
INTRODUCTION
Rhinophyma represents an advanced stage of rosacea and is a chronic condition with a long-term course. Rosacea occurs significantly more often in women; however, its end-stage manifestation – rhinophyma – is most commonly observed in men in their 50s and 60s. The condition is characterized by sebaceous gland hyperplasia, fibrosis of soft tissues, and proliferation of blood vessels [1, 2]. Its etiopathogenesis remains unknown. The treatment of choice for advanced rhinophyma is surgical intervention. Among the various invasive techniques, conventional surgical methods should be highlighted, which involve excising the rhinophyma with a scalpel or removing it with simultaneous coverage of the wound using a full-thickness skin graft. In the treatment of the condition, CO2, diode, and YAG lasers, as well as cryotherapy and electrosurgery, are also increasingly used [3–8].
The main concern for patients with symptoms of rhinophyma – apart from functional impairments – is the esthetic aspect, particularly the disfigurement and deformation of the nose. As a result, patients often become socially withdrawn, avoiding both interpersonal interactions and broader social contact. Most individuals with rhinophyma are unaware of the therapeutic options available, which aim to improve both nasal function and facial esthetics.
CASE REPORT
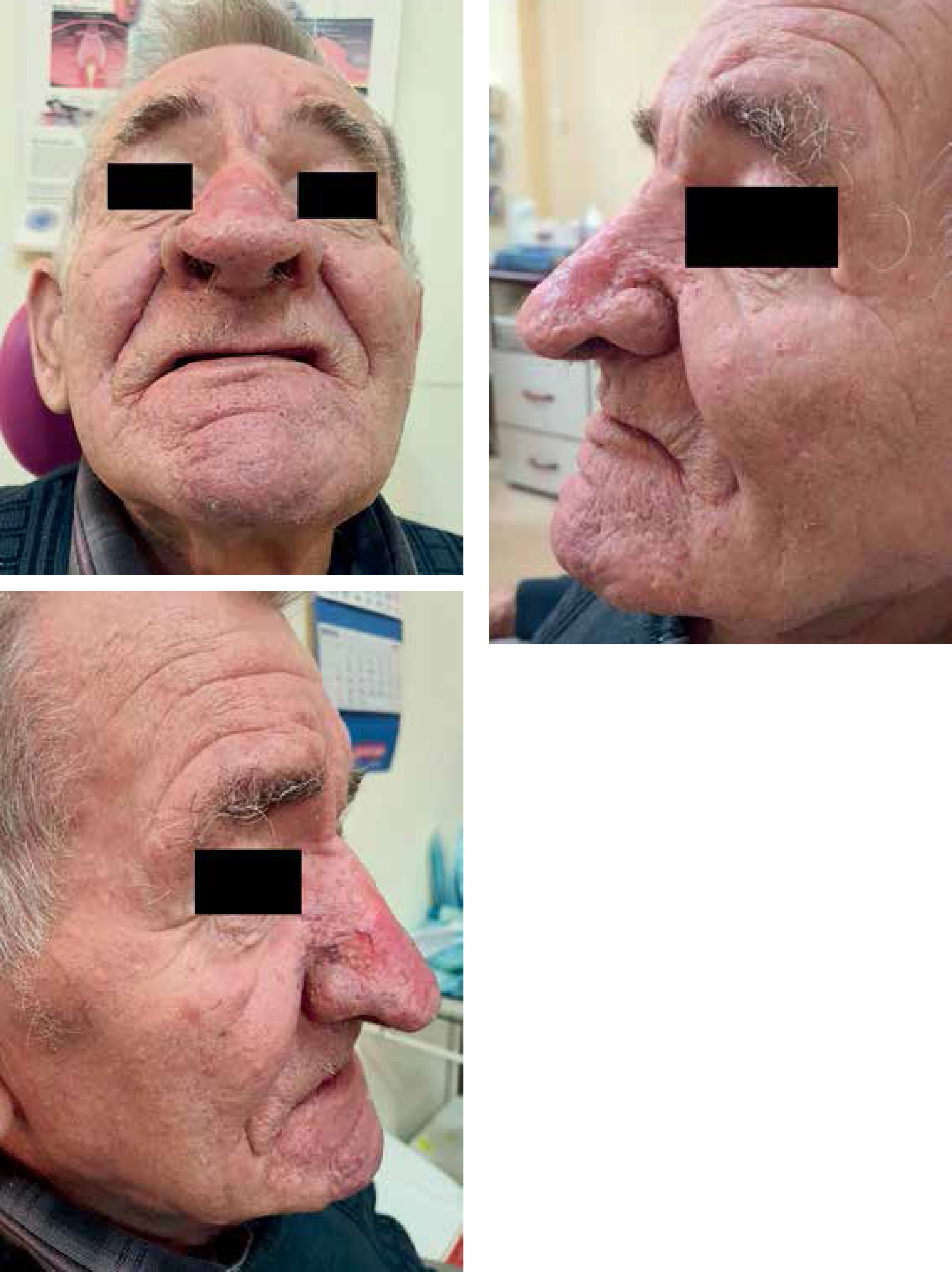
A 77-year-old male patient was referred to the Department of Otolaryngology due to giant rhinophyma (Figure 1). The condition led to complete social isolation. He had not left his home for several years, and even interactions with close family members were markedly restricted. The patient experienced significant difficulties with eating and fluid intake, as the enlarged nose obstructed both the upper and lower vermilion border. He was able to take in fluids only by using a straw. Treatment options and the anticipated cosmetic outcome were explained to the patient, who gave consent for surgical treatment. After disinfecting the surgical field and administering local anesthesia with 15 ml of 1% lidocaine injected into the nose, the giant rhinophyma was excised in layers, using a 1470 nm diode laser at 10 W in continuous mode, while maintaining full symmetry. The excised skin layers measured approximately 2 cm in length, 0.7 cm in width, and 0.3 cm in thickness. Layered excision began at the nasal dorsum and continued toward the lateral surfaces and alae, with each subsequent series starting again from the dorsum and ending at the alae. During the procedure, the diode laser provided perfect hemostasis, and no additional bipolar electrocoagulation was required. After achieving the desired cosmetic outcome, a dressing with Oxycort ointment was applied. On the second day, the dressing was changed. Healing proceeded normally through granulation, and the patient was discharged home. After three weeks, the nasal wound was completely healed, with an excellent cosmetic result (Figure 2).

DISCUSSION
Surgical treatment of rhinophyma continues to evolve alongside technological advancements in medicine. Historically, management involved rhinophyma excision using a surgical blade (so-called “cold steel”), with bipolar electrocoagulation required to control bleeding. With the emergence of laser technologies, the CO2 laser (wavelength 10,600 nm) has been increasingly used in the treatment of the condition. The 1470 nm diode laser appears to be a very effective tool in the treatment of rhinophyma, thanks to its hemostatic capabilities. In rhinophyma, the blood vessels are significantly dilated, making complete hemostasis extremely important. CO2 and diode lasers exhibit similar properties: both use water as the primary chromophore and are typically operated in continuous mode at comparable power settings for the treatment of rhinophyma. However, both lasers also differ, for example, in tissue penetration depth. In the CO2 laser, penetration reaches approximately 0.3 mm, whereas in the diode laser it is deeper, ranging from 0.5 to 0.7 mm. The lasers also differ in the temperature of the tissue at the site of application. For the CO2 laser, tissue temperature ranges between 300°C and 450°C. In contrast, the thermal effect of the diode laser is significantly higher and results not only from direct and indirect heating of the tissue by light, but primarily from the contact-based operation of the optical fiber. The fiber itself acts as an efficient heat source, and its operating temperature during use exceeds that generated solely by light absorption in the tissue, reaching approximately 700°C. This means that an electrocoagulation effect is achieved simultaneously. Despite the high temperatures achieved, its operation remains well-controlled and safe, as heat diffusion is localized [9]. This specific mode of action allows for excellent hemostasis while minimizing thermal injury to surrounding tissues. Layered excision of nasal rhinophyma using a diode laser is an extremely precise procedure. However, it is important to avoid exposing the nasal cartilage and to maintain nasal symmetry. In cases where cartilage or bones become exposed (i.e., with deep excision of the rhinophyma), exposed cartilage or bones should not be left to re-epithelialize on its own. Instead, it should be covered with a full-thickness skin graft or, if the excision involves only the ala, with a pedicled flap from the cheek. Leaving exposed cartilage to re-epithelialize may lead to necrosis, resulting in nasal deformity and poor cosmetic and functional outcomes. There is extensive literature describing surgical treatment using the CO2 laser, while reports on the application of the diode laser remain scarce. Notably, in all cases involving the CO2 laser, additional electrocoagulation was required. In contrast, both Apikian et al. [10] and Bhandry and Bhat [11] report that precise excision of rhinophyma with a diode laser is feasible thanks to a completely bloodless operative field. Unfortunately, the author was unable to find any studies in the available literature directly comparing treatment outcomes between the two laser modalities.
CONCLUSIONS
Rhinophyma is a benign condition affecting the external nose. The predominant complaint in patients with rhinophyma is the pronounced cosmetic disfigurement, which leads to social isolation. Surgical treatment of rhinophyma using a diode laser is well tolerated by patients, can be performed under local anesthesia, and provides excellent cosmetic and functional outcomes.










