
Purpose
Squamous cell carcinoma (SCC) is a common malignancy derived from epidermal keratinocytes. It is estimated that over 700,000 new cases of SCC are diagnosed annually [1]. The most common presentation is localized, highly curable disease with locoregional or distant metastases developing in less than 5% of cases [2,3]. SCC can develop on any cutaneous surface although the most common sites are those exposed to the sun. The rate of SCC in the arm or hand is estimated at 3% [4].
Treatment is primarily determined by risk of locoregional recurrence and metastasis. Treatment options include surgical excision, cryotherapy, electrosurgery, topical treatment, radiation therapy, and photodynamic therapy, with surgery being the most frequent treatment due to low rates of recurrence [5]. In terms of radiation therapy, different techniques can be used such as electron beams, megavoltage photons, low-dose-rate (LDR) or high-dose-rate (HDR) brachytherapy [6]. The treatment optionality is based on institutional resources and radiation oncologist expertise.
Radiation therapy is an effective alternative to surgery. While EBRT can be performed, tissues of the hand do not often tolerate cancercidal doses of radiation and damage to the skin and underlying tendons and bones may produce a poor cosmetic and functional result [7]. There is very limited literature regarding treatment of non-melanoma skin cancer using HDR brachytherapy. Also, these reports on HDR brachytherapy concern delivery via a surface mold and not interstitial catheters. Surface mold techniques have shown comparable tumor control to surgery with good cosmetic and functional outcomes [8,9,10,11,12,13,14].
The role of interstitial brachytherapy for SCC involving the hand has not been well defined. The purpose of the study is to report the treatment of SCC using interstitial and surface HDR brachytherapy to obtain tumor control and preserve organ function. To our knowledge, this is the first such report in the literature that shows the use of interstitial catheters to deliver HDR brachytherapy for recurrent cutaneous SCC.
Material and methods
Patient
The patient was a 48-year-old woman who worked as a healthcare professional with a medical history notable for four renal transplantations for idiopathic renal failure beginning at age eight. She was on chronic immunosuppression with tacrolimus and mycophenolic acid. She presented initially with cutaneous SCC two years previously with a nodule of the dorsal right hand involving the 3rd and 4th webspace. Biopsy confirmed squamous cell carcinoma and she underwent Mohs resection of the mass with subsequent reconstruction with chest wall flap. Resection included at least partial excision of the ring finger radial digital nerve due to perineural invasion. A year later, she noted a recurrent mass of the same webspace and underwent re-resection with negative margins. Over the next several months, the mass slowly re-grew in the same webspace, prompting a biopsy with pathology consistent with recurrent SCC. Magnetic resonance imaging (MRI) at that time showed a dorsal mass to the interspace between the heads of the third and fourth metacarpals measuring approximately 7 mm transverse × 5 mm volar-dorsal × 16 mm proximal-distal. The tumor significantly involved the webspace with some penetration of the lesion into the volar neurovascular bundle. Clinically, there was suspicion of dorsal, dermal invasion; however, MRI did not show bone invasion. She was seen in consultation at an outside institution where single (4th digit) to double ray resection (3rd and 4th digits) was recommended.
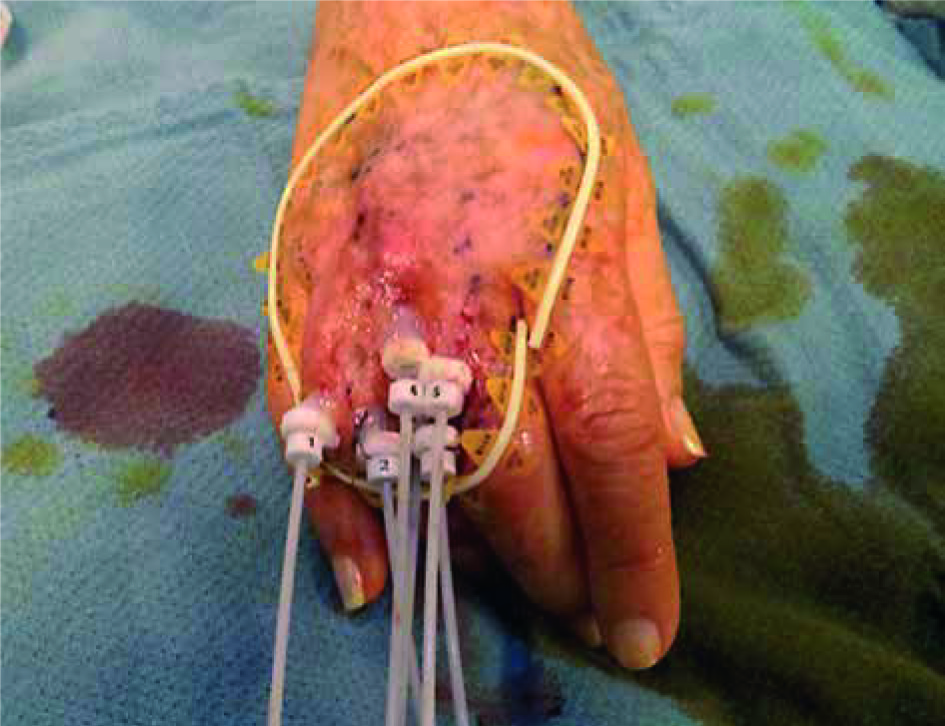
The patient presented to our institution for a second opinion. The recommendation of upfront surgical management was reinforced. As the patient refused ray amputation due to functional loss and cosmetic deformity, the option of initial external beam radiation therapy followed by surgical tumor debulking was discussed. The potential serious complications of surgery and radiation therapy were discussed in detail [15]. Due to the increased risk of wound healing complications, significant impairment of lymphatic drainage, fibrosis, swelling, and continued pain which could have limited the function of her hand, she declined this option as well. The option of EBRT alone using electrons was proposed. An initial plan using electrons was generated but the dose inhomogeneity was deemed unacceptable given the complexity of the target. Subsequently, she was referred to the brachytherapy group for consideration of interstitial brachytherapy (Figure 1). After much discussion, a plan of surface and interstitial HDR brachytherapy was generated with the goal of balancing tumor control with preserving organ function.
Treatment planning
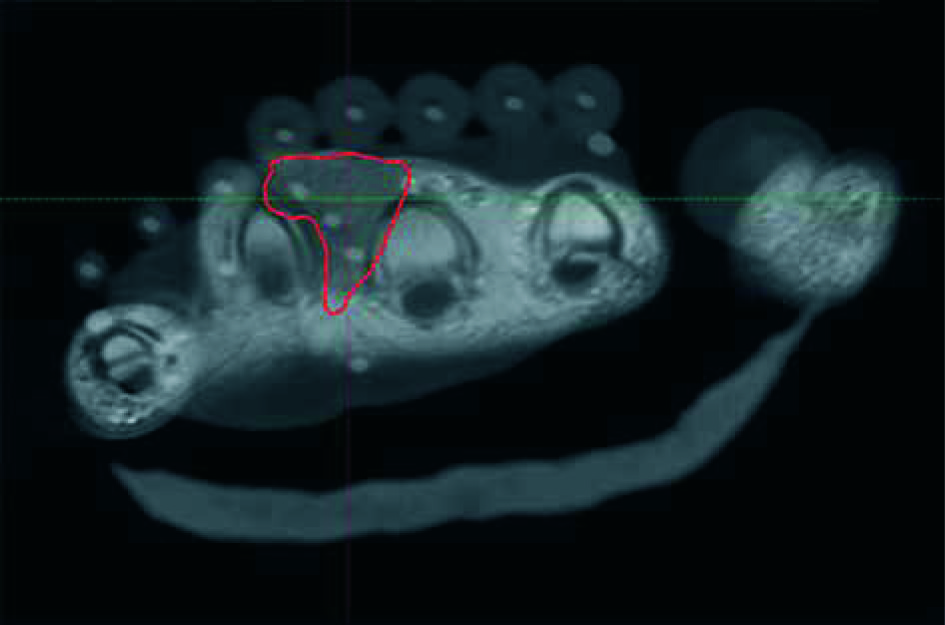
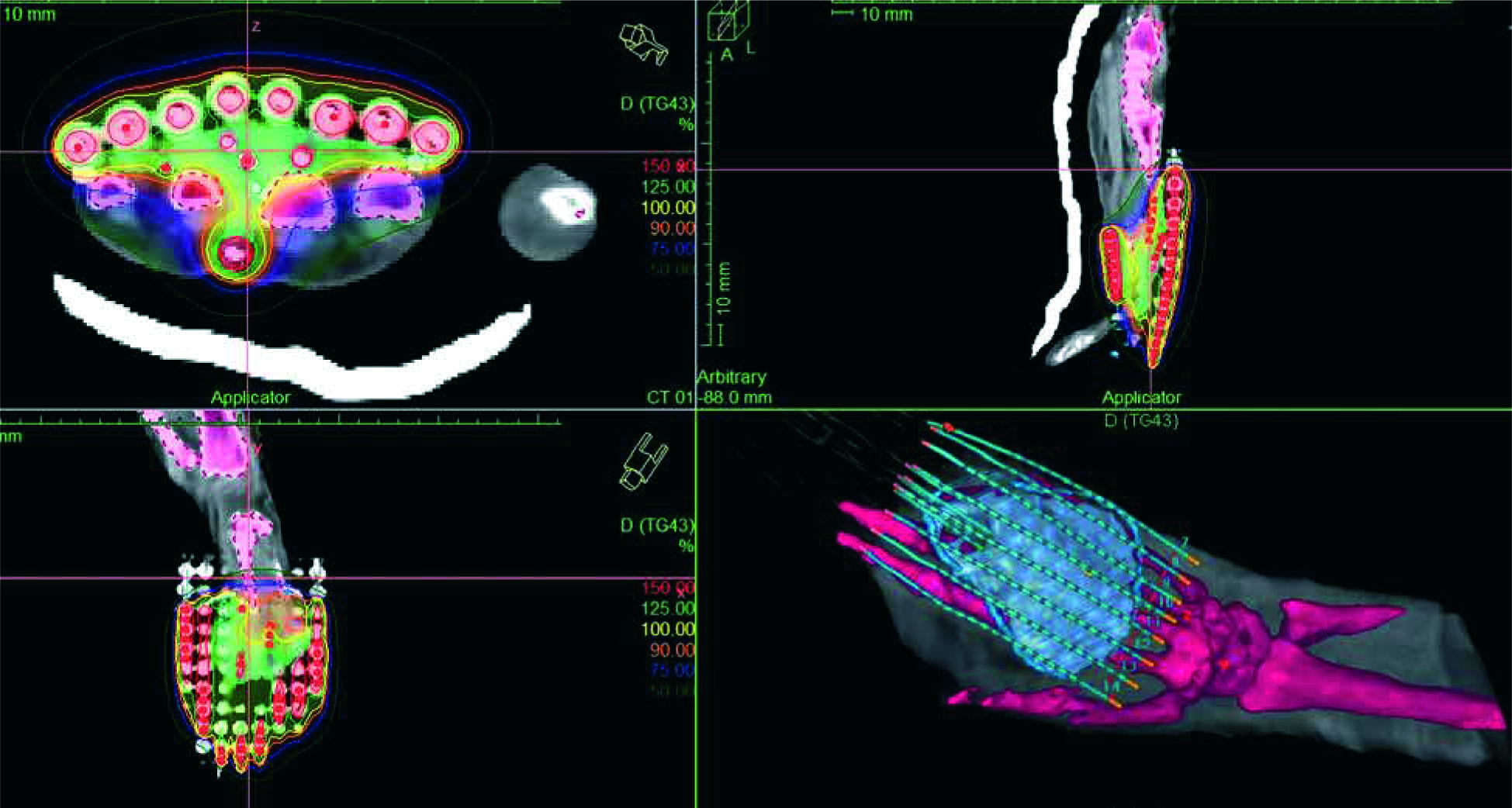
The Oncentra Brachy (Ver. 4.3., Elekta Brachytherapy) treatment planning system (TPS) was used for 3D treatment plan generation. A CT image set with a 1.25 mm slice thickness was used to allow for accurate digitization of the catheter. The prescription dose for the HDR treatments was 40.5 Gy in 9 fractions to the clinical target volume (CTV) [7]. The CTV was defined by the wire for the surface part (as seen in Figure 1). The subcutaneous part of the target contains the interspace between the heads of the third and fourth metacarpals (as seen in Figure 2). The prescription dose was planned to be delivered using 5 mm step size sequencing. The applicator consists of the two components: a) flap applicator (Freiburg Flap, Elekta Brachytherapy) with 8 catheters, and b) six 1200 mm ProGuide (Elekta Brachytherapy) interstitial needles. The flap applicator was clinically placed at the surface of the back of the hand. The flap applicator was used in a standard manner in the treatment planning phase to deliver the prescription dose to 3 mm under the skin to reach the dermis and spare unaffected stem cells and vasculature. Therefore, the treatment plan was initially normalized to the depth of 3 mm maintaining an equidistant position of 8 mm between the source dwell positions and normalization points. The interstitial needles were used to bring the dose to the depth forming the T-shape isodose distribution around the proximal phalanges (Figure 3). The distal position of the source in the TPS was determined using two independent measurements. The length of all 14 catheters was measured using the source position simulator (SPS). The length of marking wires for each catheter was compared against the values obtained with the SPS to reach a tolerance level of 1 mm. Only dwell position inside the clinical target was activated to minimize the dose to the healthy tissue. Strictly local graphical optimization of the dose was applied due to the small size and complicated topology of the target. Paraxial, parasagittal, paracoronal views were used to evaluate dose distributions over the 3D volumes. The relevant dosimetric parameters such as V100, V150, V200, D90 and D95 for the CTV were collected. In addition, V100, V150, V200, and D2cm3 for the bone were recorded to evaluate the patient dosimetry. The dose calculation was performed using the TG-43 formalism that includes the anisotropy corrections. Heterogeneity corrections were not included in the brachytherapy dose calculation.
Results
Treatment delivery
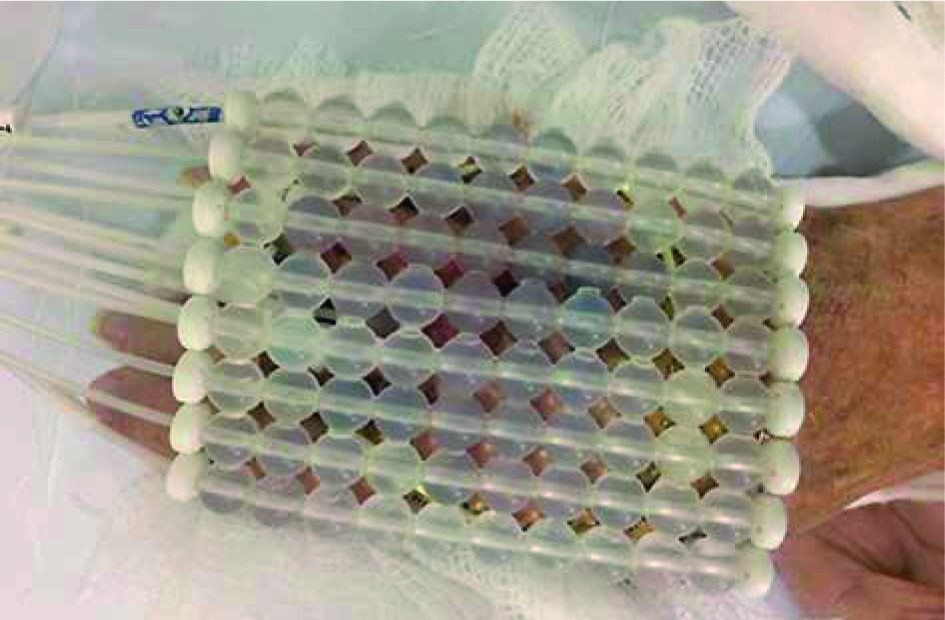
To minimize uncertainties during immobilization, self-adherent wraps, and towels for additional support were used (Figure 4). The setup was verified against the clinical photograph taken on the day of simulation. The position of the flap applicator with respect to the interstitial needles was verified prior to each fraction using CT images. The planning CT images were compared against the pretreatment CT images. Pretreatment CT images were used to evaluate possible gaps between the skin and surface applicator. The treatment plan was generated to maintain a maximum dose at the skin of 125% of the prescription dose, so the position of the applicator was carefully verified to maintain the desired dosimetry. The patients tolerated the treatment well in the sitting position. The patient did not experience discomfort during pretreatment preparation or during the delivery of the radiation dose. The treatment time for the last (9th) fraction was 403 s, which was 20 s longer relative to the first received treatment. Therefore, the extended number of fractions did not result in a significant increase of the treatment time.
Fig. 4
Treatment delivery setup (prior to immobilization using self-adherent wrap). Freiburg flap applicator is placed to the surface of the CTV
Total treatment time was 383 s when the source activity was 6.2 Ci (air kerma strength equals 25.208 mGy-m2-h-1). The total time lost due to rounding of the dwell times was negligible (0.7%). All 8 catheters from the flap applicator contributed to the total dose uniformly – the dwell times range from 34.1 to 48.2 s. The dwell times for the interstitial needles were between 2.7 and 25.2 s. Treatment times for superficial and interstitial component of the treatment plan were 84% and 16% of total treatment time, respectively. This was to be expected since the interstitial component of the applicator was used for fine distribution of the dose to the clinical target to allow for adequate coverage. Dosimetry of the CTV and bone is presented in Table 1. It was found that D90 and D95 for the CTV was 100.13% and 95.95%, respectively. V100 for the bone was 0.82% or 0.63 cm3. V150 and V200 for the bone were found to be 0.
Table 1
Dosimetry of the CTV and finger bones
Overall, the patient tolerated the whole treatment course. She required hospitalization one day after insertion of the catheters for pain control with an axillary block. After treatment, she was started on tramadol and gabapentin for long-term pain management. At three-month follow-up, MRI showed a small interval decrease in tumor size with resolution of her pain. In addition, the patient retained functional use of her 3rd and 4th digits. She was able to continue her work as a healthcare professional during this post-treatment period. Her six-month MRI showed an interval decrease in the tumor size as well as a newly developed grade 2 soft tissue necrosis that was treated with hyperbaric oxygen.
Discussion
The standard of care of SCC involving the hand and/or fingers is largely surgery. This is based on literature showing high tumor control rates after surgical excision [16,17,18]. Two of these series cite a recurrence rate as low as 3% [16,17]. Schiavon et al. reported 5-year progression-free survival of 82% [18]. The main reasons for radiation therapy for SCC have been inoperability either due to the patient’s inability to tolerate surgery and/or reconstruction, size and location or lesion, and patient preference. Finally, although long-term cosmesis after surgery, especially with the rise of Mohs micrographic surgery, has improved, radiotherapy often offers superb cosmetic results [8,9,10,11,12,13,14].
The 5-year-control rates for non-melanoma skins cancers of all sites treated with EBRT are good, ranging from 80% to 93% [19]. Brachytherapy provides the distinct advantage of maximizing the dose to the tumor while minimizing delivery of the dose to normal tissue. To individualize treatment parameters for a patient’s tumor, surface molds and/or interstitial catheters are used to position the isotope and deliver precisely targeted radiation.
The majority of the limited literature on brachytherapy for nonmelanoma skin cancer involves HDR surface mold modality [20]. There are only four reports that report interstitial LDR brachytherapy and all involve sites of the face [21,22,23,24]. Radiobiological studies showed that the effectiveness of LDR and HDR protocols was the same without increasing toxicity [25]. There is no literature that we are aware of that reports on interstitial HDR brachytherapy for SCC of the hand.
The primary goal of this treatment was to prevent the growth of the tumor and preserve the function and cosmesis of the patient’s hand. With interstitial and surface HDR brachytherapy, we were able to achieve both objectives albeit with notable side effects. Tumor control assessed by MRI at three and six months showed ~10% decrease in tumor size. Treatment-related side effects acutely were pain and long-term skin necrosis. While the patient did require hospitalization for an axillary block for pain control, this was temporary and her pain returned to baseline within two weeks after treatment. Given the location of the tumor and concern for dorsal, dermal invasion, the dose of the superficial skin was weighed against the potential for skin necrosis. In this patient, grade 2 skin necrosis was observed and treated with hyperbaric oxygen. From this patient’s perspective, the cosmetic result was more than acceptable when weighed against amputation. When planning these cases, the balance between achieving a tumoricidal dose and potential side effects will be an ongoing challenge. Patients should be counseled on potential side effects and the potential for long-term skin necrosis. No complications or tumor progression were noticed at our standard follow-ups at 2 weeks, 8 weeks, six months (Figure 5) and one year. The patient remains under regular surveillance. In summary, the treatment allowed the patient to retain functional use of her hand and produced an acceptable cosmetic outcome while providing tumor control. In selected patients who refuse ray amputation, this treatment paradigm could offer an alternative therapeutic option.

In the future, a prospective study should be conducted to evaluate the longer-term efficacy of tumor control and side effects in a larger set of patients. Also, as more patients are treated with this novel technique, case-matched studies with EBRT and/or surgery should be done.
Conclusions
In this case report we show that combined interstitial and surface HDR brachytherapy is an alternative therapy to ray amputation for a patient with recurrent SCC of the hand. Skin toxicity using this modality was observed but hand function after treatment is excellent. In carefully selected patients, interstitial and surface HDR brachytherapy can be an appropriate and effective option for recurrent SCC of the hand.








