
Introduction
Dermatophytosis is a superficial fungal infection that affects the fully keratinized layers of the skin, nails, and hair [1]. There are three species of dermatophytes: Microsporum, Trichophyton, and Epidermophyton [2]. Approximately 20–25% of the general population is affected [3]. The incubation period typically ranges from 1 to 3 weeks, but in some cases, it can be as short as 4 days [4, 5]. Zoophilic species cause strong inflammatory reactions, which can result in spontaneous recovery. In contrast, anthropophilic species tend to cause milder and more persistent skin lesions. Some researchers have proposed that the transition from sexual to asexual forms of anthropophilic species can lead to unpredictable adaptive responses, resulting in the emergence of different species and variants [6]. It has been suggested that the inflammatory response is linked to dermatophyte infection, and this response is parallel to the delayed-type hypersensitivity skin reaction to these dermatophytes [6]. Moreover, it has been hypothesized that inadequate clinical response is due to the deficient responsiveness of T lymphocytes to certain fungal antigens [6]. Current methods for diagnosing cutaneous fungal infections include direct microscopic examination with potassium hydroxide and fungal cultures. However, these traditional mycological investigations are time-consuming, complicated, and require mycological tools. Dermoscopy is becoming a straightforward, quick, and accessible diagnostic procedure that can be used at the patient’s bedside. The dermoscopic features of dermatophytosis are distinct and include an erythematous background with white peripheral scales with distinctive inward to outward direction, broken hair, Morse code hair, wavy hair, brown dots, and follicular micropustules, mainly at the active border of the lesion [7]. Recently, there has been an upsurge in cases of dermatophytosis with various modes of presentation, which are highly inflammatory and have a chronic recurrent course with unremarkable therapeutic outcomes [8]. Minocycline, a second-generation member of the tetracycline family, is a clinically accessible antibiotic with broad-spectrum activity against both Gram-positive and Gram-negative bacteria. Minocycline is frequently used to treat reproductive tract, respiratory, skin, and suppurative infections [9]. According to recent reports, tetracyclines have a range of biological effects that are distinct from their antimicrobial activity. These effects include anti-inflammatory and anti-apoptotic properties, as well as the prevention of angiogenesis, proteolysis, and tumour metastasis. These results are particularly relevant for minocycline, as it has been discovered to have many biological effects that are not antibiotic-based and are helpful in experimental models of several inflammatory diseases, such as dermatitis, periodontitis, atherosclerosis, and autoimmune conditions [9].
Aim
This study highlights the importance and value of adding minocycline as an adjunctive treatment together with itraconazole for recurrent widespread dermatophytosis. To the best of our knowledge, this is the first study globally.
Material and methods
Study design and setting
This prospective clinical intervention trial was conducted at two private clinics between October 2023 and June 2024. A cohort of 86 patients with recurrent widespread dermatophytoses (involving more than 20% of the body surface area) was enrolled in this study.
Inclusion criteria
All patients with recurrent widespread dermatophytoses, who were between 18 and 65 years of age and were free from any treatment for the last 6 weeks, were included in the study.
Exclusion criteria
Patients with chronic liver and renal diseases, congestive heart failure, or any chronic heart disease; pregnant and lactating women; patients with known allergies to both used drugs; patients with poor compliance; children below 18 years; and patients older than 65 years were excluded from the study.
Data collection
The included patients were interviewed, and detailed history was taken regarding the patient’s age, occupation, any chronic diseases, drug use, duration of the disease, presence of domestic animals, and the previously used drugs with their duration, family history of the same condition, and written consent was obtained for participation in the study.
Clinical evaluation and laboratory confirmation
A full examination of patients with full exposure was performed. During the clinical examination of dermatophyte infections, we examined the appearance of lesions that included red colour and scaly rash with ring-shaped (annular) lesions. Patients experienced itching, scaling, and cracking. Common sites included the feet, groin, scalp, body, and nail. The body surface area involved in the disease was calculated.
Laboratory methods
According to the Indian Association of Dermatologists, Venereologists and Leprologists (IADVL), the diagnosis was based on clinical examination and KOH wet preparation. Dermoscopy has been utilized as an additional tool to confirm the diagnosis [10].
Dermatoscopy and KOH preparation (potassium hydroxide test)
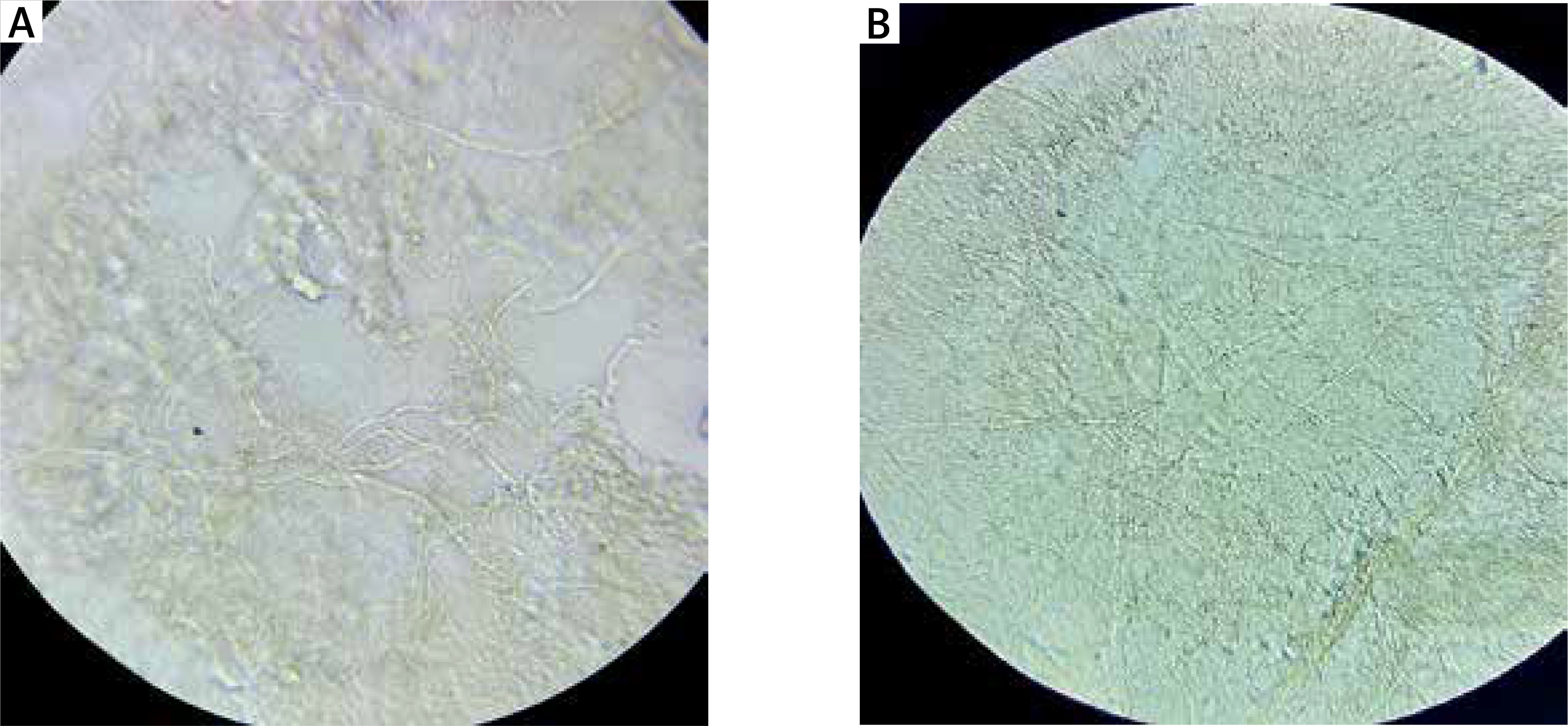
Dermoscopic (DermLite (DL), 4th generation dermatoscope, USA, magnification power: 10, IEC 60601-1-2; 2014) examination with potassium hydroxide (KOH) wet preparation was performed, and clinical photos by digital camera HD (Sony, China) were taken at baseline and then at each visit. Skin scrapings were obtained and placed on slides. Slides (ATACO, China) were then treated with 10% KOH (INNOVATEK, Innovatek Medical Inc., Canada) to dissolve keratin and examined under a compound light microscope (Olympus, Japan). Branching and septate hyphae (dermatophyte infection) were also observed (Figure 1).
Interventional course
All included patients were investigated before treatment and then monthly during the follow-up period until the end of the treatment course in the form of liver and renal function tests, blood count, and relevant serological tests.
All patients received systemic treatment with itraconazole 100 mg/day along with minocycline 80 mg/day for two–six/2–6 weeks without any topical treatment. The patients were strictly followed up every 2 weeks until a complete clinical, dermoscopic, and microbiological cure was obtained, followed up monthly for 3 successive months, and then asked to return if there was any recurrence.
At each visit during the follow-up period, the patients were examined clinically by dermoscopy, followed by KOH wet preparation, and clinical photographs were taken. Patients were asked about any possible side effects and the degree of satisfaction with the treatments being used. Clinical assessments were performed based on the improvement in erythema, scales, and itching. Dermoscopic assessment depended on the complete absence of scales, erythema, brown dots, and pustules as a complete cure. The degree of patient satisfaction was calculated based on this score 2 – fully satisfied; 1 – partially satisfied; and 0 – not satisfied.
Results
This study included 86 patients aged between 18 and 65 years with recurrent dermatophytosis. Among them, 65 (75.6%) were females and the remaining 21 (24.4%) were males, resulting in a female-to-male ratio of 3 : 1 (Table 1).
Table 1
The number and percentage of female and male participants
| Sex | No. | % |
|---|---|---|
| Female | 65 | 75.58 |
| Male | 21 | 24.42 |
| Total | 86 | 100 |
In this study, Trichophyton rubrum was the most common species, accounting for 61 (70.9%) cases, followed by T. mentagrophytes (12, 13.9%). As to other, Microsporum gypseum was observed in 8 patients, M. canis in 4, and Epidermophyton floccosum in 1. All individuals with these infections exhibited scaly and itchy rashes. Annular plaques were noticed in 80 (93%) patients. The groin was the most commonly affected site (13, 15.1%), followed by the scalp and body, and nearly half of the patients (41, 47.6%) had infections at more than one site, suggesting widespread fungal spreading. These findings highlight the predominance of T. rubrum in dermatophytosis cases, with common symptoms and multiple affected body sites, especially in the groin, body, and scalp (Table 2).
Table 2
Characteristics of the lesions and species of dermatophytes that caused the skin lesions in this study
Within 2–6 weeks of treatment, the study found that 100% of patients recovered. After 2 weeks, 36% of the patients had been cured, and by the fourth week, 40.7% of the patients showed full recovery. After 6 weeks, 23.3% of the patients were cured. Following the completion of the treatment course (Table 3).
Table 3
The number and percentage of cured patients over time (cure rate)
| Duration | No. | % |
|---|---|---|
| 2 weeks | 31 | 36 |
| 4 weeks | 35 | 40.7 |
| 6 weeks | 20 | 23.3 |
| Total | 86 | 100 |
Significant reduction in itching has been demonstrated to occur within the first week of treatment. Regarding sex, male patients showed an earlier response and did not experience any recurrence. This difference in response time between males and females was statistically significant, with X 2(2, N = 86) = 7.56, p = 0.023. The effect size was approximately 0.3, which suggests a moderately noticeable association between sex and time of response (Table 4).
Table 4
The response (cure rate) of male and female patients with time
| Duration | Female No. (%) | Male No. (%) | |
|---|---|---|---|
| Early response (2 weeks) | 19 (29.2) | 12 (57.1) | |
| Late response | 4 weeks | 27 (41.5) | 8 (38.1) |
| 6 weeks | 19 (29.2) | 1 (4.8) | |
| Total | 65 (100) | 21 (100) | |
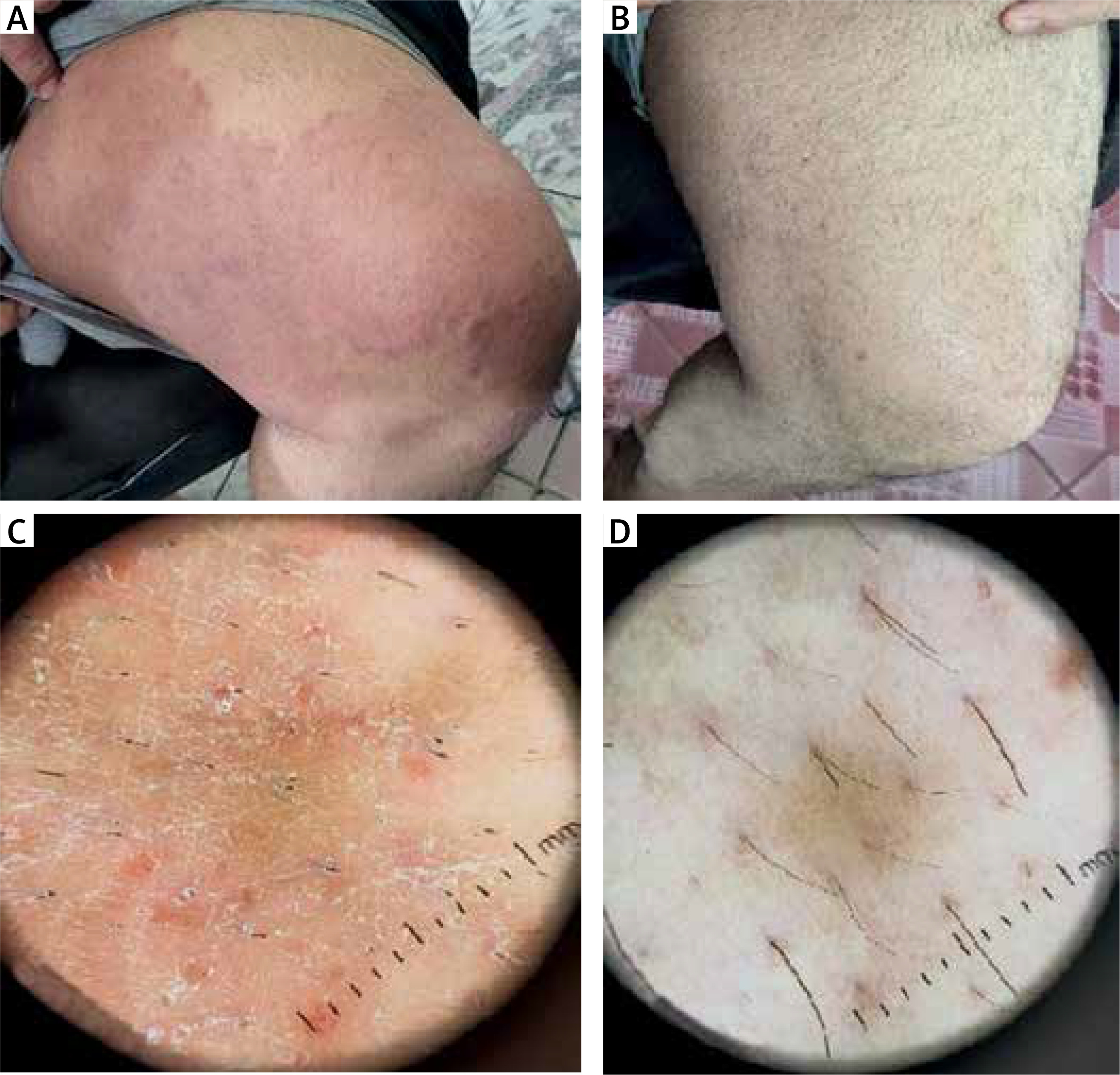
Figures 2–5 A and B display the clinical pictures of 3 different patients before and after treatment. The patients initially presented with erythematous scaly annular plaques with active borders. Complete resolution was observed at various time intervals (2, 4, and 6 weeks of treatment). For these patients, pretreatment dermoscopy showed an active border of scales and brown dots on a background of erythema. After treatment, dermoscopy showed complete clearance of erythema, scales, and brown dots (Figures 2–5 C, D).
Figure 2
A 33-year-old female presented with an erythematous, scaly, annular plaque with an active border on her abdomen and groin. A – At baseline of examination. B – After 2 weeks of treatment, the patient presented with a complete absence of the scales and erythema with only post-inflammatory hyperpigmentation. C – Dermoscopic findings of the same patient before treatment showed an active border of scales and brown dots on a background of erythema. D – After 2 weeks of treatment, the patient presented with complete clearance of erythema, scales, and brown dots
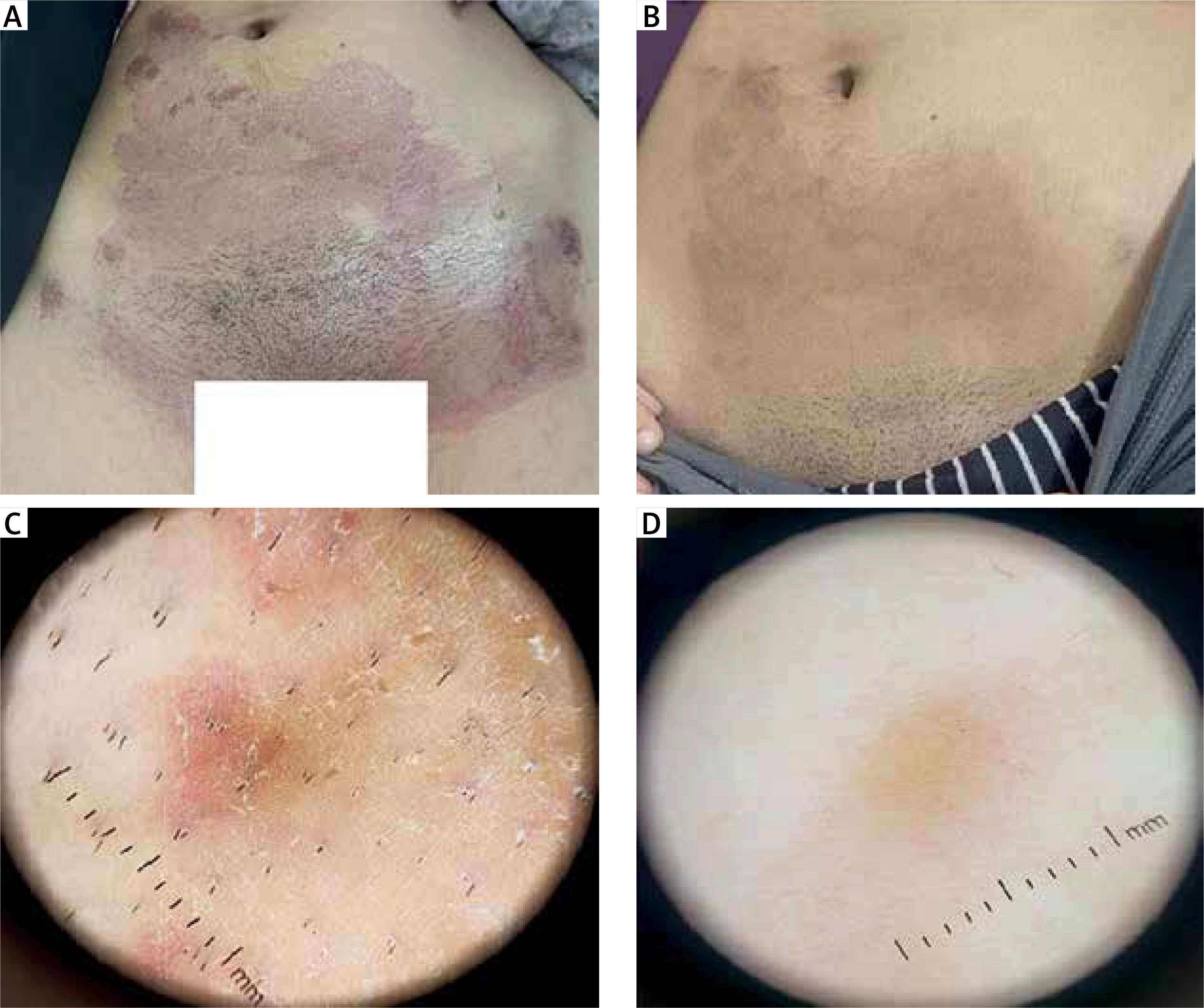
Figure 3
A 21-year-old female presented with an erythematous, scaly, annular plaque with an active border on her lower back. A – At baseline of examination. B – After 2 weeks of treatment, the patient presented with a complete absence of the scales and erythema with only post-inflammatory hyperpigmentation. C – Dermoscopic findings of the same patient before treatment showed an active border of scales and brown dots on a background of erythema. D – After 2 weeks of treatment, the patient presented with complete clearance of erythema, scales, and brown dots
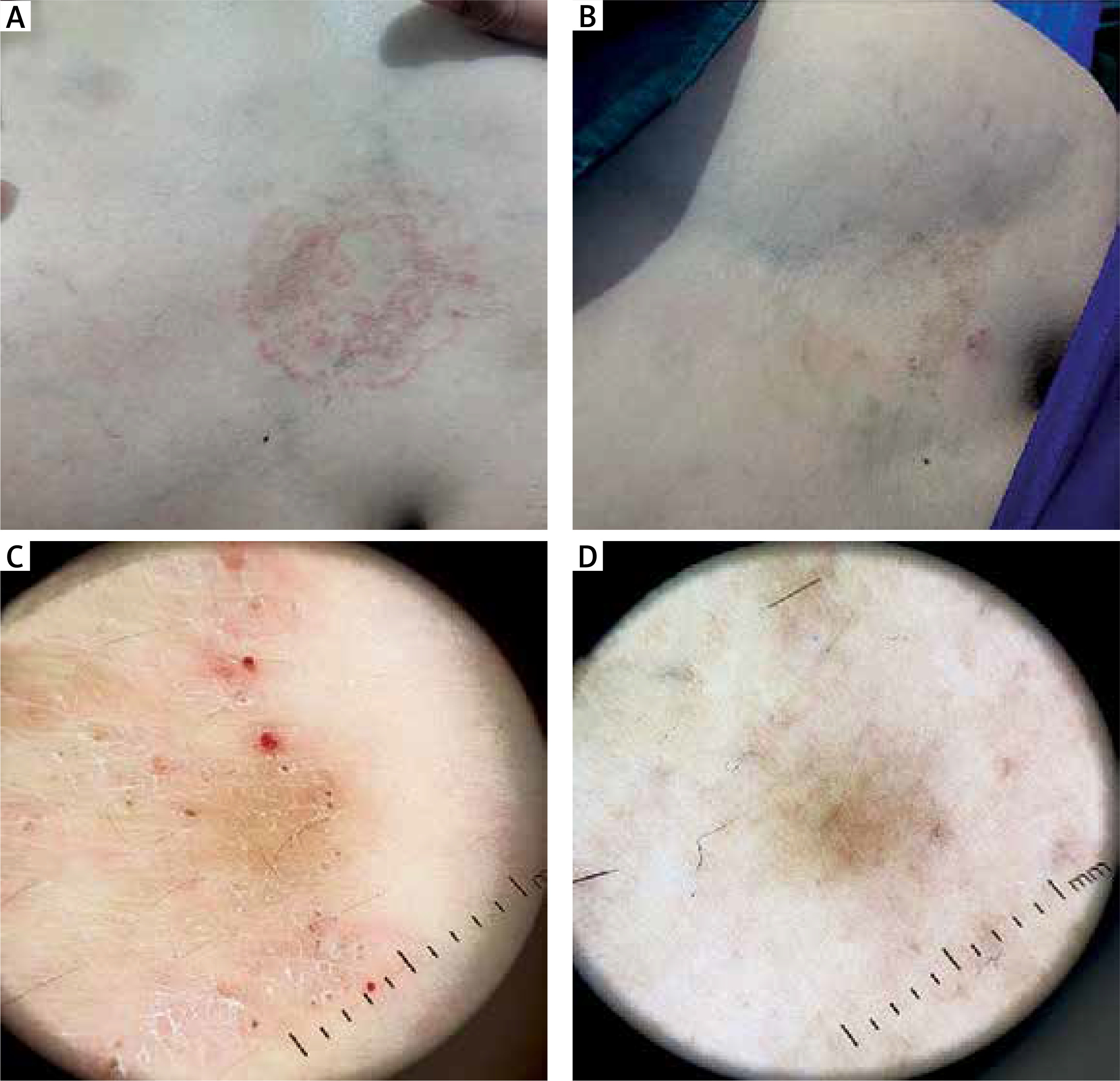
Figure 4
A 25-year-old female presented with an erythematous, scaly, annular plaque with an active border on the inner aspect of her right forearm. A – At baseline of examination. B – After 4 weeks of treatment, the patient presented with a complete absence of the scales and erythema with only post-inflammatory hyperpigmentation. C – Dermoscopic findings of the same patient before treatment showed an active border of scales and brown dots on a background of erythema. D – After 4 weeks of treatment, the patient presented with complete clearance of erythema, scales, and brown dots
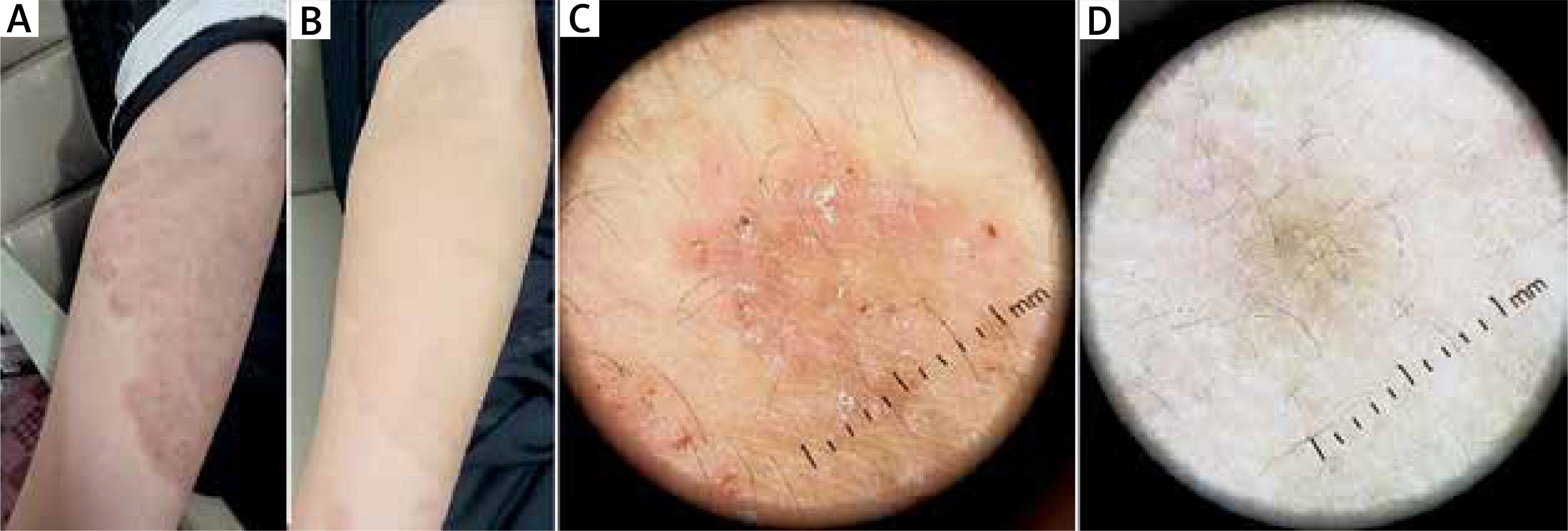
Figure 5
A 62-year-old male presented with an erythematous, scaly, annular plaque with an active border on the inner aspect of his left thigh. A – At baseline of examination. B – After 4 weeks of treatment, the patient presented with a complete absence of the scales and erythema. C – Dermoscopic findings of the same patient before treatment showed an active border of scales and brown dots on a background of erythema. D – After 4 weeks of treatment, the patient presented with complete clearance of erythema, scales, and brown dots
On the other hand, a relapse rate among patients with a complete cure was reported in 3 (3.5%) patients during the follow-up period, and all of them were females. Regarding side effects, dizziness and mild gastric discomfort were reported in 2 (2.3%) patients. Most of the treated patients were fully satisfied with the results (93.1%), while the remaining 3 (6.9%) patients were partially satisfied (Table 5).
Discussion
It is believed that a mix of environmental, host, fungal, and pharmacological factors are responsible for the novel dermatophytosis presentation and recurrence modalities that have become more prevalent in recent years [11]. Recurrent, inflammatory chronic dermatophytes are becoming more common in daily clinical practice in our area because of several factors, including the hot, humid, and long summer, the possibility of new species with high virulence and inflammatory characteristics, and the growing popularity of domestic animals, especially cats, where hyphae typically live in the hair without routine veterinary examination. Additionally, the predominance of T helper 2 response, defect in the macrophage killing mechanism, decrease in anti-inflammatory cytokines (such as interleukin-10 (IL-10)), and increase in inflammatory cytokines (such as IL-1β, IL-6, IL-8, and tumor necrosis factor-α (TNF-α)), with low levels of free radicals in 20–30% of the patients, appear to be the causes of these problematic chronic cases [12–14]. Moreover, the increasing occurrence of chronic dermatophytosis in adults, especially females, may be primarily attributed to variations in sebum production and alterations in the immune response [11]. There are two types of dermatophyte resistance to systemic and topical antifungal drugs: primary, where the pathogenic species are resistant even in the absence of previous drug treatment; and secondary, where gene expression alterations are the cause [15, 16]. Although a wide range of therapeutic techniques such as use of ND-YAG lasers or isotretinoin alone or in combination with anti-fungals- the success rates of these treatments are inconsistent, both alone and in combination with antifungals such as ND-YAG lasers or isotretinoin, have been attempted, the success rates of these treatments are inconsistent [17, 18]. These data strongly suggest the necessity for a novel medicine with anti-inflammatory and antimicrobial properties. Minocycline has been shown to have synergistic effects with antifungal agents in vitro as well as anti-inflammatory effects by reducing matrix metalloproteinase activity, leukocyte chemotaxis, and production of inflammatory cytokines (TNF-α and IL-1β) [19, 20]. The study revealed that most of our patients were adult females, accounting for 65 (47.7%) individuals. The combination of minocycline and itraconazole resulted in a 100% cure rate in all cases. Additionally, 31 (36%) of the treated patients experienced early recovery within 2 weeks, and the majority were male. Moreover, a substantial reduction in itching and other indicators of inflammation was observed quickly after initiating the therapy. In addition, the relapse rate among patients who received treatment was 3.5% during the treatment and follow-up periods. Those who relapsed either refused to treat and isolate their domestic animals or their compliance was inadequate.
In terms of side effects, 2 patients reported slight gastrointestinal discomfort and dizziness, which did not require treatment discontinuation or the addition of symptomatic drugs. In 93% of cases, the patients were extremely satisfied with the therapy. The distinguishing early and complete clinical, microscopic, and dermoscopic cure rates are mostly due to the anti-inflammatory actions of minocycline and its synergistic anti-fungal properties. In a previous case report, Flowers et al. demonstrated that a patient with a resistant fungal infection responded very well to oral therapy that combined minocycline and itraconazole [21]. To our knowledge, this is the first trial to assess the use of a combination of minocycline and itraconazole for the treatment of recurrent widespread dermatophytoses.
The limitations of our study are a relatively small sample size and the fact that the study was a prospective clinical therapeutic trial and not a randomized case-control study. Further randomized case-control studies with larger sample sizes are needed to confirm these findings. Future studies should be conducted to determine the efficacy of ultraviolet light examination (Wood’s lamp), histopathology (skin biopsy), and molecular testing (PCR). Several recommendations can be made to improve understanding and management of recurrent dermatophytosis. Future research should include a larger, multicentre, and more diverse sample population. A longer follow-up period was used to assess the long-term recurrence rates. Investigating etiological factors such as comorbidities, hygiene practices, and environmental influences should be considered. Advanced diagnostic techniques, such as histopathology and PCR, are used to better identify dermatophyte species.
Conclusions
This study highlights Trichophyton rubrum as the predominant causative agent of recurrent dermatophytosis, with a significant prevalence among the affected population, particularly females. The typical clinical presentation includes scaly and itchy rashes and annular plaques, with the groin being the most commonly affected site. A considerable proportion of patients experience infections at multiple sites in the body. The concurrent administration of minocycline and itraconazole resulted in a rapid and thorough cure, as demonstrated by clinical observations, as well as microscopic and dermoscopic examinations. Male patients responded relatively faster than female patients did, with a lower recurrence rate. The effectiveness of this therapeutic strategy was demonstrated within a short time period, with a low risk of recurrence and without any noticeable adverse effects.







