ischaemia) are a contraindication for DAPT. Moreover, data from recent trials and registries indicate that pre-treatment with P2Y12 inhibitors in patients with unknown coronary arteries anatomy increases bleeding risk with no influence on ischaemic risk. Thus, in the case of NSTE-ACS, antiplatelet drugs should not be administered in the pre-hospital phase [7].
From a practical point of view, it is worth noting some circumstances which may reduce the effectiveness of pre-hospital antiplatelet therapy. In vomiting patients, it is necessary to record how much time has passed since the administration of oral drugs and to describe the possible presence of undissolved tablets in vomit [12]. In such cases, DAPT re-loading should be considered individually. Another factor hindering the action of antiplatelet drugs are opiates, which have an inhibitory effect on gastrointestinal passage [6]. Therefore, morphine in patients with ACS should be used only for severe pain and in the lowest effective dose possible [6]. Moreover, crushing ticagrelor tablets or simultaneous intravenous metoclopramide administration may reduce this side effect. Both strategies have been proven to increase the availability of the drug and its antiplatelet effect [13, 14]. Recently available ticagrelor in soluble tablets could also be administered in vomiting or unconscious patients.
Data from the National Registry of Procedures of Invasive Cardiology (ORPKI) summarize the use of DAPT in the pre-hospital phase of ACS. In the period from September 2016 to August 2017 aspirin was administered in 72%, clopidogrel in 51.3%, ticagrelor in 2.3% and prasugrel in 0.4% of STEMI cases [15]. Thus, in this time period just over half of STEMI patients received DAPT in the pre-hospital stage. More recent data from the National Emergency Medical Services Management Support System (2018) reveal that already 72.1% of patients diagnosed with ACS in pre-hospital settings received DAPT. Clopidogrel was still the most frequently administered P2Y12 inhibitor (49.68%) and ticagrelor was used in 25.14% of cases [16].
In-hospital phase of ACS
Patients referred for invasive evaluation of coronary arteries
In cases of STEMI, DAPT should be started as soon as possible after the diagnosis, but no later than at the time of PCI. It has to be emphasised that in patients who have been loaded with clopidogrel in the pre-hospital phase, and do not have contraindications for ticagrelor application, the switch to ticagrelor by loading with 180 mg should be done immediately after admission to the hospital (regardless of the time since admission) (class I B recommendation) [6]. In patients with STEMI, who have not received DAPT in the pre-hospital phase, ticagrelor or prasugrel should be the P2Y12 inhibitor of choice [6] (selection of P2Y12 inhibitor as shown in Figure 1). After the primary PCI, when blood test results are already available, careful bleeding risk assessment has to be performed (as described in the section Periprocedural bleeding risk assessment). In low-bleeding-risk patients ticagrelor or prasugrel should be preferred for further treatment, while in the high-bleedingrisk group ticagrelor and clopidogrel are the P2Y12 inhibitors of choice. In patients with indications for chronic anticoagulation clopidogrel with aspirin should be administered during the in-hospital phase.
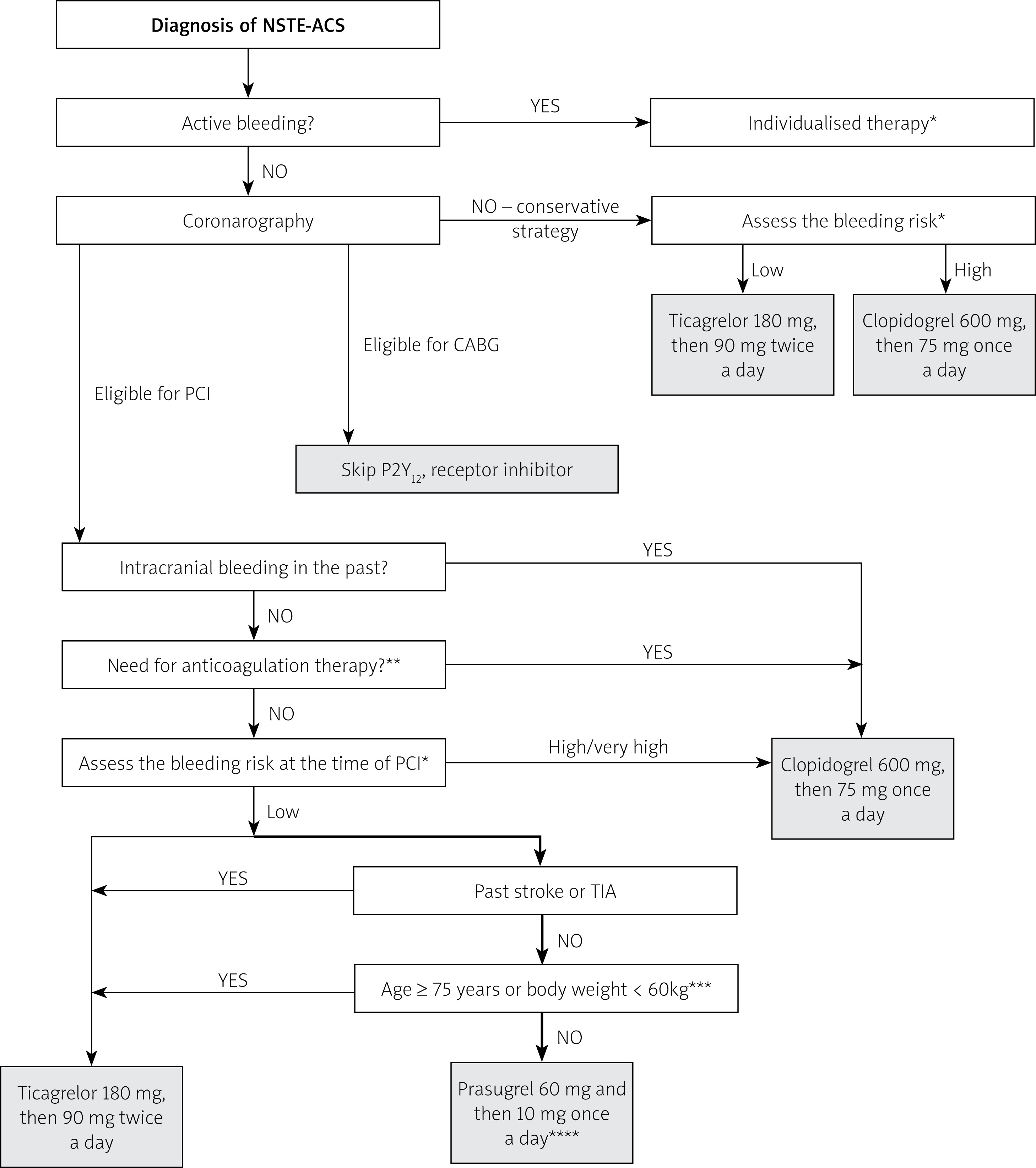
Otherwise, in the case of NSTE-ACS, current guidelines do not recommend administration of P2Y12 in patients planned for an early invasive approach before the coronarography [7]. After the procedure, when the anatomy of coronary arteries is known and the decision to perform PCI has been made, careful bleeding risk assessment has to be performed (as described in the section Periprocedural bleeding risk assessment). In patients with low bleeding risk one of the new generation P2Y12 inhibitors should be administered immediately before the angioplasty. In other cases clopidogrel should be prescribed [7]. An algorithm presenting the choice of P2Y12 inhibitor in NSTE-ACS patients is presented in Figure 2. It is worth noting that prasugrel should be preferred over ticagrelor in P2Y12 inhibitor-naïve patients, when not contraindicated (class IIa B recommendation). Such an approach is justified by the data from recent trials and registries showing that pre-treatment with P2Y12 inhibitors in patients with unknown coronary arteries’ anatomy increases bleeding risk with no influence on ischaemic risk and may postpone coronary artery bypass grafting (CABG) in particular cases. The predominance of the prasugrel-based, no pre-treatment strategy in the therapy of ACS was tested in the multi-centre, randomised, open-label ISAR-REACT 5 study. The study revealed that this strategy significantly reduces the main composite endpoint (all-cause deaths, myocardial infarction and stroke within 1 year after randomisation) with no influence on bleeding risk, compared with the ticagrelor-based, pre-treatment strategy. The results of the study aroused great controversy as, although 1,299 (32.3%) patients among the 4,018 randomized in the study did not receive the treatment according to the study protocol, the intention-to-treat analysis (analysis of the results in all randomized patients, according to the group to which they were originally assigned, regardless of the treatment applied) was used. The large proportion of patients whose treatment had been discontinued or changed, along with the open-label scheme of the trial and the lack of real supervision over the prescribed treatment (patients purchased the drugs individually), necessitate careful interpretation of the results [17, 18]. It is also worth noting that ticagrelor has not been tested in the no-pre-treatment strategy so far. Despite these doubts, based on the study results, the latest NSTE-ACS guidelines propose prasugrel as the P2Y12 inhibitor of choice in NSTE-ACS patients.
Figure 2
Simplified P2Y12 inhibitors treatment strategy for use during in-hospital phase of non-ST-elevation acute coronary syndrome (NSTE-ACS)
TIA – transient ischaemic attack. *High bleeding risk – PRECISE-DAPT ≥ 25 points or presence of one major or two minor ARC-HBR criteria (see Table II); Very high bleeding risk – defined as a recent bleeding episode in the past month or planned, not deferrable surgery in the near future. **Patients with atrial fibrillation or flutter, artificial mechanical heart valves, venous thromboembolism. ***In particular cases of these patients, where the benefits of prasugrel prescription overcome increased bleeding risk, the maintenance dose of 5 mg/day may be used after loading with 60 mg. ****Prasugrel should be preferred over ticagrelor, when not contraindicated (class IIa B recommendation).
Loading with a P2Y12 inhibitor before coronarography in the settings of NSTE-ACS may be considered only in low-bleeding risk patients referred for the delayed invasive strategy (class IIb C recommendation). In such circumstances, only ticagrelor can be administered since prasugrel is prescribed only when the coronary anatomy is known [19, 20].
Table II
Academic Research Consortium for High Bleeding Risk criteria assessed at the time of percutaneous coronary intervention. Bleeding risk is high when one major or two minor criteria are met [20]
| Major criteria | Minor criteria |
|---|---|
| Anticipated use of long-term OAC | Age ≥ 75 years |
| Severe or end-stage CKD (eGFR < 30 ml/min) | Moderate CKD (eGFR 30–59 ml/min) |
| Haemoglobin < 11 g/dl | Haemoglobin 11–12.9 g/dl for men or 11–11.9 g/dl for women |
| Spontaneous bleeding requiring hospitalization and/or transfusion in the past 6 months or at any time, if recurrent | Spontaneous bleeding requiring hospitalization and/or transfusion within the past 12 months not meeting the major criterion |
| Moderate or severe thrombocytopenia (platelet count < 100 × 109/l) | Chronic use of oral non-steroidal anti-inflammatory drugs or steroids |
| Chronic bleeding diathesis | Any ischaemic stroke at any time not meeting the major criterion |
| Liver cirrhosis with portal hypertension | |
| Active malignancy (excluding non-melanoma skin cancer) within the past 12 months* | |
| Previous spontaneous intracranial haemorrhage (at any time) | |
| Previous traumatic intracranial haemorrhage within the past 12 months | |
| Presence of a brain arteriovenous malformation | |
| Moderate or severe ischaemic stroke within the past 6 months | |
| Recent major surgery or major trauma within 30 days prior to PCI | |
| Non-deferrable major surgery on DAPT |
Periprocedural bleeding risk assessment
Current guidelines propose two approaches for the bleeding risk assessment in patients requiring DAPT – the PRECISE-DAPT scale or Academic Research Consortium for High Bleeding Risk (ARC-HBR) criteria. Both methods of assessment should be incorporated at the time of PCI using available blood test results, demographic data and records from patients’ medical history.
The PRECISE-DAPT scale includes such parameters as a history of bleeding requiring medical attention, patient’s age and laboratory test results: haemoglobin concentration, leucocytosis, creatinine clearance; these values should be collected close in time to the index procedure. A score of ≥ 25 points suggests a high risk of bleeding complications, indicating the use of a less potent P2Y12 inhibitor, e.g. clopidogrel, and beneficial reduction of post-hospital DAPT duration. Results below 25 indicate the predominant risk of ischaemic complications and should result in prescription of a more potent P2Y12 inhibitor, e.g. ticagrelor or prasugrel, and a standard or even prolonged DAPT period in the post-hospital phase [5]. The PRECISE-DAPT calculator can be found at www.precisedaptscore.com or downloaded as an application for Android or iOS smartphones. The PRECISE-DAPT scale has not been validated in patients treated with CABG.
Academic Research Consortium for High Bleeding Risk (ARC-HBR) criteria provide an interesting, simpler alternative to the PRECISE-DAPT scale for bleeding risk assessment in patients undergoing PCI [21]. High risk of bleeding is defined as the presence of one major risk factor or two minor risk factors listed in Table II at the time of PCI.
Patients with indications for chronic anticoagulation
Chronic anticoagulant therapy accompanied with DAPT significantly increases the risk of haemorrhagic complications [5, 22]. A less potent P2Y12 inhibitor, e.g. clopidogrel, is a drug of choice in this group of patients with ACS; however, the duration and the composition of antiplatelet therapy (DAPT or monotherapy) should be individually tailored. Generally in all patients triple anticoagulant therapy should be prescribed during the hospital phase (up to 1 week after ACS) and followed by careful evaluation of the bleeding and ischaemic risk factors at the hospital discharge. According to this assessment further therapy is planned, as described in the section Hospital discharge and post-hospital phase.
Data from Polish registries
Recent unpublished data from the PL-ACS database (2019) on DAPT in invasively treated patients with ACS reveal that during the in-hospital phase of STEMI, aspirin was applied in 93.0% and one of the P2Y12 inhibitors in 86.0% of patients (clopidogrel was administered in 42.8% of cases, ticagrelor in 43.2% and prasugrel in 1.6%). In non-ST segment elevation myocardial infarction (NSTEMI), these proportions were as follows: aspirin was applied in 93.0% and a P2Y12 inhibitor in 78.3% of patients (clopidogrel in 55.6% of cases, ticagrelor in 22.7% and prasugrel in 1.2%). The switch from clopidogrel to ticagrelor in the in-hospital phase was performed in 7.2% of patients. As clearly shown here, the use of new P2Y12 inhibitors in Poland is still rare, particularly in NSTEMI patients, despite the highest class of recommendation.
A separate group of ACS patients comprises those who, following the coronary angiography, are candidates for CABG. In the case of STEMI primary PCI is the preferred revascularization method and emergency CABG (usually after loading doses of DAPT) is performed rarely and only when PCI fails [6]. In NSTE-ACS, CABG could be preferred over PCI in selected cases depending on the coronary anatomy and risk assessment. In patients in whom, despite guidelines, DAPT was introduced and the surgery can be postponed, it is advisable to discontinue ticagrelor for a minimum of 3 days, clopidogrel for 5 days and prasugrel for 7 days before CABG, with continuous acetylsalicylic acid administration [5, 22]. DAPT should be restarted after surgery as soon as possible.
Patients referred for conservative treatment
In the case of patients with ACS, who are not eligible for invasive treatment, the P2Y12 inhibitor of choice is ticagrelor. In the case of contraindications, high bleeding risk or indications for chronic oral anticoagulation, clopidogrel should be administered [5].
Hospital discharge and post-hospital phase
The next critical point of the DAPT planning in patients with ACS is the time of the hospital discharge. Two problems have to be considered at this point – the duration of DAPT and the choice of a P2Y12 inhibitor. Generally, DAPT following ACS should last 12 months, but this period may be shortened in a case of high bleeding risk (due to patient characteristics) or parallel anticoagulants use, or prolonged when high ischaemic risk (due to patient or procedure characteristics) dominates. Scrupulous reevaluation of ischaemic and bleeding risk of each patient is required followed by further therapy individualisation.
High-bleeding-risk patients
The PRECISE-DAPT scale or Academic Research Consortium for High Bleeding Risk (ARC-HBR) criteria as well as clinical observations made during the hospitalization – e.g. drop in haemoglobin levels, bleeding events, new-onset atrial fibrillation – should be revised here carefully. In patients with high bleeding risk shortening of DAPT to 6 months in STEMI patients or to 3–6 months in NSTE-ACS should be considered and a less potent P2Y12 should be preferred, as presented in Figure 3 for STEMI and Figure 4 for NSTE-ACS. It is worth noting that in some trials such as in SMART-CHOICE [23], which importantly influenced the latest version of the NSTE-ACS guidelines, patients with STEMI were also included since it seems to be reasonable to consider the shortening of DAPT to 3 month also in particular cases of high-bleeding-risk STEMI patients.
Figure 3
Algorithm for dual antiplatelet treatment in patients with ST-elevated myocardial infarction (STEMI) depending on the bleeding risk. (Modified on the basis of 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS [5])
PCI – percutaneous coronary intervention, green – class I recommendation, yellow – IIa, orange – IIb. *If patient is not eligible for treatment with prasugrel or ticagrelor. **High bleeding risk – PRECISE-DAPT ≥ 25 points or presence of one major or two minor ARC-HBR criteria (Table II). #If patient is not eligible for treatment with ticagrelor. A – acetylsalicylic acid, C – clopidogrel, T – ticagrelor, P – prasugrel.
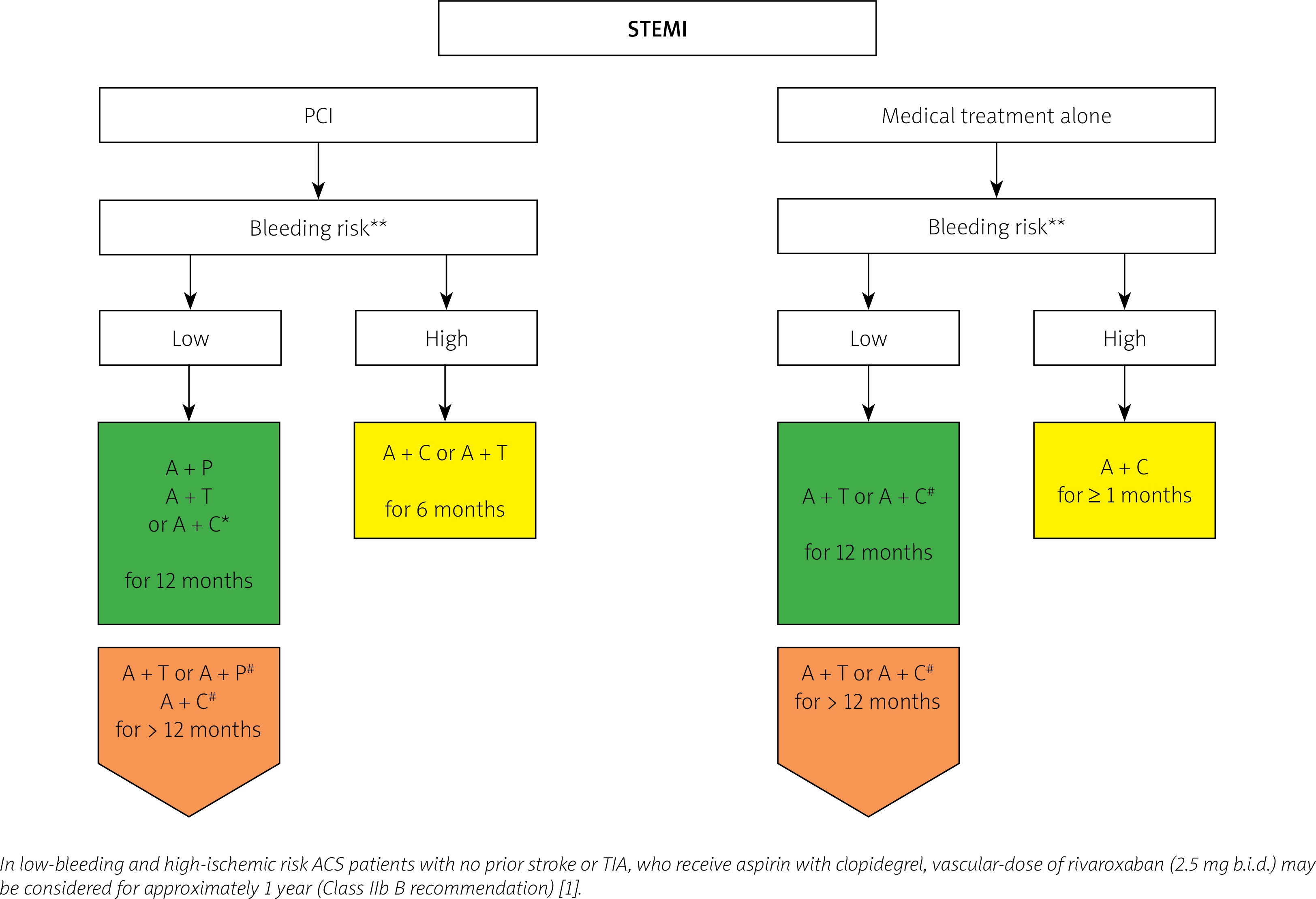
Figure 4
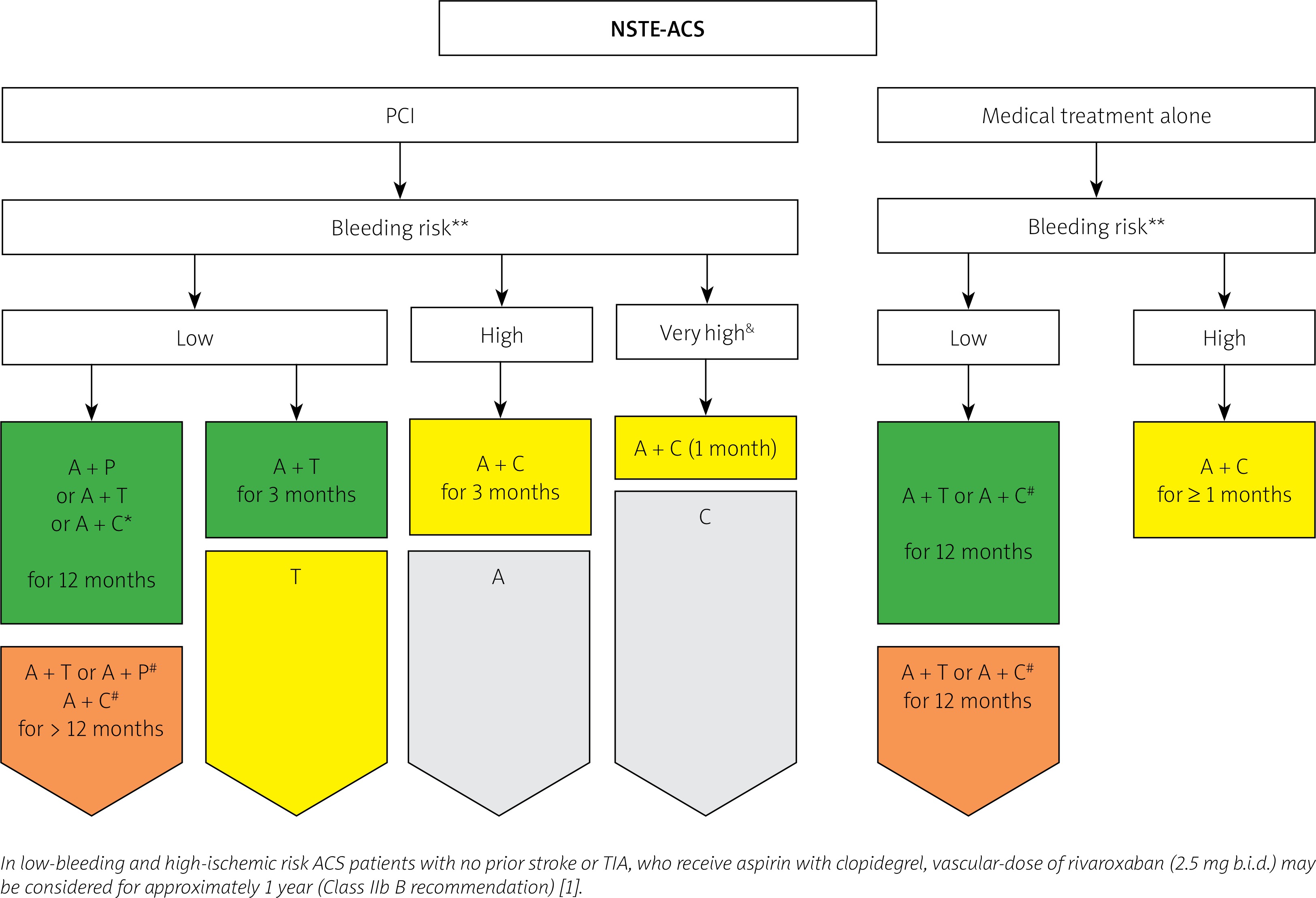
Novel approach for antiplatelet treatment in patients with NSTE-ACS (modified on the basis of 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation) [7])
&Defined as a recent bleeding episode in the past month or planned, not deferrable surgery in the near future. *When prasugrel or ticagrelor is contraindicated. #If patient is not eligible for ticagrelor. **High bleeding risk – PRECISE-DAPT ≥ 25 points or presence of one major or two minor ARC-HBR criteria (Table II), green – class I recommendation, yellow – IIa, orange – IIb). A – acetylsalicylic acid, C – clopidogrel, T – ticagrelor, P – prasugrel.
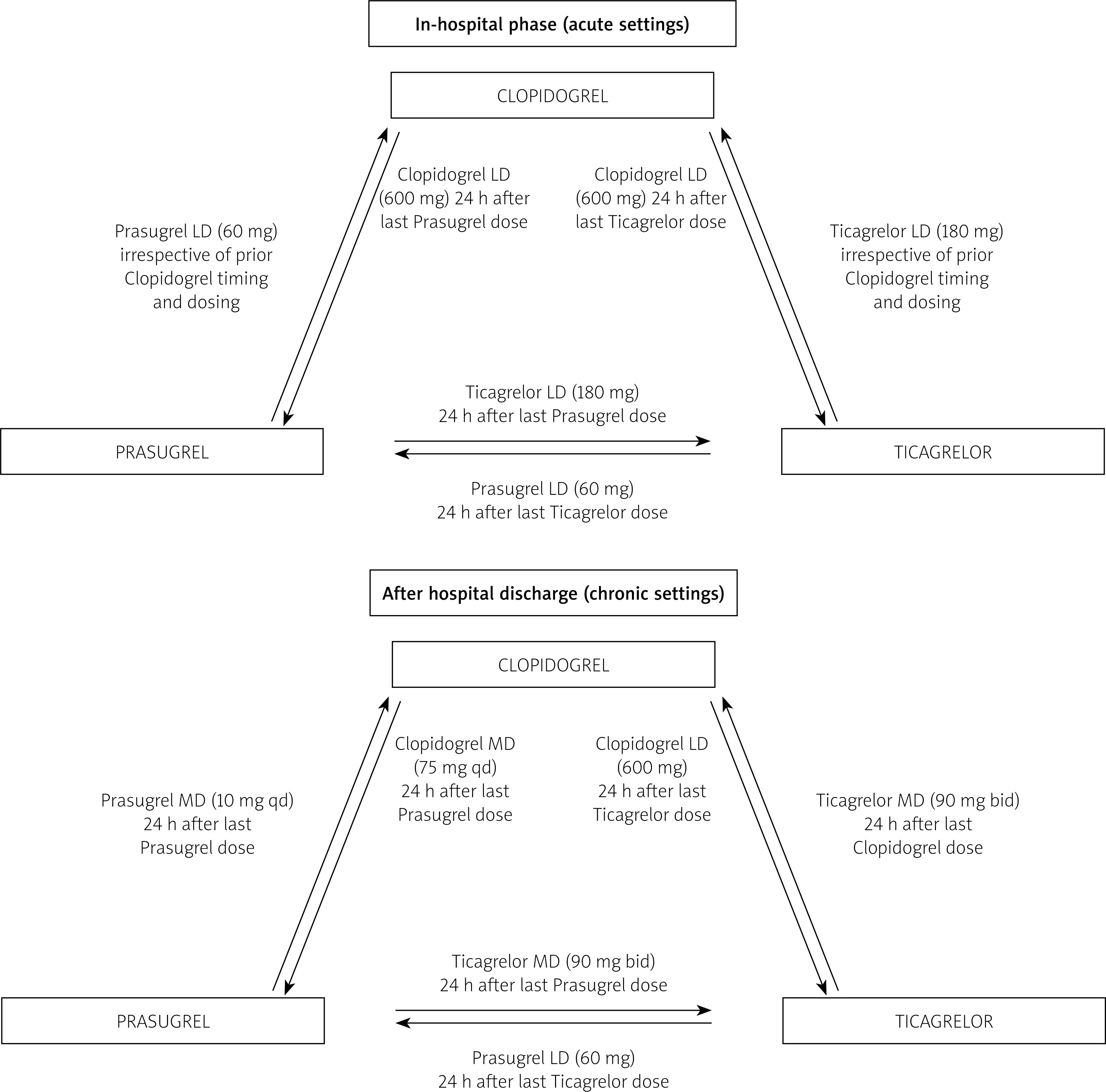
The new NSTE-ACS guidelines also permit the DAPT de-escalation strategy (switching to clopidogrel after initial administration of ticagrelor or prasugrel) to treat patients who are no longer suitable for more potent P2Y12 inhibitors, e.g. due to increased risk of bleeding (class IIb A recommendation) [7]. De-escalation may be guided by platelet function testing or CYP2C19 genotyping or even unguided, based on clinical assessment. It has to be stressed that the unguided approach and uniform de-escalation switching schemes have not been tested in clinical trials so far, since de-escalation should be performed carefully in selected patients and potential increased risk of ischaemic events needs to be considered. It seems to be reasonable to perform de-escalation after at least 1 month after ACS. Algorithms describing possible ways of P2Y12 inhibitor switching during DAPT, based on pharmacokinetic data, are shown in Figure 5.
Figure 5
Algorithm for switching between oral P2Y12 inhibitors in the in-hospital and out-of-hospital settings (modified on the basis of 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS [5])
Low-bleeding-risk patients
In low-bleeding-risk patients more potent P2Y12 inhibitors – ticagrelor or prasugrel in STEMI and prasugrel in NSTE-ACS – should be preferred, as presented in Figure 3 for STEMI and Figure 4 for NSTE-ACS. Moreover, patients who were initially at low risk of bleeding, and if DAPT was well tolerated in the obligatory 12-month period, may be considered for prolongation of the therapy.
According to the Focused update on DAPT Guidelines 2017, the use of the DAPT scale is suggested for DAPT prolongation in STEMI patients (a calculator is available at www.daptstudy.org or as an application for an Android or iOS smartphone). A score of 2 (or more points) indicates a high risk of thrombotic complications and supports potential benefits from DAPT prolongation (class IIb B recommendation), while a score of fewer than 2 points suggests lack of benefits from DAPT continuation.
A slightly different approach is proposed by the new NSTE-ACS guidelines 2020. Prolonged DAPT should be considered in patients without increased risk of major or life-threatening bleeding and high ischaemic risk (class IIa A recommendation) or may be considered in patients with a moderate risk of an ischaemic event (class IIb A recommendation). Ischaemic risk assessment is much more complicated than in previous guidelines discussed. A two-step approach is proposed: (1) in the first step the clinician stratifies the severity of individual patient coronary artery disease into complex or non-complex disease (the judgement is based on the patient’s cardiovascular history and/or coronary anatomy); (2) in the second step patient- and procedure-dependent ischaemic-risk-enhancing factors are analysed – see Table III for more details.
Table III
Patient- and procedure-dependent ischaemic-risk-enhancing criteria for extended treatment with DAPT (modified on the basis of 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation) [7]. The complexity of CAD is assessed by the clinician, who takes into consideration individual patient’s ischaemic events history and coronary anatomy
The preferred P2Y12 inhibitor for prolonged DAPT is ticagrelor, usually in a dose of 60 mg twice a day (In the PEGASUS trial, such treatment was beneficial for up to 36 months after myocardial infarction, in patients aged ≥ 65 years or ≥ 50 years with one of the additional high-risk factors for ischaemic incidents, i.e. with diabetes mellitus requiring pharmacotherapy, with previous myocardial infarction, multivascular coronary disease or chronic kidney disease with GFR < 60 ml/min) [24]. In all patients after ACS, ASA lifelong therapy should be introduced following DAPT discontinuation [5].
In low-bleeding- and low-ischaemic-risk NSTE-ACS patients the new treatment strategy consisting of 3 months of DAPT with aspirin and ticagrelor followed by ticagrelor monotherapy up to 12 months after the ACS should be considered [7]. Such an approach was tested in the TWILIGHT trial, where 64.8% of all 7119 randomized participants had NSTE-ACS and were generally low-ischaemic- and -bleeding-risk patients according to current criteria. The shortening of DAPT resulted in 44% reduction of haemorrhagic complications in the period from 3 to 12 months after PCI (HR = 0.56; 95% CI: 0.45–0.68; p < 0.001), defined as type 2, 3 or 5 bleeding according to BARC. At the same time, this DAPT modification did not increase the prevalence of ischaemic events (secondary composite endpoint – death from any cause, stroke, myocardial infarction – HR 0.99; 95% CI: 0.75–1.25; p < 0.001 for equivalence) [25].
Patients with indications for chronic anticoagulation
In the group of patients with indications for chronic anticoagulation the in-hospital triple therapy period should be followed by careful evaluation of bleeding and ischaemic risk factors at the hospital discharge. We do not have a dedicated scale evaluating the risk of bleeding and ischaemic events in this population; however, according to the latest NSTE-ACS guidelines, despite the lack of validation, the use of PRECISE-DAPT or ARC-HBR criteria is advised for the assessment of bleeding risk in NSTE-ACS patients [7]. Otherwise, the risk of ischaemic events is demonstrated by a subject’s clinical characteristics and the complexity of coronary intervention, and may be assessed using the criteria listed in Table III [7]. Since there are no large randomized clinical trials on the topic, it seems to be reasonable to use the same criteria and algorithm for STEMI patients.
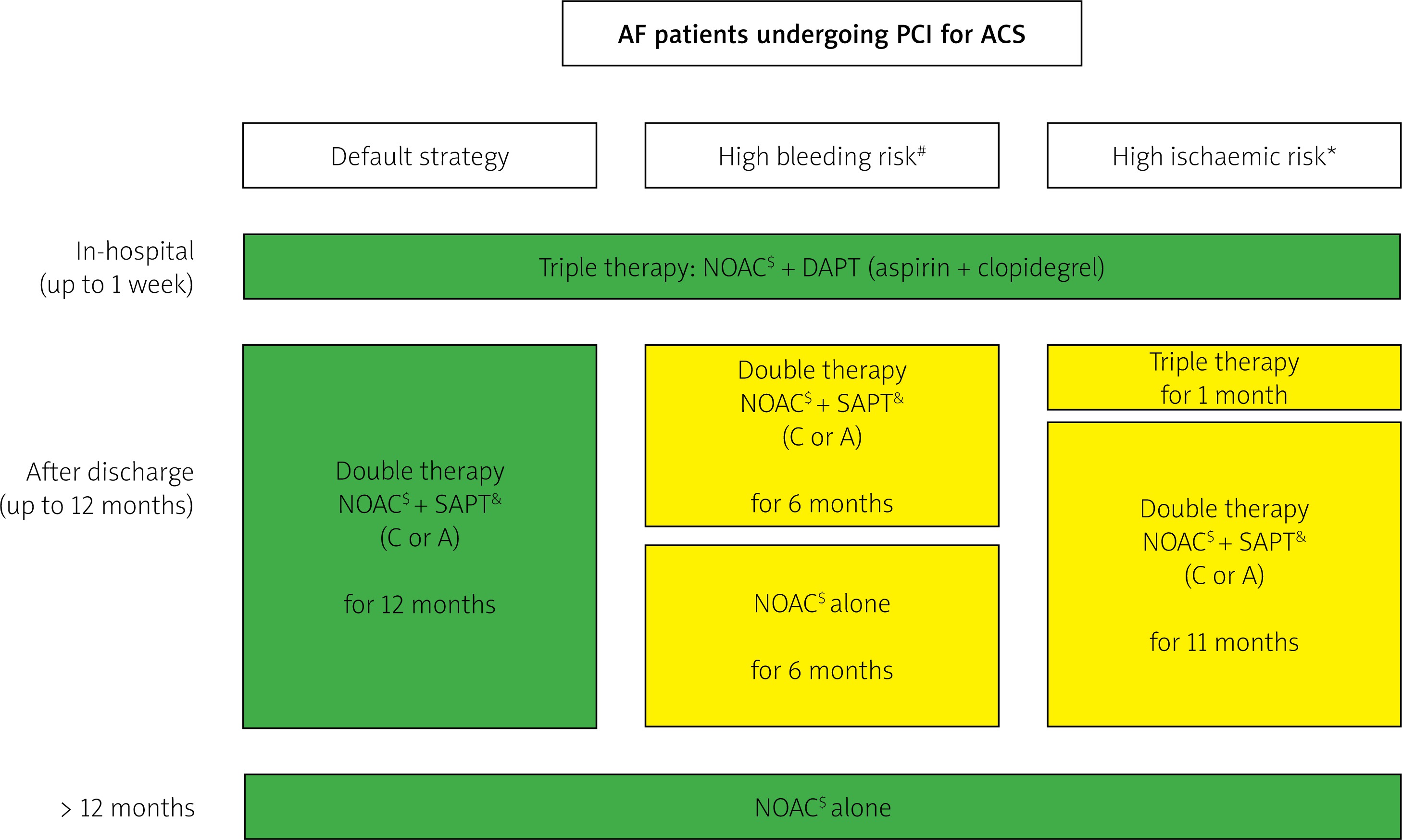
In patients with predominating bleeding risk factors the triple therapy used at hospital should be reduced at discharge to double therapy (anticoagulant + clopidogrel or aspirin) for 6 months followed by an anticoagulant alone. Otherwise in patients with ischaemic risk overbalancing bleeding risk triple therapy should be prolonged for 1 month after the hospital discharge and followed by double therapy (anticoagulant + clopidogrel or aspirin) up to 12 months after the ACS. In all other cases with no predomination of either ischaemic or bleeding risk triple therapy should be reduced at discharge to double therapy (anticoagulant + clopidogrel or aspirin) for 12 months. One year after ACS in all cases antiplatelets should be withdrawn and the therapy should be limited to an oral anticoagulant [7]. The principles of antiplatelet treatment in anticoagulated patients with ACS and the algorithm facilitating the selection of antiplatelet therapy duration are presented in Table IV and Figure 6.
Table IV
Strategies to avoid bleeding complications in ACS patients treated with oral anticoagulant (modified on the basis of 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS [1] and 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation [2])
Figure 6
Algorithm for dual antiplatelet therapy in PCI-treated acute coronary syndrome patients with an indication for chronic oral anticoagulation (modified on the basis of 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation [7])
A – acetylsalicylic acid, C – clopidogrel, T – ticagrelor, P – prasugrel, NOAC – non-vitamin K oral anticoagulant, DAPT – dual antiplatelet treatment, SAPT – single antiplatelet treatment, PCI – percutaneous coronary intervention, ACS – acute coronary syndrome. #assessed using PRECISE-DAPT scale or ARCHBR criteria, *assessed with criteria listed in Table III, $NOACs are preferred when not contraindicated, &in SAPT clopidogrel is preferred [29], green – class I recommendation, yellow – IIa, orange – IIb.
Planning long-term P2Y12 inhibitor therapy
When planning long-term therapy one has to remember about the most common reasons for the discontinuation of particular P2Y12 inhibitors. It was shown in a recent meta-analysis of randomised clinical trials that as many as 25% of patients prescribed with ticagrelor stopped taking the medication prematurely. This was significantly more frequently compared to clopidogrel cessation [26]. The analysis of Polish prescription data (RECEPTOmetrPEX panel) showed that 37% of patients discontinued ticagrelor therapy after 1 month, and the therapy duration was less than 60 days in nearly half of the patients. Furthermore, after premature discontinuation of ticagrelor therapy, 57% of patients did not take any P2Y12 inhibitors. The most common cause of premature discontinuation of ticagrelor worldwide was its side effects, such as bleeding, dyspnoea and sporadically bradyarrhythmia. The high cost of the medication and its twice-daily dosage regimen are also significant [26]. Patients’ education regarding possible side effects, including dyspnoea, is very important. Dyspnoea associated with ticagrelor application decreases with time or even disappears completely and, most importantly, it does not influence the effectiveness of the treatment [27]. Possible predictors of this side effect are currently studied, which may help to identify patients who will suffer due to the phenomenon. Generally switching between different types of P2Y12 inhibitors should be avoided, since the only replacement whose safety has been confirmed in clinical trials is the switch from clopidogrel to ticagrelor in an acute phase of cardiac infarction. However, in specific clinical scenarios (bleeding, persistent severe dyspnoea, initiation of oral anticoagulation, poor economic situation, etc.) other drug changes are required. Algorithms describing possible ways of P2Y12 inhibitor switching during DAPT, based on pharmacokinetic data, are shown in Figure 5 [5].
Data from Polish registries
Data from the PL-ACS (2019) database show the structure of antiplatelet treatment at discharge in Polish patients with ACS. After PCI-treated STEMI 9.1% of patients were discharged on triple antithrombotic therapy, 84.5% on DAPT, 5.9% with a single antiplatelet drug, and 0.5% without any antiplatelet treatment. Following PCI-treated NSTEMI triple therapy was administered to 13.6% of patients, DAPT to 78.0%, monotherapy to 7.9%, and 0.6% of patients were discharged without any antiplatelet treatment. Worth noting in 2019 is the change of the leading combination of DAPT prescribed following STEMI compared to previous years. For the first time in Poland, the combination of aspirin and ticagrelor was the most frequently prescribed one (in 53.4% of patients) and outstripped aspirin with clopidogrel (prescribed in 44%). Aspirin with prasugrel was prescribed only in 2.6%. However, among NSTEMI patients the combination of aspirin with clopidogrel was still the most prescribed one (61.4%). Aspirin with ticagrelor or aspirin with prasugrel was recommended in 36.3% and 2.3% of patients respectively. The duration of DAPT, in patients without anticoagulation, advised at the discharge was usually 12 months (in 93.0% of patients with STEMI and in 91.8% with NSTEMI); less frequently a longer period (3.9% of patients with STEMI and 3.9% with NSTEMI) or shorter period (3.1% of patients with STEMI and 4.1% with NSTEMI) was suggested. Unfortunately, and inconsistently with current guidelines, the same 12-month DAPT period was most frequently recommended in patients on anticoagulants (in 61.6% of patients with STEMI and in 55.9% with NSTEMI). Less frequently, 6-month (in 18.2% of patients with STEMI and in 20.2% with NSTEMI) and 1–2-month periods (in 9.9% of patients with STEMI and in 14.6% with NSTEMI) were suggested [28].
Summary
Appropriately tailored DAPT is a key to the successful treatment of ACS. According to the recent guidelines careful assessment of ischaemic and bleeding risk has to be performed in each patient individually and repeated at successive phases of the treatment. According to the risk assessed and clinician’s intuition, the therapy should be individualized using the following variables: (1) choice of the P2Y12 receptor inhibitor, (2) the composition of antiplatelet therapy (dual or single blockade) and (3) the period of treatment (from 1 week of DAPT to > 12 months).







