
Introduction
Gastric cancer is considered the fourth most common in malignancies of the gastrointestinal tract and the second cause of deaths from malignancy worldwide [1, 2]. Gastric carcinoma was histopathologicaly classified into intestinal and diffuse subtypes according to Lauren classification. The management of patients with gastric cancer needs a multidisciplinary team which is based on surgery and chemo-radiotherapy. But it is still having a dismal outcome and it is associated with recurrence, failure of treatment and a higher mortality [2]. So, it is important to detect novel factors which could be considered novel prognostic markers for such a serious malignancy. Oxidative stress (OS) is found to be related to gastric mucosa damage and gastric carcinogenesis [3]. Oxidative stress and antioxidant capacity of tumors modulation is considered a novel promising treatment approach. Malignant cells are metabolically active and it could be able to generate huge amounts of reactive oxygen species (ROS) as products which are resulting from mitochondrial activity. Such oxidative stress is intrinsically harmful to tumor cells in case of absence of adequate defense mechanisms [4, 5], to antagonize the harmful effects of ROS and to maintain the oxidation-reduction homeostasis, the aerobic tissues must have a suitable antioxidant system. Sulfiredoxin (Srx), which is an endogenous antioxidant protein, was described as an enzyme in in yeast which could regulates the signaling pathways of reactive oxygen species, catalyzes peroxiredoxins (Prxs) reduction in presence of glutathione, ATP and thioredoxins [6]. Srx inhibition has been described as a novel management strategy against malignant tumors [7]. Nuclear factor erythroid 2-related factor 2 (Nrf2) is Cap-N-collar (CNC) transcription factors family member that have essential roles in regulation of antioxidant response. Nrf2 is one of the important inducers of production of the antioxidant enzymes. Its aberrant expression was found many tumor tissues [8]. PROX1 is a transcription factor and a key regulatory protein in the development and regulation of progenitor-cells in many organs and in cancer development. PROX1 was described to have either tumor-stimulatory or suppressive properties according to cancer type. PROX1 roles in malignant cells proliferation, migration, and invasion is unclear [9, 10]. There is no study which explored the detailed clinical, pathological and prognostic role of the oxidative stress markers: Srx, Nrf2 in addition to assessment of the expression of the transcription factor PROX1 in gastric cancer.
In the current study we aimed at analysis of levels of tissue expression of Srx, Nrf2, and PROX1 in gastric cancer and adjacent non-neoplastic gastric mucosa to clarify the relationship between their expression levels, clinical, pathological parameters and patients’ outcome.
Material and methods
Design of the study: a prospective cohort-study.
The setting of the study: Internal Medicine, General Surgery, Pathology, Medical Oncology and Clinical Oncology and nuclear Medicine Departments, Faculty of Medicine, Zagazig University Hospitals.
The type of materials involved: 70 paraffin-embedded samples: 50 specimens from gastric carcinomas and 20 specimens from adjacent non-neoplastic gastric mucosa.
The type of analysis used, Data analysis was performed using the software SPSS (Statistical Package for the Social Sciences) version 20.
Patients and tissue specimens
Our prospective cohort-study that was performed using 70 paraffin-embedded samples: 50 specimens from gastric carcinomas and 20 specimens from adjacent non-neoplastic gastric mucosa. Samples were taken from 50 patients with gastric carcinoma who were diagnosed and treated in in the period from May 2014 to May 2019. Malignant tissue specimens and specimens from non-neoplastic mucosa were collected after having a written informed consent from all studied patients. Ethics approval and written informed consent for the use of the specimens were provided by the Institutional Research Board (IRB) Committee of Faculty of Medicine, Zagazig University. None of the studied patients received any anti-cancer therapy before surgery.
Patients were evaluated by upper gastrointestinal tract (GIT) endoscopy and biopsies were taken to confirm the diagnoses of gastric cancer in Gastroenterology& Hepatology unit, Department of Internal Medicine. All cases were operated in Department of General Surgery by total or partial gastrectomy according to its stage. Specimens sent to Pathology Department, where patients were specimens were processed, diagnosed, evaluated, graded and staged. We have used the 8th edition of the American Joint Committee on Cancer staging system (AJCC-8) classification and the World Health Organization (WHO) classification for pathologic staging and a pathologic grading respectively [11]. Clinical, pathological and demographic data were collected through examination of the patient’s files. Surgery was performed for all operable patients followed by chemotherapy and radiotherapy. Patients were followed up for 5 years from May 2014 to May 2019 for assessment of recurrence, progression, response to therapy, disease free survival and overall survival. Patients’ follow-up records were obtained from Clinical Oncology and Nuclear Medicine Department and Medical Oncology Department.
Immunohistochemistry
We used automated method of immunohistochemistry (IHC) staining. Sections were cut from the collected paraffin tissue blocks, deparaffinized by putting them in xylene and rehydrated by putting them in descending grades of ethanol. The sections were put in EDTA (pH 8.0) for 12 min and then were boiled in a microwave oven for 2 min, the sections were incubated with primary rabbit polyclonal anti-SRXN1 antibody (ab203613), anti-Nrf2 antibody (ab31163), and anti-PROX1 antibody (ab101851) dilution (1 : 200) overnight at 4°C (Abcam, USA). Then, we have incubated the sections with secondary goat anti-rabbit antibody (1 : 1000) at room temperature for about two hours, and the degree of immune-stain was detected by using the DAB system (Santa Cruz Biotechnology, Santa Cruz, CA, USA). The sections were counterstained using hematoxylin. Mouse brain, placenta and human heart tissues were used as positive controls for Srx, Nrf2 and PROX1 respectively. Negative control used by omission of the primary antibodies and replacement by phosphate buffered saline [12].
Evaluation of Srx, Nrf2 and PROX1 expression
Positive cytoplasmic expression of Srx and PROX1 and positive nuclear Nrf2 expression were considered positive expression in tumor cells. To calculate Srx, Nrf2 and PROX1 immunoreactivity score (IRS) two pathologists independently evaluated the tumor tissue sections and sections of non-neoplastic mucosa in ten microscopic representative fields. To reach the final IRS multiplication of the score of staining intensity by the score of positively stained cells was done. The staining intensity was graded as: 0 = no stain, 1 = weak stain (light yellow), 2 = moderate stain (yellow brown) and 3 = strong stain (brown). The fraction of positive stained cells was graded as 0 = no positive cells, 1 = 10% or less positive cells, 2 = 11–50% positive cells, 3 = 51–80% positive cells, or 4 = 80% or more positive cells. The total final IRS ranged from 0 to 12 and it was divided into two levels: low immunoreactivity when the total IRS is 0–4 and high immunoreactivity when the IRS is higher than 4 [3, 6].
Statistical analysis
Quantitative variables were described using their means and standard deviations. Categorical variables were described using their absolute frequencies and were compared using χ2 test. Kolmogorov-Smirnov (distribution-type) and Levene (homogeneity of variances) tests were used to verify assumptions for use in parametric tests. To compare means of two groups: independent sample t test was used for normally distributed data and Mann-Whitney test was used when data is not normally distributed. Kaplan-Meier plot was used to measure the survival rates. The level statistical significance was set at 5% (p < 0.05). Highly significant difference was present if p ≤ 0.001.
Results
Patient clinicopathological characteristics
A total of 70 samples are taken from 50 gastric carcinoma patients. As regard patients clinicopathological features there were 34 (68%) patients ≥ 60 years old (mean ±SD 456.84 ±7.93), median 57 (39–72).
We included 37 (74%) male patients. Histopathological examination revealed 20 specimens of non-neoplastic gastric mucosa, 45 (64.3%) cases of intestinal adenocarcinoma, and 5 (7.1%) cases of diffuse carcinoma. High grade was found in 10 cases and distant metastases were found in 4 patients. Curative surgery was performed in most cases and adjuvant therapy was given according to the stage.
The detailed clinic-pathological data of our patients were fully illustrated in Table 1.
Immunohistochemical results
Srx expression
High Srx expression was found in 29 (58%) of gastric carcinoma and in 3 (15%) specimen of normal gastric mucosa. Srx was up-regulated in gastric carcinoma tissue than adjacent non-neoplastic mucosa (p < 0.001)
High levels of Srx expression was found in 29 (58%) of gastric carcinoma and high expression was positively associated with higher cancer grade (p = 0.006), presence of lymph nodes metastases (0.04), advanced stage (p < 0.001) and higher incidence of occurrence of distant metastases (p = 0.029). but we have not found any significant associations between Srx expression and age or sex of the patient, initial site or size of the tumor or histopathological subtype. All data regarding Srx expression and association with clinicopathological findings was detailed in Tables 1–3 and in Figure 1.
Fig. 1
Immunohistochemical expression of sulfiredoxin (Srx) in gastric carcinoma (GC). A) High cytoplasmic Srx expression in poorly differentiated GC intestinal type ×400. B) High cytoplasmic Srx expression in moderately differentiated GC intestinal type ×400. C) High cytoplasmic Srx expression in poorly differentiated GC diffuse (signet ring subtype) ×400. D) Low cytoplasmic Srx expression in well differentiated GC intestinal type ×400. E) Negative cytoplasmic Srx expression in well differentiated GC intestinal type ×400. F) Negative cytoplasmic Srx expression in adjacent non-neoplastic gastric mucosa ×400
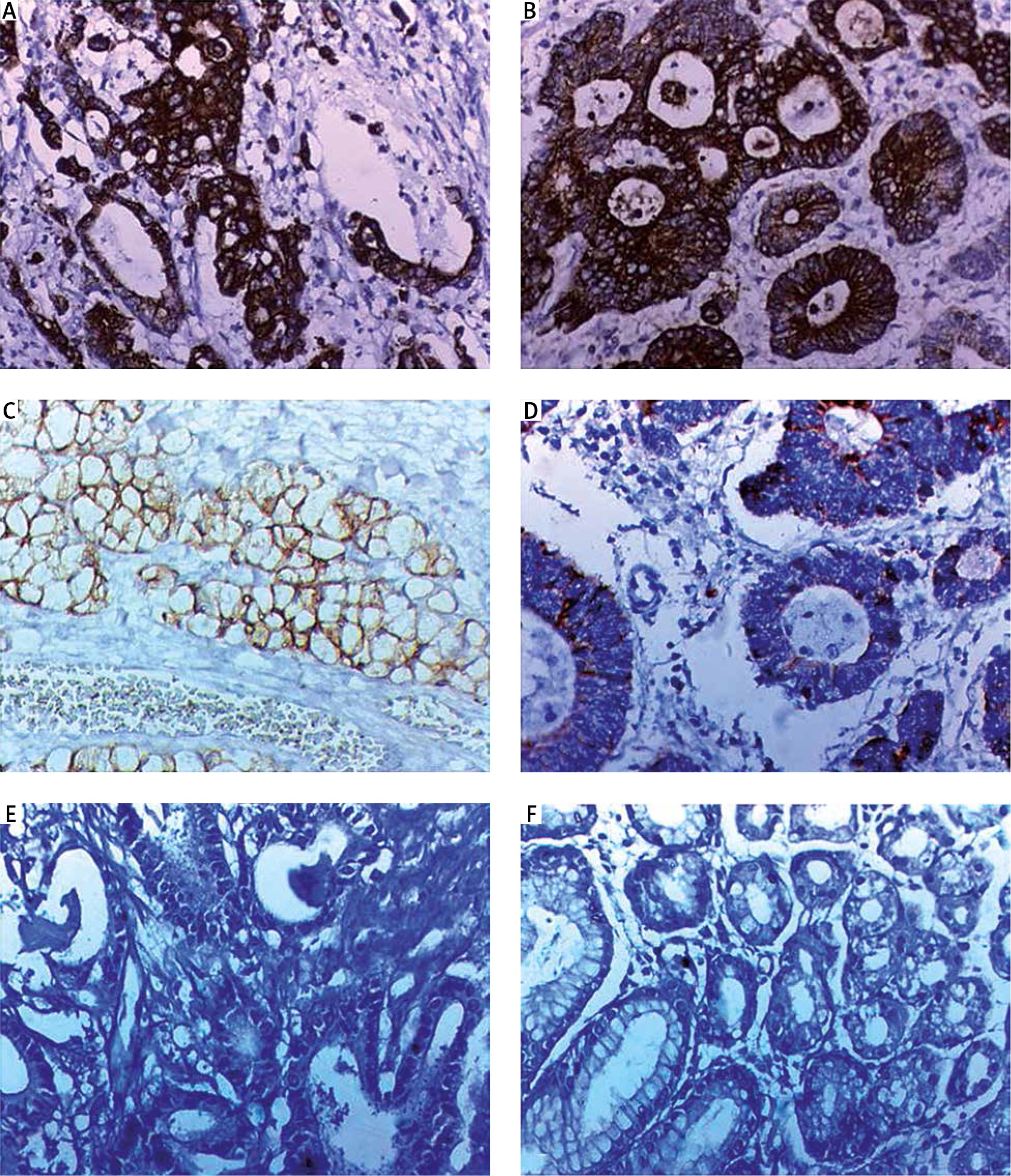
Table 2
Distribution of the studied samples according to levels of Srx, PROX1 and Nrf2
Table 3
Correlation between Srx, PROX1 and Nrf2 levels in the studied gastric cancer patients and their demographic and histopathological parameters
Association between disease progression, patients’ survival and Srx expression
Srx higher expression in tissues of included patients was positively associated with good response to treatment, lower levels of complete disease remission (p = 0.002), occurrence of relapse (p = 0.004), poor disease free survival (p < 0.003), dismal outcome and poor overall survival (p < 0.001). All data regarding Srx expression and association with follow-up findings was detailed in Figure 2 and Tables 4 and 5.
Fig. 2
Kaplan-Meier survival curves of disease-free survival (DFS) and overall survival rate (OS) of the studied in gastric carcinoma (GC) patients. A and B) DFS and OS rates of the studied GC cases stratified according to Srx expression respectively, C and D) DFS and OS rates of the studied GC cases stratified according to Nrf2 expression respectively, E and F) DFS and OS rates of the studied GC cases stratified according to PROX1expression respectively
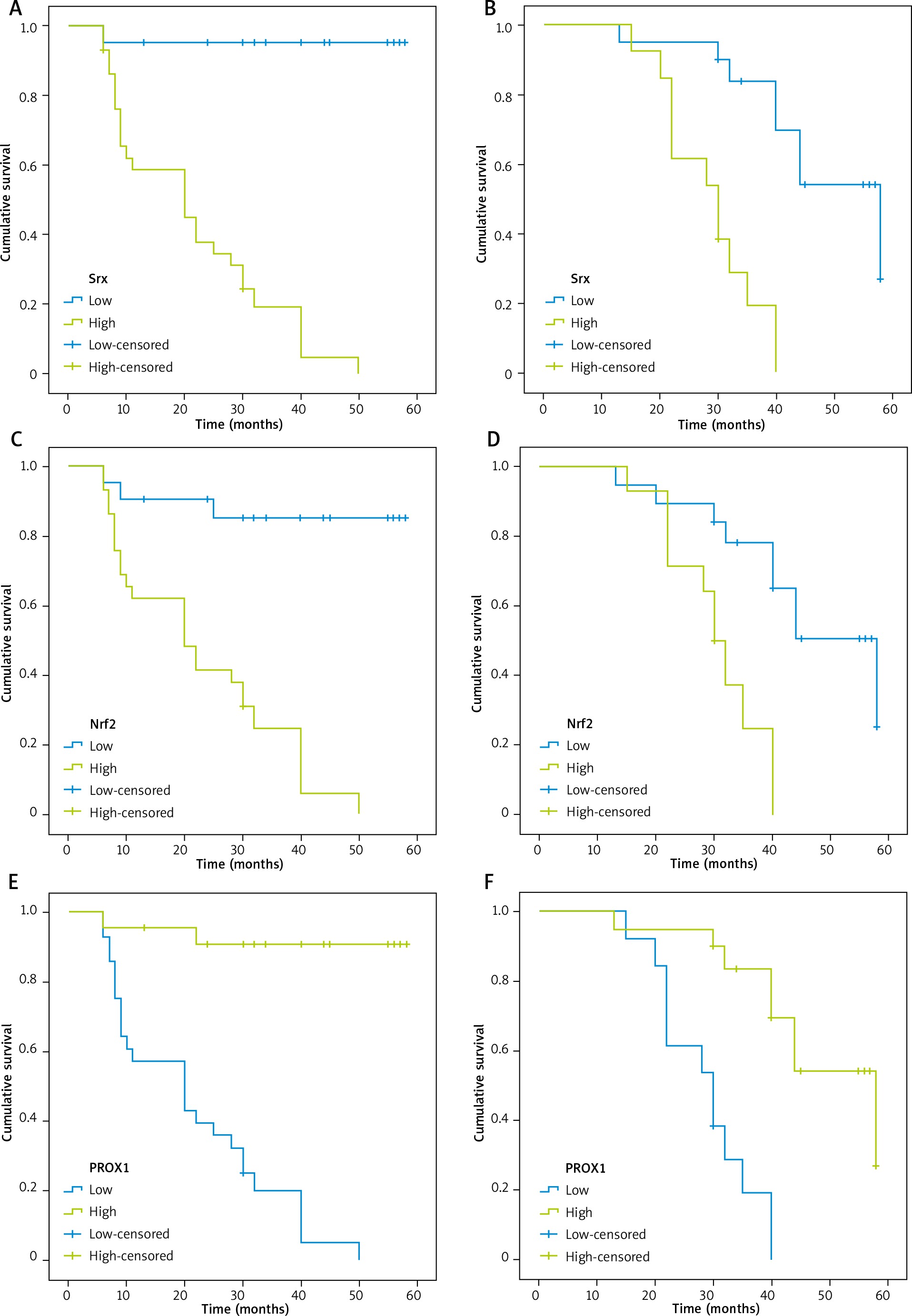
Table 4
Correlation between Srx, PROX1 and Nrf2 levels in the studied patients and treatment-specific characteristics and patients’ outcome
Table 5
Correlations between Srx, PROX1 and Nrf2 levels in the studied gastric cancer patients and their outcome
Nrf2 expression
High Nrf2 expression levels was found in 29 (58%) of gastric carcinoma and in 2 (10%) specimen of normal gastric mucosa. Nrf2 was up-regulated in gastric carcinoma tissue than adjacent non-neoplastic mucosa (p < 0.001)
High levels of Nrf2 expression was found in 29 (58%) of gastric carcinoma and high expression was positively associated with higher cancer grade (p = 0.031), advanced stage (p = 0.02) and higher incidence of distant metastases (p = 0.03), but we have not found any significant associations between Srx expression and age or sex of the patient, initial site or size of the tumor or histopathological subtype or presence of lymph node metastases. All data regarding Nrf2 expression and association with clinicopathological findings was detailed in Tables 1–3 and in Figure 3.
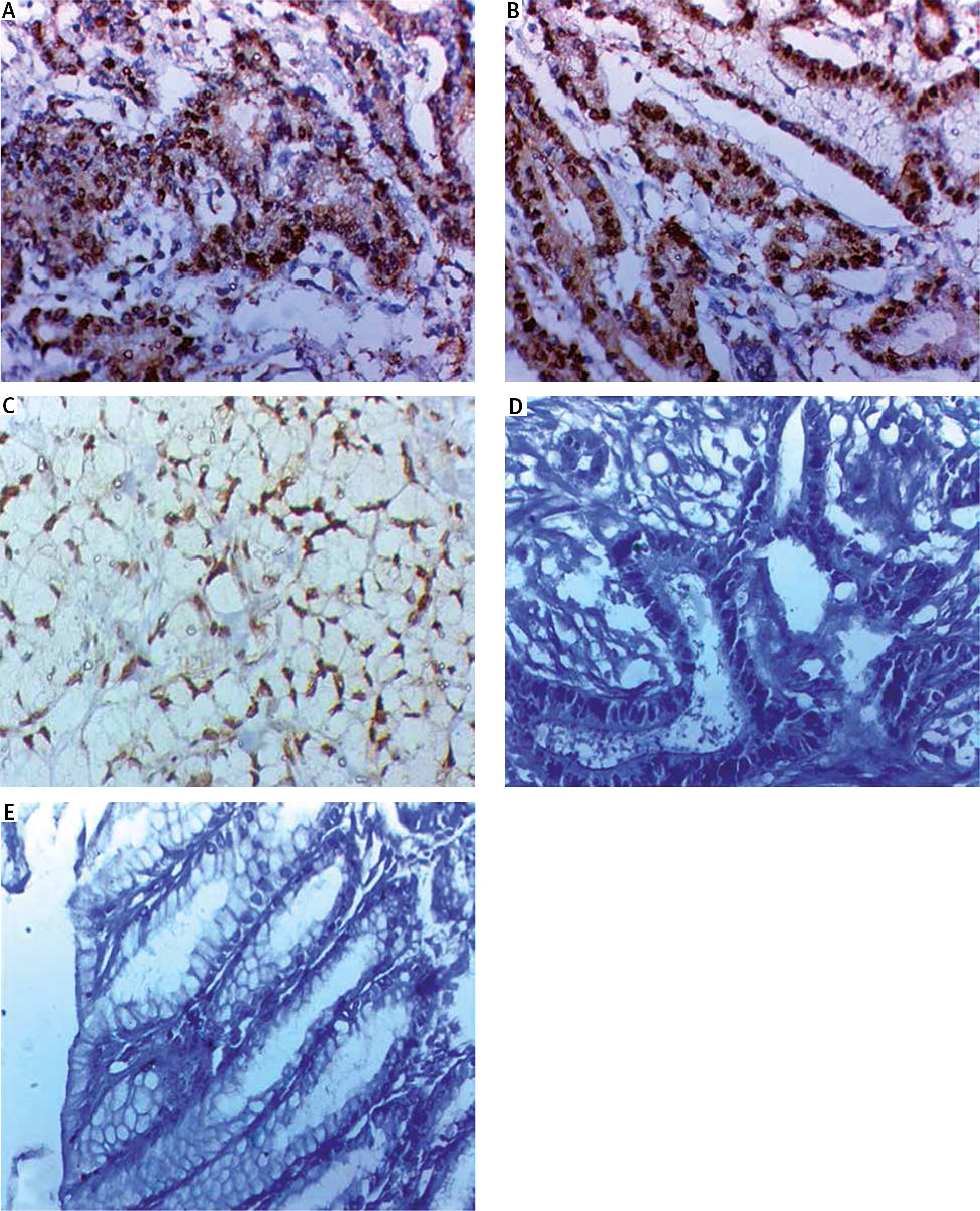
Fig. 3
Immunohistochemical expression of nuclear factor erythroid 2-related factor 2 (Nrf2) in in gastric carcinoma (GC). A) High nuclear Nrf2 expression in poorly differentiated GC intestinal type ×400, B) high nuclear Nrf2 expression in moderately differentiated GC intestinal type ×400, C) high nuclear Nrf2 expression in poorly differentiated GC diffuse (signet ring subtype) ×400, D) negative nuclear Nrf2 expression in well differentiated GC intestinal type ×400, E) negative nuclear Nrf2 expression in adjacent non-neoplastic gastric mucosa ×400
Association between disease progression, patients’ survival and Nrf2 expression
Nrf2 higher expression in tissues of included patients was positively associated with good response to treatment, lower levels of complete disease remission (p = 0.017), occurrence of relapse (p = 0.04), poor disease free survival (p = 0.005), dismal outcome and poor overall survival (p < 0.001). All data regarding Nrf2 expression and association with follow-up findings was detailed in Tables 4 and 5 and in Figure 2.
PROX1 expression
PROX1 high expression was detected in 22 (44%) of gastric carcinoma and in 15 (75%) specimen of normal gastric mucosa. PROX1 was decreased in gastric carcinoma tissue than adjacent non-neoplastic mucosa (p = 0.019).
PROX1 high expression was associated with lower cancer grade and lower T stage (p = 0.005), absence of lymph nodes metastases (p = 0.023) and early stage (p = 0.003), but we have not found any significant associations between PROX1 expression, patients age or gender, primary tumor site, size or histopathological subtype or presence of distant metastases. All data regarding PROX1 expression and association with clinicopathological findings was detailed in Tables 1–3 and Figure 4.
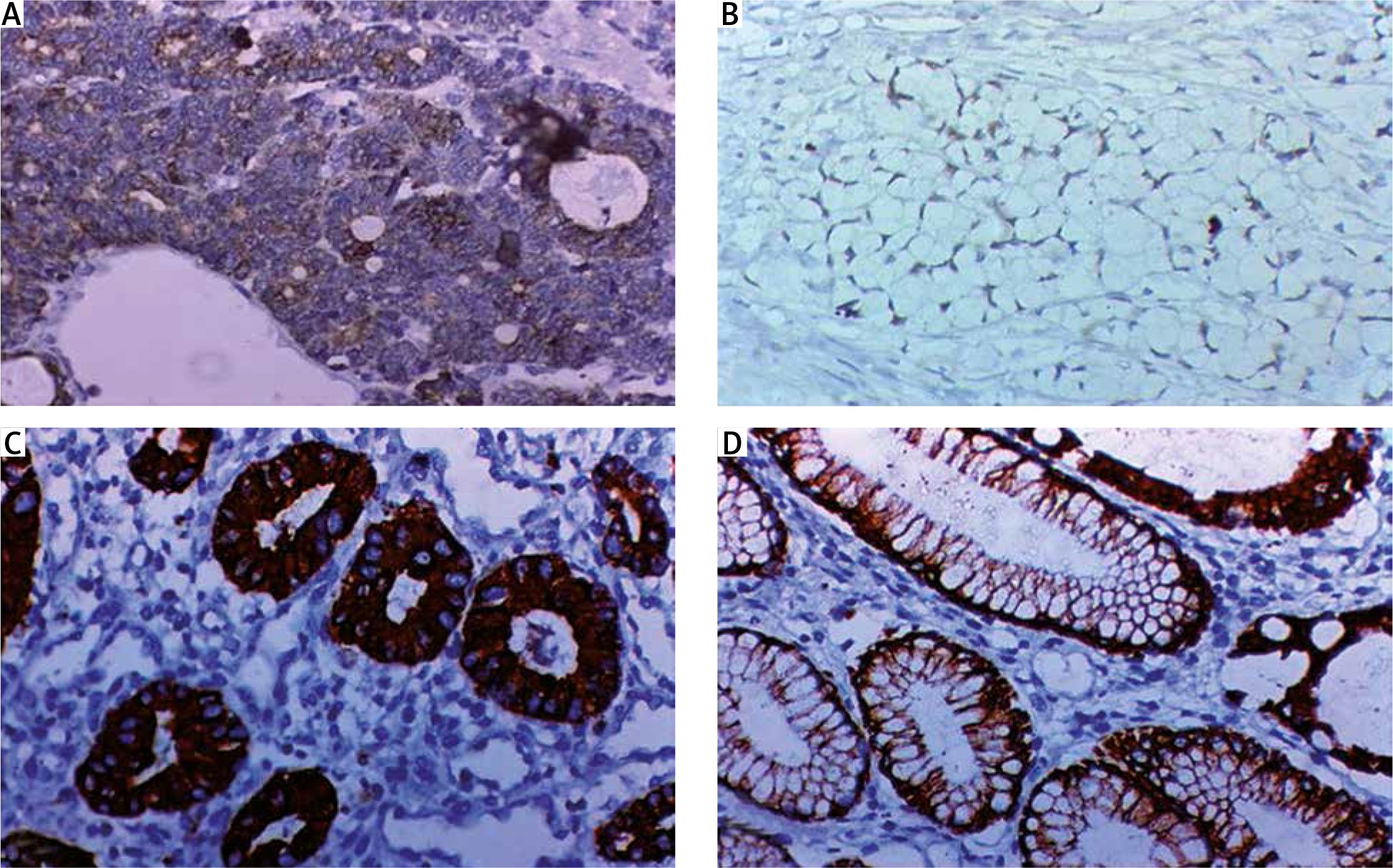
Fig. 4
Immunohistochemical expression of PROX1 in gastric carcinoma (GC). A) Low cytoplasmic PROX 1 in poorly differentiated GC intestinal type ×400, B) low cytoplasmic PROX1 in poorly differentiated GC diffuse (signet ring subtype) ×400, C) high cytoplasmic PROX1 expression in well differentiated GC intestinal type ×400, D) high cytoplasmic PROX1 expression in adjacent non-neoplastic gastric mucosa ×400
Association between disease progression, patients’ survival and PROX1 expression
PROX1 expression levels in included patients were positively associated with higher incidence of response to therapy, complete remission, good disease free survival rate (p = 0.003), absence of disease recurrence (p = 0.004), and longer overall survival rate (p < 0.001) (Tables 4 and 5, Fig. 2).
High level of Srx increases risk of mortality by a270 fold while low level of PROX1 increase that risk by 130 fold and high level of Nrf2 increases risk of mortality by 37.5 folds. All data regarding PROX1 expression and association with follow-up findings was detailed in Tables 4 and 5 and in Figure 2.
There were inverse associations between Srx and PROX1 and between Nrf2 and PROX1. There is strong positive correlation between Srx and Nrf2 in included patients. Phi co-efficient = –0.96, –0.797 and 0.836 respectively (p ≤ 0.001).
Discussion
Identification of novel prognostic biomarkers for gastric cancer is needed for improving management strategies and the post-operative recovery [13]. Oxidative stress (OS) became wide¬ly accepted mechanism which has been incriminated in gastric carcinogenesis, due to its role in DNA damage and injuries of the normal mucosa [14].
In this study, we used the immunohistochemistry technique to determine levels of expression of related two oxidative stress markers: Srx and Nrf2 correlate their expression with each other, with another transcription factor: PROX and correlate their expression with pathological parameters and patients’ outcome.
We have found that Srx expression was higher in cells of gastric cancer more than adjacent non-neoplastic gastric mucosa, and its expression was related to unfavorable pathological and prognostic parameters in gastric cancer patients. Wang et al. [2] showed a similar finding by proving that the levels of expression of Srx protein were elevated by increasing the oxidative stress in gastric cancer cells. Similarly, Chen et al. [6] and Lan et al. [15] proved the increased Srx expression in cervical cancer tissues it was associated with unfavorable patients outcome. Similar results were previously shown in various cancer types [16]. The role of Srx/Prx axis in promotion of invasion, progression and spread of lung cancer is pointing to using Srx as a target for prevention and treatment of cancer [17].
Follow-up results of our gastric cancer patients that were shown in the current study showed that differences in DFS rate between patients with higher and lower Srx expression levels was statistically significant, and patients having high Srx expression levels, had a worse survival rates and unfavorable prognosis more than patients with low Srx expression. Srx over-expression patients had higher rates of cancer recurrence and metastasis, which was similar to results of Chen et al. [6].
Srx is considered a major antioxidant in normal non-neoplastic cells but its upregulation in cancer cells indicated an abnormal redox status which indicated that Srx is considered a major marker of oxidative stress than having antioxidan+t properties.
The role of Srx in gastric oncogenesis is still unknown, but its higher expression levels in advanced, high stage, recurrent gastric cancer pointed to its role in increasing oxidative stress from non-neoplastic gastric mucosa to high grade and advanced stage gastric cancer.
Srx has been found to be a target gene for activator protein-1 (AP-1), that is required for malignant transformation in several cancer tissues but not in their neighboring non-neoplastic tissues [18].
Srx was found to induce cancer by epithelial mesenchymal transition (EMT) induction through down regulation of E-cadherin in cervical cancer cells [6]. Moreover, Wnt/β-catenin pathway is involved in Srx oxidative stress related cancer cell survival [15]. Many signaling pathways are needed for cancer development through Srx mediated induction of EMT, e.g. tumor growth factor (TGF)-β, Notch and Nrf2 [19], In addition, Nrf2 polymorphisms could be involved in control of Srx levels and its role in malignant induction [20]. As there are no detailed studies about the expression of Srx and Nrf2 in gastric cancer cells so we tried to assess their expression correlating their expression with each other and with pathological parameters and gastric cancer patients’ outcome.
Nrf2 is a major cellular defense mechanism due to its antioxidant role which to protects normal cells from many damaging oxidative conditions, but its overexpression in cancer cells leads to activation of many downstream genes which facilitate proliferation, invasion of cancer cells and prolong their survival [3]. In the current study, Nrf2 nuclear expression was up regulated in gastric cancer tissues more than adjacent non-neoplastic tissues. Furthermore, we found significant correlations between Nrf2 expression and unfavorable clinicopathological factors in gastric cancer. Our findings are in accordance with Kawasaki et al. [3] and Zheng and Nong [21] in gastric cancer tissues that showed the association with gastric cancer progression. Similarly, Kari et al. [8] and Yi et al. [22] showed that in diffuse large B cell lymphoma (DLBCL) patients high nuclear Nrf2 expressions are also associated with higher stage and adverse outcome when compared with its expression in reactive lymph nodes. Kawasaki et al. [3] showed that continuous high expression levels of Nrf2 in gastric cancer tissue might result in production of antioxidants, which allow these cancer cells to antagonize the presence of a huge amount of reactive oxygen species (ROS) giving cancer cells higher malignant properties through this mechanism.
Hu et al. [23] similarly showed the presence of a prognostic significance of tissue expression in Nrf2 in gastric cancer that was similar to our results. But, they assessed only its cytoplasmic expression in malignant cells. This different result may be due to they were using different primary antibodies from the antibodies that we have used in the present study. Our localization of Nrf2 in the nucleus is more accurate as it was previously demonstrated that Nrf2 exerts its antioxidant roles in cancer cells only when it translocates from the cytoplasm to the nucleus [24]. Our results were similar to Kawasaki et al. [3] who showed that Nrf2 was located in the nucleus of cells of gastric cancer and that its persistent overexpression in the nucleus likely worked as an antioxidant which could be able to protect the cells of gastric cancer from harmful effects of ROS, which reflected aggressive behavior of gastric cancer. So, it is essential to assess only nuclear expression of Nrf2 in tissues derived from of gastric cancer patients. Overexpression of Nrf2 is associated with unfavorable survival rates in several solid cancers [25, 26].
Similarly, Solis et al. and Wang et al. showed that high Nrf2 expression was elated to poor outcome in lung carcinoma [27] and in gallbladder cancer [28], respectively. Nrf2 over expression may be able to prolong the survival of cancer cells following chemotherapy and radiation therapy and positive Nrf2 expression was associated with resistance to 5FU based chemotherapy [3]. So, evaluating the expression level of Nrf2 predicts patients who could benefit from receiving postoperative neo-adjuvant chemotherapy in gastric cancer cells.
Cho et al. reported that inhibition of Nrf2 resulted in cancer cells sensitization to anticancer alkylating agents [29]. Furthermore, Ma et al. stated that the combination of cisplatin and inhibition of Nrf2 significantly inhibited tumor growth [30].
Nrf2 plays a role in protecting the body cells from the oxidative stress. Nrf2 was found to have a dual role in both preventing and promoting oncogenesis making it a candidate factor for tu¬mor growth and invasion [21], suggesting the benefits of using Nrf2 as a prognostic index for evalu¬ating the postoperative outcome of patients. Other than its role as oxidative stress marker, Nrf2 might allow chemo-resistance through induction of abnormalities in cell cycle and up-regulation of multidrug resistance- related protein transporters,[8] immunosuppression [31] and reduced sensitivity to radiotherapy [32]. Oncogenes such as Kras, Braf and Myc stimulate the expression of Nrf2 [30]. These findings suggest that Nrf2 expression might be used as a prognostic and predictive parameter for the postoperative survival of gastric cancer patients. We have found a positive association between Srx expression and Nrf2 expression of gastric carcinoma and high expression of both of them is related to unfavorable patients outcome suggesting their role in induction of oxidative stress and EMT in gastric cancer progression. We assessed the expression of another transcription factor: PROX which was involved in progression of many gastrointestinal tract tumors [33], in Kaposi sarcoma [34], and in brain tumors [35]. The role of PROX1 in cancer is variable depending on its subtype as it might have tumor promoting or tumor inhibiting role. In the current study we have found that PROX1 expression was down regulated in gastric cancer tissues than adjacent non-neoplastic mucosa and that it was related to favorable pathological parameters and better patients outcome, which is similar to Laitinen et al. [9] in gastric cancer, who found that high PROX1 expression served as a favorable prognostic marker and patients with high PROX1 immunoreactivity had a better survival rate.
Moreover, we have showed that patients with gastric cancer, who had high expression of PROX1, have a favorable survival rate than those with low expression which is similar to Petrova et al. [35] findings in colon cancer.
In cancer colon, PROX1 has an important role in cancer progression and is associated with poor patient outcome [33]. In carcinoma of the liver [37], pancreatic cancer [38] and gall bladder carcinomas [39], increased PROX1 expression is associated with better prognosis. Moreover, in esophageal cancer cells, increased expression of PROX1 leads to reduction of tumor cell proliferation [40]. Additionally, it was found that miR-489 dysregulation lead to gastric cancer progression, it is markedly down regulated in such malignancy and PROX1 was a direct miR-489 [41].
We have showed that PROX1 was evenly expressed in the cytoplasm. Previous studies showed that it could be found in the nucleus and cytoplasm of the tumor cells [10]. But similar to our results cytoplasmic PROX1 expression has been related to PROX1 mRNA amplification [42]. The stained region of the tumor cells varied according to the subtype of cancer as it is mainly located in the nucleus of tumor cells in colon cancer, liver cancer and in glioma [33, 36, 43], while it was found to be cytoplasmic in gastric cancer and pancreatic cancer [9, 37]. PROX1 is activated in the cytoplasm before translocation to the nucleus [33]. Cell proliferation was inhibited by knockdown of PROX1, suggesting that PROX1 might reduce apoptosis and reduce gastric cancer cells proliferation [10].
Conclusions
It might be clinically beneficial to develop novel prognostic biomarkers for gastric cancer to predict invasion and metastasis.
High expression of Srx and Nrf2 could be able to decrease gastric cancer patients’ survival rates via facilitation of tumor cell resistance to therapy. So evaluation of their expression in gastric cancer patients might be able to help in optimizing the chemotherapy plan. We have also demon¬strated a positive association between Srx and Nrf2 expression and gastric cancer invasiveness, suggesting their utility as poor prognostic markers. Additionally, our study showed that expression of PROX1 serves as a favorable prognostic marker of gastric cancer patients.
Limitations of the study
The study included relatively little number of cases and this is because the study was performed in a single university so patients’ number was according to number of operated cases in such hospital and was having complete follow-up data. We used immunohistochemistry for evaluation of tissue protein expression of evaluated markers cases which was assessed semiquantitively without gene assessment. There are many inoperable cases where samples were taken from them by endoscopy and surgical samples were taken during palliative surgery to bypass gastric outlet obstruction which could not allow us to adequately evaluate number of lymph nodes or accurate staging.






