
Introduction
The prevalence of hepatitis C virus (HCV) antibodies worldwide ranges from 1.6% to 2.8%. The peak prevalence is reported in low-income countries, including Egypt (15%) and Pakistan (4.7%), and is lower in North America (range: 1.1-1.3%), Australia (1.7%), and Eastern and Western Europe (range: 0.5-4.5%) [1, 2].
The latest epidemiologic reports suggest that there are currently 80 million HCV-RNA-positive individuals around the globe [1, 3].
As a result of receiving frequent blood and blood product transfusions and/or intravenous drug therapy, child patients with malignancy are potentially at a higher risk of HCV infection, which is diagnosed in 1.5% to 32% of patients around the world, depending on the geographic area and type of malignant disease studied [4-6].
In up to 5% of neonates born to infected mothers, vertical transmission may occur, influenced by the immunogenetic profile of both mother and child, mother’s viral load and human immunodeficiency virus (HIV) status. Type of transmission also differs within the pediatric population and HCV infection decreases the general health and quality of life in adolescents despite high rates of asymptomatic infection in children [5].
Chronic HCV infection was shown to be associated with hepatocellular carcinoma (80% of cases are preceded by hepatitis B or C infection) and non-Hodgkin lymphoma (NHL; HCV infection increased the risk of developing NHL by 20-30%) with significant increase of morbidity and mortality, while immunosuppression from cancer-related treatment and/or cancer itself could increase the risk of chronicity, activation and progression to cirrhosis in patients with chronic HCV [6-8].
Because of a higher rate of progression to fibrosis, rapid development of cirrhosis, worse outcome, and increased viral titers are more common in patients with hematologic malignancies than in patients without cancer; therefore management of HCV infection in these cases is more demanding [9, 10].
In 2013 direct-acting antiviral (DAA) regimens were approved in adults and they showed an excellent response rate of more than 95% with minimal side effects for 12 weeks. In the following years this regimen was applied in adolescents aged 12-18 years (2017), in school-aged children 6-11 years, and recently, the FDA approved the sofosbuvir/ledipasvir (SOF/LDV) combination for children aged 3 years with genotypes 1 and 4 [11-13].
For these reasons the beneficial effects of DAA treatment and subsequent sustained virologic response (SVR) in patients with malignancy and chronic HCV infection can improve patients’ hepatic and extrahepatic consequences; this confers manifold potential benefits [14, 15].
Around the world, HCV infection is encountered in 1.5% to 32% of patients with malignancy, depending on the type of malignancy studied and geographic area [6, 16, 17].
Previously, the treatment of chronic HCV infection has been neglected in oncology centers, perhaps due to fear of treating patients receiving chemotherapy and older HCV therapy, such as interferon, but the treatment protocols with DAAs have changed the treatment criterion and dramatically improved SVR, which is now similar in HCV-infected patients with and without malignancy [18, 19].
Material and methods
A prospective cohort study in a single tertiary hospital was conducted on pediatric patients with malignancy infected with HCV from January 2018 to October 2020. We recruited them in the outpatient pediatric hepatology and gastroenterology clinic at a children’s welfare teaching hospital/medical city complex. The study was conducted in a single tertiary hospital on 30 patient with malignant diseases, and simultaneously who are suffering from HCV but did not receive any specific treatment for the this infection. Their age (at the time of diagnosis of HCV) ranged between 3.2 and 15.3 years; the mean age was 8.3 years, with male predominance of 60%. Inclusion criteria were children with malignancy aged between 3 and 16 years, with HCV RNA analysis by polymerase chain reaction (PCR) results of more than 1000 IU/l [20]. Exclusion criteria were children older than 16 or younger than 3 years, viral load less than 1000 IU/l, patients with associated comorbidities of hepatitis B virus or HIV infection, autoimmune hepatitis, any biliary disorder, Wilson’s disease, hemolytic anemia, or any critical illness, critically ill children, any patients with hepatocellular carcinoma or metastases to the liver to avoid the confounding effect on liver biochemical tests caused by tumors infiltrate, or parents’ refusal for participation of their children in the study or for signing the consent form.
Six patients were excluded from the study: two patients with viral load lower than 1000 IU/l, one patient had concomitant hepatitis B virus (HBV) infection and in the case of three patients their parents refused to include them in the study.
All patients submitted to laboratory assessment initially and subsequently at weeks 4, 8 and 12 and at 12 weeks after the end of treatment: sustained virologic response 12 (SVR12).
Parents were instructed to immediately contact their responsible doctor if any serious side effects or other worrisome condition developed at any time during the treatment course.
Written consent was obtained from all participants. Moreover, the study was approved by the Ethical Scientific Committee of the Children’s Welfare Teaching Hospital and was carried out according to the guidelines of the Helsinki Declaration [21].
All patients received treatment for 12 weeks which consisted of weight-based doses of SOF/LDV fixed-dose combination granules (33.75 mg/150 mg if their weight was < 17 kg or 45 mg/200 mg if their weight was in the range 17-35 kg and 90 mg/400 mg if their weight was > 35 kg) once daily.
Statistical analysis
SPSS version 23 was used to tabulate data, one-way ANOVA was used to evaluate the association between different variables means, quantitative values were expressed as means ± standard deviations. Qualitative data were expressed as proportions and percentages (with upper and lower confidence limits) and a p-value of less than 0.05 was considered significant.
Results
Thirty eligible patients all of whom fulfilled the in-clusion criteria of the study were included and all received treatment with SOF/LDV which consisted of weight-based doses. All the patients were followed during the whole period of the treatment (every 4 weeks) and 12 weeks after the end of treatment all achieved treatment response (SVR12).
The age ranged from 3.2 to 15.3 years; the mean age was 8.3 years, with male predominance of 60%.
Twenty-one were treated for acute lymphoblastic leukemia (ALL), four for Hodgkin’s lymphoma, two for acute myeloblastic leukemia (AML), and one each for neuroblastoma, osteosarcoma, and Wilms’ tumor.
The commonest HCV genotype in the study group was genotype 4 in sixteen patients (53.3%), followed by genotype 1 in twelve patients (40%), and two patients with genotype 2 (6.7%). Hepatitis screen was positive in 25 patients (83.3%) as shown in Table 1.
Table 1
Clinical and demographic characteristics of the studied group
Routine laboratory investigations were performed at baseline (prior to treatment) and followed serially at 4, 8, 12 weeks and 12 weeks after finishing treatment, as summarized in Table 2. The hemoglobin (Hb) level, white blood cell (WBC) count and platelet count did not show significant changes after treatment, international normalized ratio (INR) showed slight decrease after treatment, initial alanine amino transferase (ALT) and aspartate aminotransferase (AST) were approximately 4-5 times above the upper limit of normal (ULN) in about two third of patients, but there was a gradual significant decline in the subsequent reading until normalization at the end of treatment.
Table 2
Biochemical profile at baseline, after 4, 8, 12 weeks and 12 weeks after completing treatment in the 30 hepatitis C virus-infected children and adolescents
Serum bilirubin level showed a gradual decrease from 1.84 ±1.33 (±0.243) to the normal level of 0.69 ±0.31 (±0.057) after the end of the treatment.
Regarding serum albumin and serum creatinine both showed gradual normalization until the end of treatment.
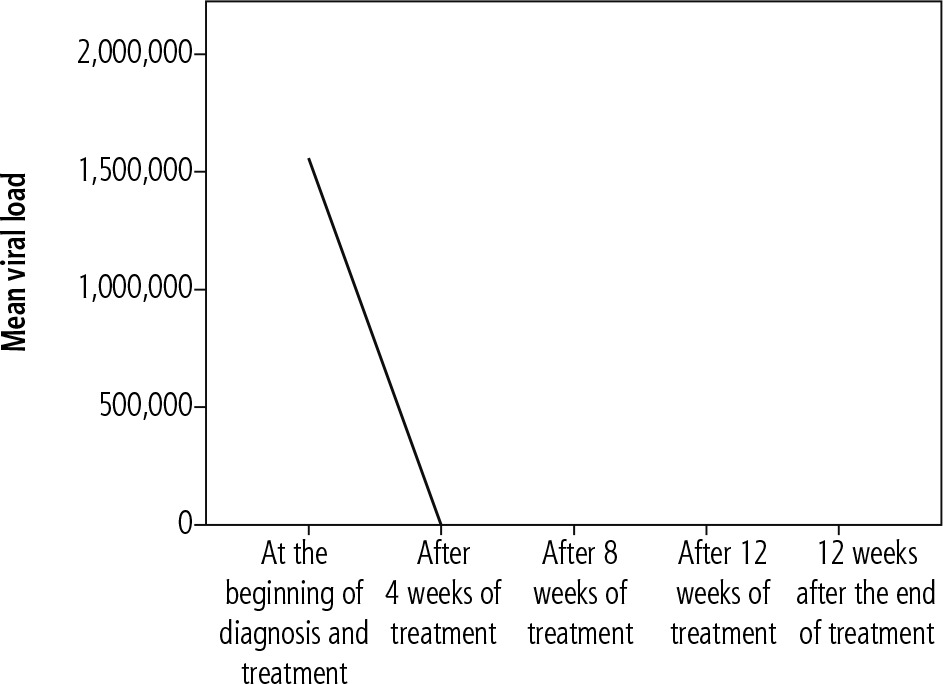
After 4 weeks of treatment, all patients had negative HCV RNA, and maintained it at week 8 and at the end of treatment (week 12). All patients (100%) achieved SVR12 as shown in Figure 1.
Treatment was well tolerated by all patients without any serious side effects or treatment discontinuation. The most common side effect observed in the study group was tiredness, reported by 10 patients (33.3%) during the course of treatment, followed by nausea and diarrhea in 8 cases (26.6%), headache in 6 patients (20%), two patients suffered from sleep disorders (6.66%), but 12 patient (40%) did not report any side effects. No patient experienced serious or dangerous adverse reaction or discontinued treatment because of the side effects, as shown in Table 3.
Table 3
Side effects encountered in the studied sample
| Side effects | n | % |
|---|---|---|
| Tiredness | 10 | 33.30 |
| Nausea | 8 | 26.66 |
| Diarrhea | 8 | 26.66 |
| Headache | 6 | 20.00 |
| Difficulty in sleeping | 2 | 6.66 |
| None | 12 | 40.00 |
The HCV PCR showed a very rapid virologic response to an undetected level at the fourth week of treatment and maintained SVR at post-treatment week 12 as shown in Figure 1.
Discussion and conclusion
To our best knowledge this is the first study conducted to test the effects of dual SOF/LDV therapy on children and adolescents infected with chronic HCV who at the same time suffered from malignant disease in Iraq.
Treatment of HCV infection is more difficult in patients with malignancies than in patients without because of a higher rate of worse outcome, increased viral titers, progression of fibrosis, and more rapid development of cirrhosis [14, 15, 18].
In this study, children (n = 30), aged 3-16 years, received a single daily dose of dual SOF/LDV combination regimen.
The overall response was 100% in all patients and no serious adverse effects were observed.
Although the treatment of children older than 3 years with the interferon/ribavirin-based therapy is controversial because of associated significant side effects as well as the non-favorable response to the treatment in genotypes 1 and 4, as well as the approval of the dual SOF/LDV in children, specifically those who are suffering from malignant disease, it is encouraging because of increased access to malignant disease treatment, improved malignant disease treatment outcomes, prevention of HCV reactivation during its treatment, reduced liver disease progression rate, and increased access to liver transplantation and hematopoietic cell transplantation [22].
The commonest HCV genotype found in this study was type 4 (53.3%) followed by type 1 in 40%, and type 2 in one patient (6.7%); these findings are consistent with previous result obtained in Iraq [23-25].
Although the patients presented as HCV-PCR positive with a mean titer of 1.447.487 IU/l, about 6.7% of them had negative primary hepatitis C antibody, and for this reason it is not appropriate for accurate diagnosis to rely solely on presence or absence of antibody only against hepatitis C [26, 27].
Regarding the distribution of malignant disease in the study cohort acute lymphoblastic leukemia is the commonest disease in 70% of cases, followed by lymphoma and acute myeloblastic leukemia.
The initial reading of liver enzymes (ALT) after the diagnosis of HCV was found elevated in 76.3% of our patients with a mean value of ALT 230 U/l (about 4 times the upper limit of normal), and this is comparable to Locasciulli et al. [28] and Economides et al. [29]. Our result, however, is almost twice that reported by others, in addition to a slow return to normal value. This may be explained by a selection bias given that others recruited their patients from a pediatric hepatology clinic with HCV infection after management of malignancy and after cessation of oncologic therapy whereas we selected our patients who were still continuing their treatment with chemotherapy and without abatement of the immunosuppressive effects.
Anyhow, even in patients with advanced liver cirrhosis, their liver function tests have been shown to recover when HCV replication is successfully omitted [30].
We found that the concomitant use of dual SOF/LDV in patients with malignant diseases was well tolerated in this age group. The most common adverse events were tiredness, nausea, diarrhea, headache, and difficulty in sleeping and no patients experienced serious adverse events, discontinuation of treatment, laboratory abnormalities or death.
The limitations of this study were the small sample size, FibroScan was not available for all patients, we were not able to accurately assess the cirrhotic and fibrotic stage in some patients, costs of some investigations and drug purchasing for many patients, and the short duration of follow-up, as it would be informative to evaluate outcomes in patients over longer periods following viral clearance.
In conclusion, SOF/LDV is a safe and effective drug in children infected with chronic HCV aged older than 3 years with malignant disease who are still receiving their specific chemotherapy. Nonspecific trivial development of a few side effects may occur in some patients, but no serious adverse reactions were reported.





