
Introduction
Skin cancers are the most commonly diagnosed malignant neoplasms worldwide. The lifetime risk of developing non-melanoma skin cancers exceeds 20% and increases with age, with the highest incidence observed in individuals over 80 years of age. Basal cell carcinoma is the most frequently diagnosed type (80%), while squamous cell carcinoma accounts for approximately 15–20% of cases [1]. Although these cancers rarely metastasize or lead to patient death, they represent a significant clinical problem. If left untreated, skin cancers infiltrate and destroy surrounding tissues, resulting in functional impairment, substantial aesthetic defects, and considerable deterioration in quality of life.
Surgery is the most established and commonly employed treatment modality for skin cancers, offering high cure rates with an approximate 5% risk of recurrence. The likelihood of recurrence after primary treatment depends, among other factors, on the location of the primary lesion. Three anatomical risk zones have been defined: the L area (low risk of recurrence, e.g., trunk and extremities), the M area (intermediate risk, e.g., central face, cheeks, forehead, scalp), and the H area (high risk, including so-called “mask area” of the face – specifically, the periorbital region, eyelids, periauricular region, temples, ears, central face, lips, and nose – as well as other high-risk locations such as the genitalia, hands, and feet [1–3]. Treatment outcomes comparable to those achieved with surgery can also be obtained with radiotherapy, which is typically considered in cases where surgery would result in disfigurement, functional impairment, or when clear surgical margins cannot be obtained [1, 4–7]. Other treatment options include cryotherapy and topical pharmacotherapy (e.g., 5-fluorouracil, imiquimod). The role of brachytherapy, a specific form of radiotherapy, in the treatment of skin cancers remains insufficiently described. Brachytherapy involves placing a radiation source in close proximity to or within the tumour, allowing for targeted dose delivery and sparing of surrounding healthy tissues, thereby reducing the risk of adverse effects.
To date, no prospective studies have directly compared the effectiveness of the aforementioned treatment modalities [6–9]. In this context, reporting real-world clinical practice data becomes increasingly important.
Aim
The aim of this study was to assess the efficacy and safety of skin cancer brachytherapy based on data from the Brachytherapy Unit at the Tadeusz Koszarowski Cancer Center in Opole.
Material and methods
Between 2015 and 2023, a total of 265 patients with epithelial malignant skin tumours were treated, including 287 cancerous lesions. The study had an ambispective design, combining retrospective data collection with prospective follow-up of patients. The analysis focused on treatment outcomes of individual lesions; however, only 236 lesions in 215 patients were included in the final assessment. These patients had a minimum follow-up of 1 year after treatment. In 18 patients (6.8% of the analysed cohort), more than one skin cancer lesion was treated – 15 patients had two lesions, and 3 patients had three. A total of 50 patients, with 51 (17.8%) lesions, were lost to follow-up and were therefore excluded from the outcome analysis.
The study population was predominantly elderly, with a median age of 77 years (range: 45–95 years). Only 39 (18.1%) patients were younger than 65, while 48 (22.3%) patients were older than 85. There was a slight predominance of male patients (116, 54%) over female patients (99, 46%). Lesion characteristics are summarized in Table 1. Basal cell carcinoma was the predominant histologic type (78.4%), although a more prognostically unfavourable squamous cell carcinoma was diagnosed in approximately 1 in 5 patients. The majority of lesions (56.8%) were located in high-risk areas for recurrence, while only 7 (3.0%) lesions were found in low-risk zones. Clinical staging was performed according to the TNM classification, 8th edition (2017) [10], with tumour size designated by the T category. Only patients without regional lymph node metastases (N0) and distant metastases (M0) were eligible for brachytherapy.
Table 1
Tumour lesion characteristics
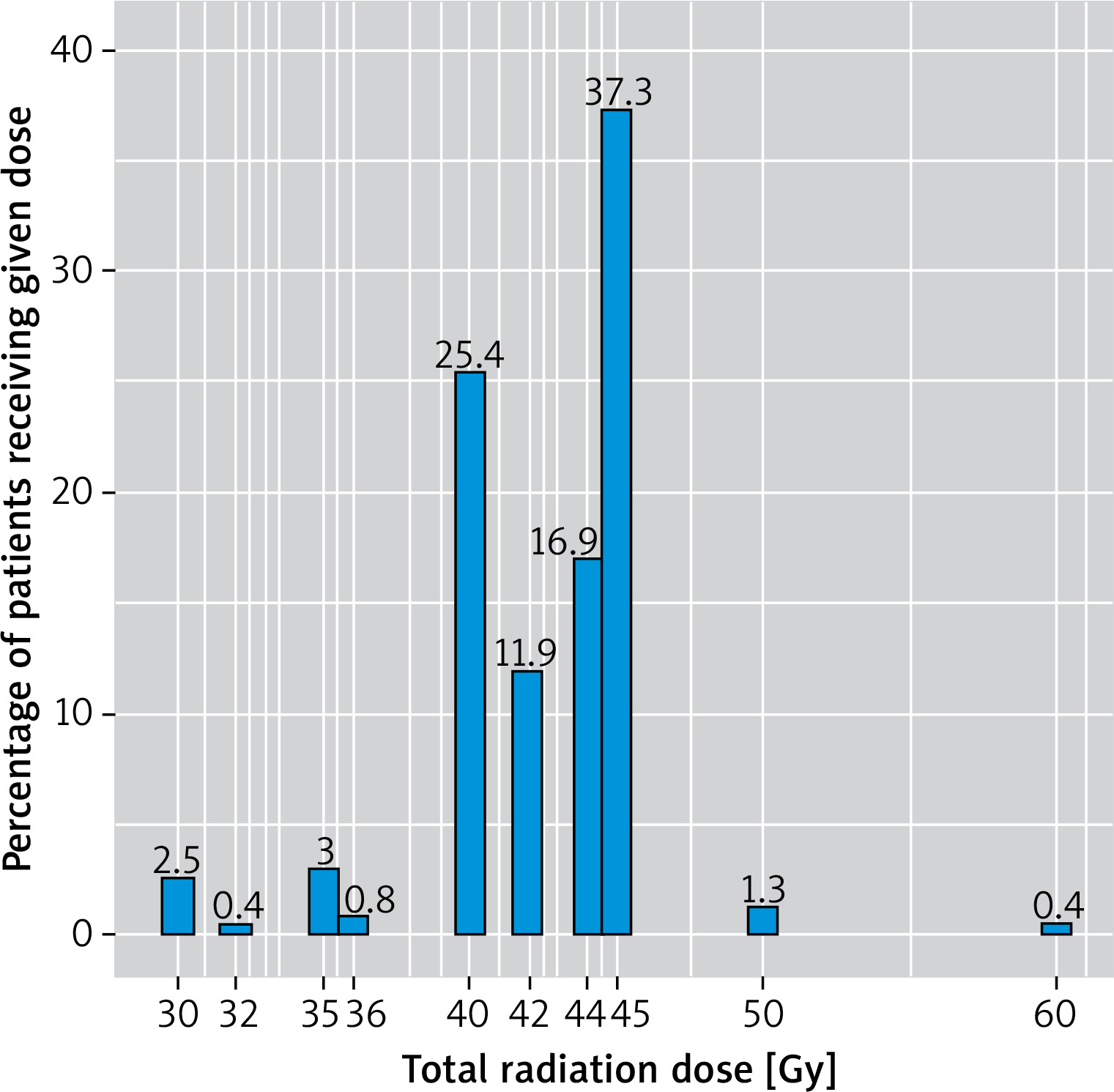
In all patients, high-dose-rate (HDR) brachytherapy was used. Until 2019, treatment was performed using the microSelectron HDR system (Elekta AB, Stockholm, Sweden), and from 2020 onwards, the Flexitron system (Elekta AB, Stockholm, Sweden), both employing the iridium-192 isotope. In most cases (229 lesions), surface brachytherapy was applied using bronchial applicators in combination with a Freiburg flap applicator or custom-made moulds. In 7 cases, an interstitial technique was used. Treatment planning was based on computed tomography and performed using the Oncentra Brachy planning system. Brachytherapy was administered as the primary treatment modality (105 lesions, 44.5%) or – more commonly – as treatment for recurrence following prior surgical intervention (131 lesions, 55.5%). The total treatment duration ranged from 4 to 42 days, with a median of 21 days. The total radiation dose administered ranged from 30 to 60 Gy, with a median dose of 44 Gy (Figure 1). The number of treatment fractions varied between 3 and 12, with a median of 9 fractions. The most commonly used regimen was 45 Gy delivered in 9 fractions.
Figure 1
Total radiation dose administered in the study group with the percentage of patients receiving each dose
Treatment failure was defined as either recurrence or a non-curable case. Lesion progression within 6 months after the completion of brachytherapy was classified as a non-curable case, whereas progression occurring after this period was considered a recurrence. For statistical analysis, the Fisher’s exact test was used to assess the association between treatment failure and tumour size (T category), lesion location, and total radiation dose. The c2 test was applied to evaluate the relationship between treatment failure and sex, histological type, and whether the lesion was primary or recurrent. The Student’s t-test was used to analyse the correlation between treatment failure and patient age. A p-value of less than 0.05 was considered statistically significant.
Results
The median follow-up period was 24 months (12–67 months). Larger tumours were more commonly observed in male patients, although the differences in tumour stage by sex were not statistically significant. Brachytherapy resulted in complete tumour control in the vast majority (representative clinical outcomes are shown in Figures 2 and 3).
Figure 2
Basal cell carcinoma – recurrence after surgical treatment: before (A) and 3 years after (B) surface HDR brachytherapy. The patient received a total dose of 44 Gy in 11 fractions, administered three times per week
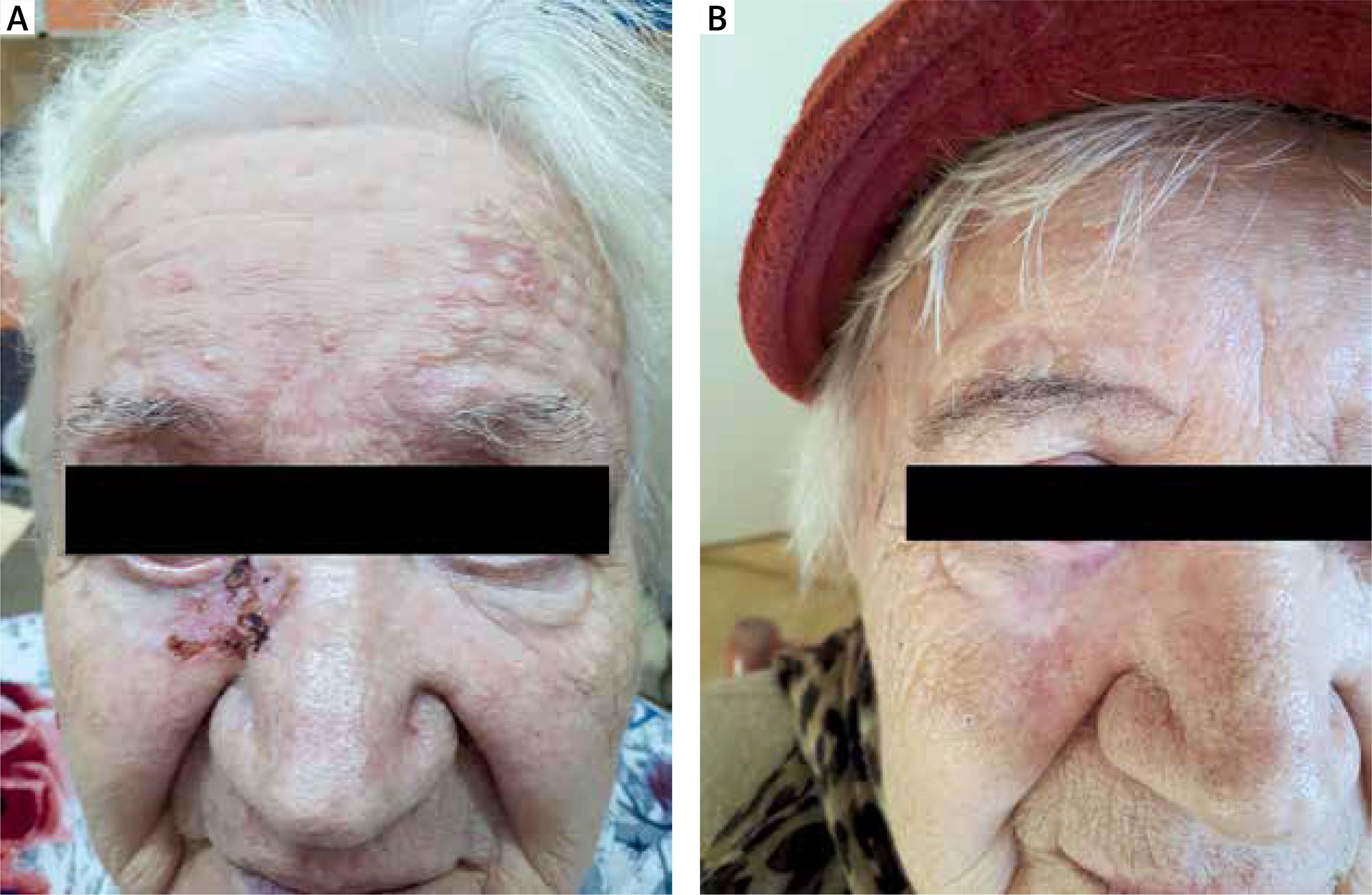
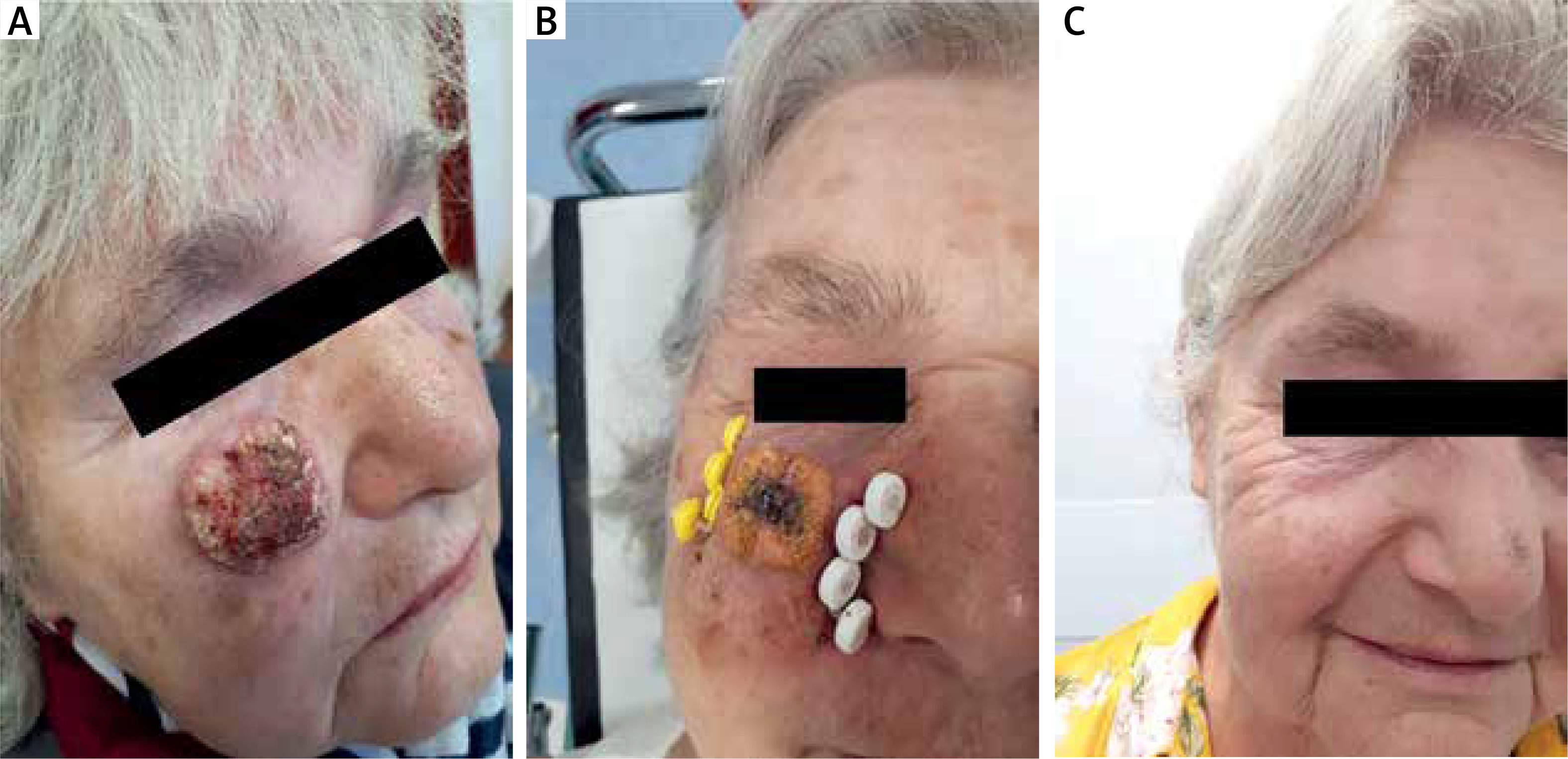
Figure 3
Squamous cell carcinoma before (A), during (B), and 2 years after (C) interstitial HDR brachytherapy. The patient received a total dose of 40 Gy in 10 fractions, administered twice daily
Among the 236 treated cancer lesions, 16 treatment failures were recorded (6.8%) – including 2 non-curable cases (0.8%, both in the same patient) and 14 recurrences (5.9%). The patient in whom tumour control was not achieved has been undergoing immunotherapy for over 2 years with a partial response. Both cases of lack of tumour control involved squamous cell carcinoma lesions. Of the 14 recurrences, 9 were basal cell carcinomas (4.9% of all basal cell carcinomas), and 5 were squamous cell carcinomas (9.8% of all squamous cell carcinomas). Overall, treatment failure occurred in 13.7% of squamous cell carcinomas. Lack of tumour control was observed 3 months after treatment, while recurrences occurred between 9 and 38 months post-treatment (mean: 17 months).
The relationship between selected clinical characteristics and treatment failure was analysed, but no statistically significant associations were found (Table 2). However, values approaching statistical significance were observed in relation to histological type, suggesting a higher risk of failure in squamous cell carcinomas.
Table 2
Risk of treatment failure depending on selected tumour and patient characteristics
All patients experienced an acute radiation reaction, initially presenting as erythema followed by ulceration, typically appearing around 14 days after the start of brachytherapy. The healing period ranged from 4 to 8 weeks. A late skin reaction was also observed at the site of each successfully treated lesion, characterized by skin thinning, depigmentation, and telangiectasia of varying severity. A serious complication in the form of skin necrosis within the irradiated area of the arm occurred in 1 (0.4%) case.
In the studied group of skin cancer patients, seven deaths were recorded during the follow-up period, including 1 patient who died due to metastatic uterine cancer. No deaths were attributed to skin cancer. Additionally, during follow-up, 1 patient was diagnosed with lung cancer and another with prostate cancer, both of which are currently undergoing treatment.
Discussion
According to data from the National Cancer Registry from 2021, 13,540 individuals in Poland were diagnosed with skin cancer (6,665 men and 6,875 women), and 180 deaths were reported due to this cause (97 men and 83 women) [11]. The incidence of skin cancers has been steadily increasing, with the main contributing factors including tanning, which became more popular, migration to regions with high sun exposure, UV radiation from artificial sources (tanning beds), and occupational exposure among individuals working outdoors without adequate photoprotection [1, 2, 4, 12]. The risk of developing skin cancer increases with age, particularly after the age of 80, although patients around the age of 65 account for 50% of all cases, and it is estimated that the majority of them will develop another lesion within 5 years [7, 12]. In the studied group, only 18.1% of patients were under 65. In some cases, the advanced age of patients in this cohort could have contributed to the loss of follow-up. An additional burden on patient monitoring was the fact that a significant part of the follow-up occurred during the SARS-CoV-2/COVID-19 pandemic, which impacted the frequency of follow-up visits and contributed to the relatively short observation period (median of 24 months).
Nevertheless, this does not diminish the value of brachytherapy in elderly patients, as this method enables good treatment outcomes even in advanced stages of cancer [13]. The vast majority (~80%) of skin cancer lesions are located in the head and neck area, which is associated with a high risk of recurrence after treatment [9, 12]. In the present analysis, more failures were also recorded in the high-risk area compared to the intermediate-risk area, although the difference was not statistically significant (p = 0.17). The lack of significance may be due to a distribution of lesion locations differing somewhat from literature data (only half of the lesions in the study group were located in the H zone). This is likely a result of patient selection for brachytherapy, which was most often used when effective surgical treatment was difficult to perform or when surgery would have caused disfigurement. Surgery remains the most effective treatment method for skin cancer. The Mohs technique is particularly valued for its high efficacy and favourable cosmetic outcomes. However, it is time-consuming and thus not widely used. For larger lesions or those located in specific parts of the body, optimal surgical treatment often requires general anaesthesia and complex reconstruction techniques.
HDR brachytherapy techniques have been evolving for the past 50 years and are now recognized as an effective method for treating skin cancers. They offer high cure rates with minimal complications and good cosmetic results. Recurrence rates reported by various authors range from 2% to 19% [4, 7, 14]. The number of publications on this topic is also growing [8, 14].
However, there are no randomized studies that would allow for a clear recommendation of the optimal total dose and the method of its fractionation. Most recommendations are based on clinical experience and expert opinions [6, 8, 14]. In the studied group, the fractionation method and total radiation dose were mainly based on the patient’s general condition, histopathological findings, tumour location, and ability to travel to the Opole Oncology Center. In cases where interstitial brachytherapy was used or outpatient treatment was not feasible, hospitalization and a twice-daily fractionation schedule were chosen, significantly reducing total treatment time. Fractionation schedule was also preferred in the treatment of squamous cell carcinoma lesions. No difference in treatment outcomes was observed depending on the fractionation method. HDR brachytherapy enables short treatment sessions in an outpatient setting, thereby avoiding prolonged hospital stays, which is particularly important for elderly patients.
Brachytherapy provides good cosmetic and functional outcomes. A literature review on acute and late complications and toxicity of skin brachytherapy showed that dermatitis is the most common acute side effect. In contrast, late side effects are mostly limited to hypopigmentation, telangiectasia, and alopecia [14, 15]. Similar reactions were observed in the studied patient group and, aside from 1 case of skin necrosis, did not affect the patients’ functionality. In the SCRiBE meta-analysis involving nearly 10,000 patients, brachytherapy was compared with external beam radiation therapy (EBRT) with equivalent dosing for T1-2 skin cancers, and similar local control rates were demonstrated. However, cosmetic outcomes were significantly better with brachytherapy [16]. Another meta-analysis (58 studies involving 21,000 patients) showed that cosmetic outcomes with brachytherapy are comparable to those achieved with the Mohs technique and superior to those obtained with EBRT or standard surgery [17]. The study material recorded a higher (though not statistically significant) failure rate for squamous cell carcinomas. However, the recurrence rates reported in meta-analyses for both types of skin cancer are similar [1]. The arbitrarily adopted minimum 1-year follow-up period after treatment is consistent with recommendations from other researchers and appears appropriate, especially for monitoring elderly patients [13, 14, 17].
When interpreting these results, some aspects of the study should be considered. The ambispective design may have been associated with incomplete data collection and a relatively short follow-up (median of 24 months, range: 12–67 months). Moreover, histopathological subtypes of BCC and SCC were not consistently reported, which could influence treatment outcomes; however, this reflects the ambispective nature of the study, evolving standards of histopathological classification, and limitations of available pathology reports. Finally, as this was a single-centre study, the generalizability of the findings may be somewhat limited. Despite these factors, the study provides valuable clinical insights into the role of brachytherapy in the management of skin cancers.
Conclusions
The high cure rate in the studied patient group indicates that brachytherapy is an effective method for treating skin cancers, regardless of the fractionation schedule used. Brachytherapy allows for excellent cosmetic results while preserving organ function when appropriately selected, especially in the head and neck region.







