
Summary
Despite the growing number of studies on the epidemiology of out-of-hospital cardiac arrest (OHCA) in Poland, this issue has not been sufficiently studied to date. Moreover, most previous studies on the epidemiology and management of OHCA in Poland were limited by retrospective character, low adherence to the guidelines for uniform OHCA data reporting, and lack of data on in-hospital management and outcomes of OHCA. Our study aimed to evaluate the epidemiology of OHCA, baseline characteristics of OHCA patients, the role of laypeople, and emergency medical service (EMS) in response to OHCA, treatment of OHCA, including coronary revascularization, as well as prehospital and in-hospital outcomes, based on a large, 12-month, prospective registry encompassing the population of 2.7 million inhabitants of Upper Silesia, Poland (Silesian Registry of Out-of-Hospital Cardiac Arrests; ClinicalTrials.gov Identifier: NCT03654859). We found that the prehospital and in-hospital survival rates of patients after OHCA in Poland are low. Only one-fourth of EMS-treated patients after OHCA are admitted to the hospital after ROSC, and less than 30% of hospitalized patients are alive at hospital discharge. In addition, we identified that there is still room for improvement in increasing the prevalence of CPR performed by bystanders and automated external defibrillator use before EMS arrival. To the best of our knowledge, it is also the first paper presenting the outcomes of the specific subgroup of patients with bystander witnessed events and initial shockable rhythm in Poland (the so-called Utstein-comparator group). The Utstein-comparator group constitutes a relatively homogeneous group of OHCA patients, enabling the comparison of various EMS systems’ efficacy between countries.
Introduction
In spite of the considerable advances in cardiovascular and emergency medicine within the last several years, out-of-hospital cardiac arrest (OHCA) is still associated with a very poor prognosis. The modifiable factors having the most significant influence on the survival of patients with OHCA have remained the same, i.e., early recognition of cardiac arrest, timely performed cardiopulmonary resuscitation (CPR), rapid defibrillation, and proper post-resuscitation care [1].
In recent years the number of studies on the epidemiology of OHCA in Poland has multiplied [2–7]. These studies have yielded a large amount of information on the incidence rate of OHCA and prehospital outcomes in the Polish population. However, the data on the frequency of key components of the emergency medical service (EMS) and bystanders’ response to OHCA in Poland have not been sufficiently studied. Moreover, the outcomes of the homogeneous subgroup of patients with bystander witnessed cardiac arrest and initial shockable rhythm (the Utstein comparator group), as a measure of EMS system efficacy, are not well known in the Polish population.
Aim
Our study aimed to evaluate the epidemiology of OHCA, baseline clinical characteristics of OHCA patients, the laypeople, and EMS response to OHCA as well as prehospital and in-hospital outcomes, based on a large, 12-month, prospective registry encompassing a population of 2.7 million inhabitants of southern Poland.
Material and methods
SIL-OHCA registry
We analyzed the data of patients included in the prospective, population-based registry of OHCA (Silesian Registry of Out-of-Hospital Cardiac Arrests; SIL-OHCA; ClinicalTrials.gov Identifier: NCT03654859). The study design and other details on SIL-OHCA have been presented previously [8, 9]. In brief, SIL-OHCA was conducted between the 1st of January 2018 and the 31st of December 2018. The area covered by the registry is a part of Upper Silesia, Poland, which encompasses the region of Voivodeship Rescue Service in Katowice, the largest public EMS provider in Poland. Upper Silesia is a highly urbanized part of Poland, and the area covered by the registry comprises 1.2% of the area of Poland and is inhabited by 7% of the Polish population.
All cases of OHCA within the covered area with CPR started or continued by EMS, and patients with confirmed OHCA and return of spontaneous circulation (ROSC) achieved before EMS arrival, have been included in the registry. In addition, between the 1st of July 2018 and the 31st of December 2018, cases without CPR attempted by EMS were included as well, and the reason for withholding CPR was recorded. Moreover, between the 1st of July 2018 and 31st of December 2018, detailed data on medical dispatch, automated external defibrillator use by laymen bystanders, and information on the functional status of patients before the arrest were collected. The paper-based case report forms, the template of which has been published previously, were filled out by the EMS team, who managed the patients [8]. Completed forms were subsequently digitalized and checked for duplicates and logical errors. The scope of collected data and definitions were based on Utstein guidelines updated in 2014 [9, 10].
In-hospital data
Data on duration of hospital stay, comorbidities, performed procedures, and in-hospital mortality were gathered retrospectively for patients who survived to hospital admission. These data were derived from the National Health Fund (NHF), the sole public payer of health care services in Poland. The anonymized dataset from NHF was merged with data collected in the SIL-OHCA registry based on sex, age, and date of admission to the hospital for OHCA. If a given patient had been transferred between hospitals, the date of discharge from the hospital was considered the last day of the last hospitalization. Information on the past medical history was based on the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes reported to the NHF after all ambulatory visits to a general practitioner, outpatients specialist care, or hospitalizations between 2006 and 2019, except for mental, behavioral and neurodevelopmental disorders codes (ICD-10: codes F00-F99). Information on medical procedures performed at the time of index hospitalization or between 2006 and admission for OHCA was based on an International Classification System for Surgical, Diagnostic, and Therapeutic Procedures (ICD-9-CM) codes.
Patients
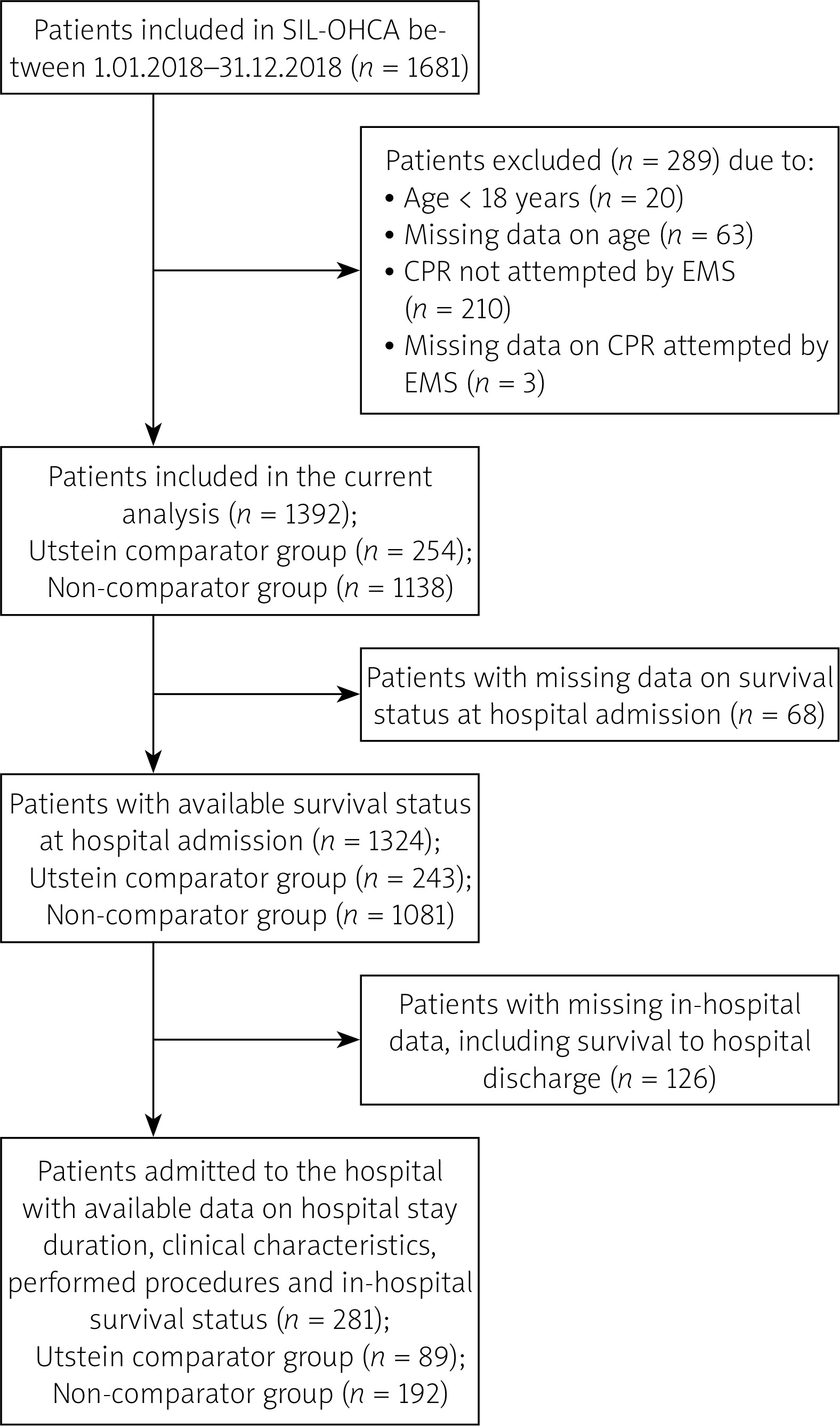
Patients aged 18 or older with CPR started or continued by EMS were included in the current analysis. Patients with missing age (n = 63) or information on whether the CPR was attempted by EMS (n = 3) were excluded. The analysis was performed for the whole cohort and the subgroups of patients with bystander CPR and initial shockable rhythm (i.e., the Utstein comparator group, which enables reliable comparison of different EMS systems’ efficacy) and subjects who did not meet Utstein comparator group criteria (non-comparator group) [10]. The flowchart of the study cohort is depicted in Figure 1.
The study conformed to the Declaration of Helsinki. The Bioethics Committee of the Medical University of Silesia in Katowice waived ethical approval for this study, given the study’s observational nature.
Statistical analysis
Dichotomous variables are presented as percentages. As assessed by the Shapiro-Wilk test, continuous variables were not distributed normally and are, accordingly, presented as a median (interquartile range). Cumulative survival to discharge was calculated by multiplying the probability of survival to hospital admission and the probability of in-hospital survival. The differences between the Utstein-comparator and non-comparator groups in terms of categorical and continuous variables were compared using the χ2 test and the Mann-Whitney U test, respectively. Univariate and multivariable logistic regression models were developed on a subset of patients with available pre-hospital and in-hospital survival status data to identify factors associated with survival to discharge. Covariates significantly associated with survival in univariate analysis entered the multivariable model. The final logistic regression model was created using a stepwise selection of predictors to find factors independently related to survival. A p-value of < 0.05 was considered significant.
Results
Of the 1681 patients included in the registry, CPR was attempted or continued by EMS in 1471 cases of OHCA (54.5 cases per 100,000 population per year). Two hundred and ten patients (15.6 per 100,000 population per year) with CPR withheld or withdrawn by EMS were excluded. The most common reason for withholding or withdrawing CPR was the presence of evident signs of death (81.4%); in 4 cases, ROSC was achieved before EMS arrival (2.4%). Moreover, twenty patients were excluded from further analysis due to age < 18 years (0.7 cases per 100,000 population per year). Finally, 1392 adult patients with CPR attempted or continued by EMS were included in the study.
Among patients included in the current analysis, the median age was 67.2 (57.7–78.0) years, and 66.2% were male. The vast majority of OHCA occurred at home (74.7%) and were of medical etiology (85.5%). In 66.8% of all OHCA cases, laymen bystanders witnessed the collapse, and EMS teams witnessed another 20.4% of cardiac arrest events. Of the non-EMS-witnessed cases, the dispatcher identified cardiac arrest in 63.2% and provided CPR instructions over the phone to laymen bystanders in 54.6%. Bystanders undertook CPR in 54.4% of events, and almost one-fourth of victims received both chest compressions and ventilation. Publicly available AEDs were used in 4.6% of patients who received CPR performed by laymen. Twenty-three percent of patients had shockable rhythm as the first recorded rhythm.
Utstein comparator group criteria (bystander witnessed events and initial shockable rhythm) were met by 254 (18.2%) patients. Patients included in the Utstein comparator group were younger and more frequently male than other patients. Moreover, in this group, more cardiac arrests occurred in locations other than the home and more often were of medical etiology than in the non-comparator group. There were no significant differences between groups regarding bystander CPR and the cardiac arrest identification by the dispatcher. Data on other baseline characteristics are shown in Table I.
Table I
Baseline characteristics of the study population as well as the bystander and dispatcher response in the entire cohort and the subgroups of patients who met and did not meet Utstein comparator group criteria (bystander witnessed CA with an initial shockable rhythm)
| Variable | All patients N = 1392 | Utstein comparator group n = 254 | Non-comparator group n = 1138 | P-value |
|---|---|---|---|---|
| Emergency Medical Dispatch: | ||||
| Dispatcher identified presence of cardiac arresta,b | 63.2% | 69.1% | 61.5% | 0.18 |
| Dispatcher provided CPR instructionsa,b | 54.6% | 56.4% | 54.1% | 0.68 |
| Patient demographics, pathogenesis, initial presentation, and bystander response: | ||||
| Age [years] | 67.2 (57.7–78.0) | 64.0 (56.7–73.0) | 68.0 (57.9–78.9) | < 0.001 |
| Sex (male) | 66.2% | 77.4% | 63.7% | < 0.001 |
| Pathogenesis: | < 0.001 | |||
| Medical | 85.5% | 95.6% | 83.1% | |
| Asphyxia | 6.5% | 1.6% | 7.6% | |
| Traumatic | 2.8% | 1.2% | 3.2% | |
| Other | 5.3% | 1.6% | 6.1% | |
| Witnessed arrest: | < 0.001 | |||
| Bystander witnessed | 66.8% | 100.00% | 59.29% | |
| EMS witnessed | 20.4% | 0 | 25.00% | |
| Unwitnessed | 12.8% | 0 | 15.71% | |
| Bystander CPRb | 54.4% | 51.4% | 55.3% | 0.28 |
| Bystander CPR (actions)b: | 0.12 | |||
| Compressions only | 76.8% | 71.0% | 79.0% | |
| Compressions and ventilations | 23.2% | 29.0% | 21.0% | |
| Bystander AED useb | 4.6% | 0.0% | 6.1% | 0.18 |
| Arrest location: | < 0.001 | |||
| Home | 74.7% | 63.0% | 77.3% | |
| Street | 6.3% | 8.4% | 5.8% | |
| Workplace | 2.7% | 4.4% | 2.4% | |
| Public space/public building | 9.6% | 19.9% | 7.3% | |
| Other | 6.6% | 4.4% | 7.1% | |
| First monitored rhythm: | < 0.001 | |||
| VF | 23.1% | 95.3% | 5.9% | |
| Pulseless VT | 1.5% | 4.7% | 0.8% | |
| Asystole | 56.3% | 0 | 69.6% | |
| PEA | 18.7% | 0 | 23.1% | |
| Bradycardia | 0.5% | 0 | 0.6% | |
| Medical history and comorbidities: | ||||
| Chest pain before OHCA | 15.0% | 19.8% | 13.9% | 0.02 |
| Chest pain duration before OHCA: | 0.02 | |||
| < 1 h | 38.8% | 35.6% | 39.9% | |
| 1–24 h | 26.8% | 15.6% | 30.4% | |
| > 24 h | 15.8% | 20.0% | 14.5% | |
| Unknown | 18.6% | 28.9% | 15.2% | |
| Previous MI | 16.8% | 25.4% | 14.9% | < 0.001 |
| CAD | 25.3% | 26.3% | 25.0% | 0.70 |
| ICD/CRT-D | 1.7% | 1.2% | 1.9% | 0.46 |
| Previous stroke | 10.1% | 5.5% | 11.1% | 0.01 |
| Malignant neoplasm | 8.5% | 4.2% | 9.4% | 0.01 |
| Independent livinga | 79.8% | 93.9% | 76.6% | < 0.001 |
b Refers to non-EMS-witnessed events. AED – automated external defibrillator, CA – cardiac arrest, CAD – coronary artery disease, CPR – cardiopulmonary resuscitation, CRT-D – cardiac resynchronization therapy defibrillator, EMS – emergency medical service, ICD – implantable cardiac defibrillator, MI – myocardial infarction, OHCA – out-of-hospital cardiac arrest, PEA – pulseless electrical activity, VF – ventricular fibrillation, VT – ventricular tachycardia.
Median ambulance response time (time from call to arrival of an ambulance) was 8 (6–11) min, and the median time to the first defibrillation was 4 min longer. Physician-staffed ambulances accounted for 44.3% of all EMS teams. Mechanical CPR (using a LUCAS chest compression device) was performed in 11.1% and endotracheal intubation in 64.5% of patients. ECG e-transmission was performed after ROSC in 35.5% of patients, and ST-segment elevation was preset on 27.4% of 12-lead ECGs.
Both the response time and the time to the first defibrillation were shorter in the Utstein comparator group. Physician-staffed ambulances were more often dispatched to these patients. There were no differences in the frequency of mechanical CPR and endotracheal intubation. ECG e-transmission and ST-segment elevation were significantly more prevalent in patients with a witnessed event and initial shockable rhythm.
Data on ROSC were available for 1367 patients. ROSC was achieved in 36.3% of all analyzed patients and was significantly higher in patients who met the Utstein comparator group criteria than in the non-comparator group (53.4% vs. 32.4%). Finally, 30.7% of all patients were transported to the hospital, including 47.0% of patients with bystander witnessed events and initial shockable rhythm, and 25.1% of patients in the non-comparator group (Table II).
Table II
Emergency medical service response, prehospital treatment, and outcomes of all patients and those who met and did not meet the inclusion criteria of the Utstein comparator group (bystander witnessed CA with an initial shockable rhythm)
| Variable | All patients n = 1392 | Utstein comparator group n = 254 | Non-comparator group n = 1138 | P-value |
|---|---|---|---|---|
| EMS response and treatment: | ||||
| Response time [min]a | 8 (6–11) | 7 (5–10) | 8 (6–11) | < 0.001 |
| Physician-staffed EMS | 44.3% | 50.6% | 42.9% | 0.03 |
| Defibrillation time [min]a | 12 (8–21) | 10 (6.5–15) | 22 (11–36) | < 0.001 |
| Number of shocks | 2 (1–4) | 2 (1–4) | 2 (1–4) | 0.31 |
| Mechanical CPR with LUCAS chest compression system | 11.1% | 10.9% | 11.2% | 0.94 |
| Airway control: | ||||
| Oropharyngeal/nasopharyngeal tube | 43.6% | 41.4% | 44.1% | 0.45 |
| Laryngeal tube/mask | 33.3% | 39.4% | 31.8% | 0.02 |
| Endotracheal intubation | 64.5% | 66.5% | 64.1% | 0.46 |
| Routes of medication administration: | 0.84 | |||
| Peripheral IV | 98.3% | 98.8% | 98.3% | |
| IO | 1.2% | 1.2% | 1.2% | |
| IT | 0.2% | 0.0% | 0.2% | |
| More than one | 0.3% | 0.0% | 0.4% | |
| Adrenaline | 96.5% | 93.5% | 97.3% | 0.004 |
| Amiodarone | 34.6% | 53.7% | 30.2% | < 0.001 |
| Atropine | 37.0% | 39.0% | 36.6% | 0.47 |
| Lidocaine | 0.4% | 0.8% | 0.3% | 0.24 |
| Magnesium sulfate | 2.7% | 6.9% | 1.7% | < 0.001 |
| 12-lead ECG after ROSC | 88.2% | 85.7% | 89.1% | 0.33 |
| ECG e-transmission after ROSC | 35.5% | 53.8% | 28.5% | < 0.001 |
| Presence of ST-segment elevation after ROSC | 27.4% | 43.2% | 20.6% | 0.005 |
| Prehospital outcomes: | ||||
| ROSC | 36.3% | 53.4% | 32.4% | < 0.001 |
| Survival to hospital admission: | < 0.001 | |||
| Survived event (hospital admission after ROSC) | 24.2% | 41.2% | 20.4% | |
| Transfer to the hospital with ongoing CPR | 4.2% | 2.1% | 4.7% | |
| Transfer to the hospital (ROSC status unknown) | 2.3% | 3.7% | 2.0% | |
| Time to the decision to cease CPR [min] | 36 (26–48) | 43 (33–57) | 35 (25–47) | < 0.001 |
In-hospital data were available for 281 patients. The clinical baseline characteristics of patients admitted to the hospital are shown in Table III. Among them, 94.3% achieved ROSC before arrival, 54.4% had previous coronary artery disease, and approximately one-fifth had a previous myocardial infarction. During the index hospitalization, one-third of event survivors underwent coronary angiography (34.5%), and coronary revascularization was performed in one-fourth of patients (25.3%). In addition, before hospital discharge, 4.6% received implantable cardioverter-defibrillator implantation. No patients received extracorporeal membrane oxygenation (ECMO) therapy in our cohort, neither as extracorporeal CPR nor as post-resuscitation shock treatment.
Table III
Baseline characteristics, in-hospital treatment, and outcomes of all patients who survived until hospital admission and the subgroups of patients who met and did not meet the Utstein comparator group criteria
| Variable | All patients admitted to the hospital N = 281 | Utstein comparator group n = 89 | Non-comparator group n = 192 | P-value |
|---|---|---|---|---|
| Patient demographics, prehospital factors, and status on admission: | ||||
| Age [years] | 63.9 (55.7–75.0) | 61.0 (54.6–70.3) | 66.0 (56.1–75.3) | 0.16 |
| Sex (male) | 64.8% | 78.7% | 58.3% | < 0.001 |
| First shockable rhythm | 41.9% | 100.0% | 11.2% | < 0.001 |
| Bystander or EMS witnessed event | 92.8% | 100.0% | 89.5% | < 0.001 |
| ROSC before admission | 94.3% | 98.8% | 92.2% | 0.02 |
| Medical historya: | ||||
| HF | 27.4% | 27.0% | 27.6% | 0.91 |
| Hypertension | 68.0% | 74.2% | 65.1% | 0.13 |
| AF | 13.2% | 14.6% | 12.5% | 0.63 |
| CAD | 54.4% | 59.6% | 52.1% | 0.24 |
| Previous MI | 18.1% | 24.7% | 15.1% | 0.052 |
| Previous PCI | 14.6% | 21.4% | 11.5% | 0.03 |
| Previous CABG | 4.6% | 7.9% | 3.1% | 0.08 |
| Previous ICD | 1.1% | 0.0% | 1.6% | 0.24 |
| Previous CRT-D | 0.7% | 1.1% | 0.5% | 0.58 |
| Previous stroke | 11.4% | 9.0% | 12.5% | 0.39 |
| PAD | 2.8% | 2.4% | 3.1% | 0.68 |
| In-hospital treatmenta: | ||||
| Coronary angiography | 34.5% | 65.2% | 20.3% | < 0.001 |
| PCI | 24.2% | 49.4% | 12.5% | < 0.001 |
| CABG | 1.1% | 3.4% | 0.0% | 0.01 |
| ICD/CRT-D implantation | 4.6% | 10.1% | 2.1% | 0.003 |
| Outcomesa: | ||||
| Duration of hospital stay [days] | 7 (1–18) | 13 (5–24) | 4 (1–15) | < 0.001 |
| Survival rate to discharge | 29.9% | 46.1% | 22.4% | < 0.001 |
| Survival rate to discharge (subgroup of patients admitted after ROSC) | 30.0% | 43.6% | 22.8% | < 0.001 |
a Based on administrative data from the National Health Fund database. AF – atrial fibrillation, CABG – coronary artery bypass grafting, CAD – coronary artery disease, CRT-D – cardiac resynchronization therapy defibrillator, EMS – emergency medical service, HF – heart failure, ICD – implantable cardiac defibrillator, MI – myocardial infarction, PAD – peripheral artery disease, PCI – percutaneous coronary intervention, ROSC – return of spontaneous circulation.
Of 281 patients admitted to the hospital, 89 (31.7%) were patients who met Utstein comparator group criteria. These patients were significantly more likely to be admitted to the hospital after ROSC and had previous percutaneous coronary interventions more frequently than the non-comparator group. On the other hand, there were no significant differences in terms of other cardiovascular comorbidities between groups. During the index hospitalization, patients with witnessed cardiac arrest and first monitored shockable rhythm more often received coronary angiography, revascularization, and cardioverter-defibrillator implantation.
Among all patients admitted to the hospital after ROSC or during ongoing CPR, 29.9% survived to hospital discharge. The proportion of patients discharged alive from the hospital was over two times higher in the Utstein comparator group than in the non-comparator group (46.1% vs. 22.4%; Table III). The cumulative survival to hospital discharge for all included patients and subsets of patients who met and did not meet the Utstein group criteria was 9.2%, 21.7%, and 6.1%, respectively.
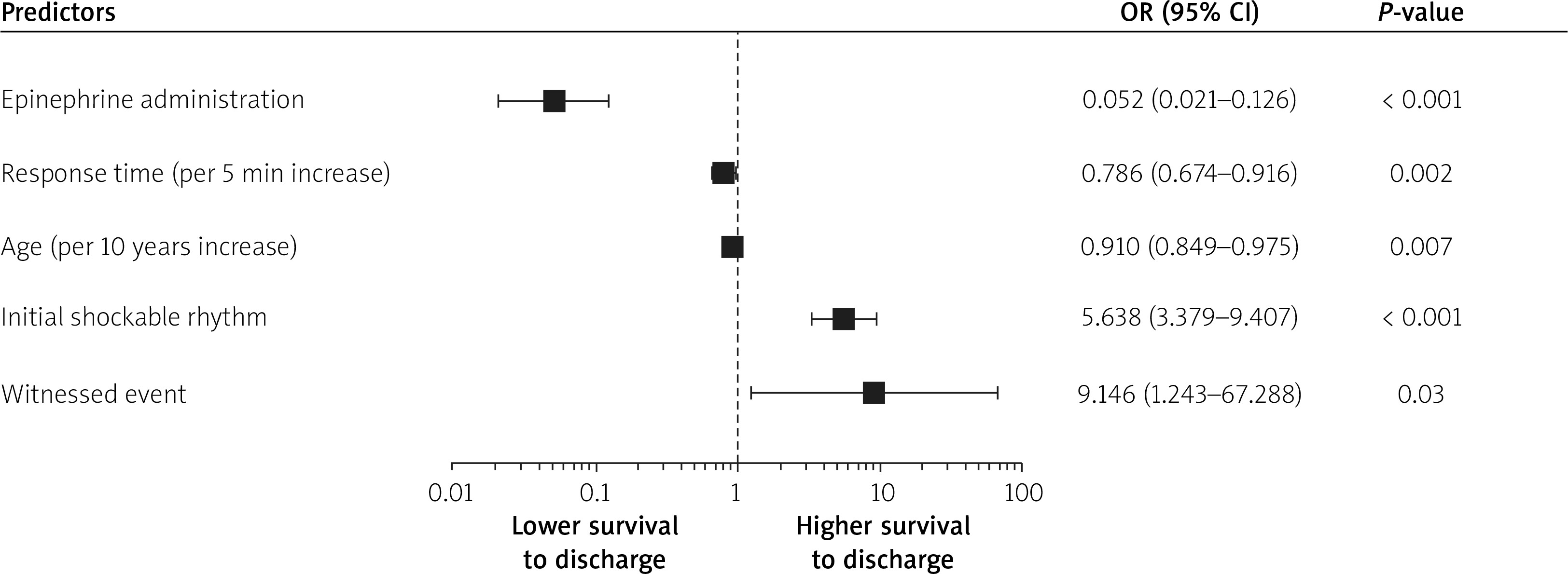
Univariate logistic regression analysis revealed that the need for epinephrine administration, cardiac arrest occurring at home, longer EMS response time, older age, non-shockable rhythm, and unwitnessed events were associated with increased prehospital and in-hospital mortality. On the other hand, malignant neoplasm, previous stroke and myocardial infarction, sex, etiology of OHCA, as well as endotracheal intubation were not significantly associated with survival to discharge. The results of univariate analysis are shown in Table IV. In addition, the multivariable analysis identified epinephrine administration, witnessed cardiac arrest, response time, age, and initial rhythm as independent predictors for survival to discharge in the SIL-OHCA cohort (Figure 2).
Table IV
Factors associated with survival to discharge – results of univariate logistic regression analysis
Discussion
Recent registry-based studies provided much data on epidemiology, characteristics, and prehospital outcomes of patients with OHCA in Poland [2–7, 11–17]. However, most of those studies were limited by retrospective character or small sample size, or presented only prehospital or in-hospital data. The so-called Utstein-style guidelines, published for the first time in 1991 and last updated in 2014, are a set of expert recommendations on OHCA data reporting [18, 19]. These guidelines enable collection of uniform data on OHCA and comparison of the efficacy of different EMS systems between countries [10, 20, 21]. None of the previous reports on OHCA in Poland have contained all of the core elements, according to Utstein style recommendations [10].
Considering previous studies’ limitations, we performed a comprehensive analysis of registry-based Utstein-style data collected during 12 months in a population encompassing 2.7 million inhabitants of southern Poland (Upper Silesia). We observed 54.5 EMS treated OHCA cases per 100,000 population during this period. That is similar to previous studies from Poland, which showed the OHCA incidence rate of 34.7 to 156.0 per 100,000 per year [3, 12, 13, 15, 16, 22, 23]. In the most extensive of these studies, retrospective analysis based on EMS medical charts, the prevalence of EMS treated OHCA varied between regions of Poland (range 58.9/100,000 to 84.5/100,000 per year) [15]. Our results are also in line with the EuReCa TWO study encompassing data from 28 European countries, which reported the mean incidence rate of started resuscitations of 56 per 100,000 population per year (range 27-91 per 100,000 population per year) [24].
Prehospital outcomes of SIL-OHCA patients are similar to those included in EuReCa TWO as well [24]. In our registry, ROSC was achieved in 36.3% of the entire group (vs. 32.7% in the EuReCa TWO cohort), and 24.2% of patients were admitted to hospital with ROSC and 4.2% during ongoing CPR (vs. 25% and 11% in EuReCa TWO, respectively) [24]. According to previous studies from Poland, the rate of ROSC ranged from 30.48% to 42.3% [4, 12, 16] and was slightly higher in cases of OHCA to which Helicopter Emergency Medical Service (HEMS) teams were dispatched (45.7%) [2]. Moreover, in the retrospective study by Nadolny et al., the survival rate to hospital admission or transfer to HEMS was 36.3% [15].
Very little data exist on in-hospital outcomes of patients after OHCA in Poland. In two previous studies, based on the registry of patients treated with hypothermia (The Polish Registry of Therapeutic Hypothermia) and the registry of invasive cardiac procedures (National Registry of Invasive Procedures – ORPKI), the percentage of patients who survived to hospital discharge was 81% and 87%, respectively. However, one must note that these studies refer to highly selected groups of patients after OHCA [14, 25]. In the cohort of consecutive OHCA patients admitted to the hospital with sustained ROSC in 2004, the survival rate was 31.9%, which is much lower than in the studies mentioned above and was similar to our results, where 30.0% of these patients survived to discharge [13]. These results might suggest that in-hospital outcomes of patients after OHCA have not changed substantially over this period; however, we could not exclude the effect of confounding factors since OHCA patients’ characteristics might have changed over these years. None of the previous studies have provided in-hospital outcomes of unselected Polish patients with OHCA (regardless of ROSC status on admission) to the best of our knowledge. Among all patients admitted to the hospital in our cohort, 29.9% were discharged alive, and it was slightly higher than the in-hospital survival rate of patients included in the whole EuReCa TWO population but much lower than in leading countries included in this study (26.4% in the entire cohort, ranging between 0% and 48%).
While the success rate of CPR in patients with OHCA depends on many factors, including the prevalence of demographic, social, and economic factors in a given population, patients with witnessed collapse and initial shockable rhythm constitute a relatively homogeneous group (the Utstein comparator group), which enables the comparison of various EMS systems’ efficacy. In our study, among patients who met Utstein comparator group criteria, the prehospital and in-hospital outcomes were similar to other countries, according to EuReCa ONE and TWO studies [24, 26]. Utstein group patients were more frequently diagnosed with STEMI and were less likely to be admitted to the hospital without sustained ROSC. Moreover, EMS response times were shorter in these cases compared with patients who did not meet Utstein comparator group criteria. Finally, the in-hospital survival rate of the Utstein comparator group was over twice as high as in other patients who were admitted to the hospital after OHCA.
As reported by us, prehospital and in-hospital outcomes after OHCA in the Polish population, even though similar to average outcomes in other European countries, are still much worse than in some Western European countries such as the Netherlands and Denmark [24, 26, 27]. Although bystanders witnessed 66.8% of OHCA events, only in about half of cases did laypeople start CPR before EMS arrival. In most attempted CPR cases, the dispatcher provided CPR instructions to the event witnesses, confirming the dispatcher’s significant role in OHCA management. The quality of basic life support (BLS) probably requires improvement as well, since ventilation was not performed in the three-fourths of patients who received CPR [1]. Educational campaigns on BLS are necessary to increase the frequency and quality of layman CPR [28].
Moreover, our study showed that bystanders performing CPR used AED only in 4.6% of cardiac arrest cases before EMS arrival. The reason for that might be the limited availability of AEDs in public places, limited knowledge of OHCA witnesses regarding the use of AEDs, and the fact that most cardiac arrests occurred at home. Nevertheless, in countries that introduced voluntary first responders to attend OHCA events (unlike Poland), the frequency of AED use and defibrillation shocks delivered before EMS arrival is higher, which results in better prehospital and in-hospital outcomes of patients with OHCA, as compared to the results of our study [29–31].
In addition, our study confirmed the value of the need for epinephrine administration, witnessed cardiac arrest, response time, age, and initial rhythm as independent predictors of survival to hospital discharge in SIL-OHCA patients. Despite being well known, these predictive factors have mostly not been analyzed in the Polish cohort of OHCA patients to date [32].
The limitation of our study is a relatively high volume of missing data on in-hospital patient management and outcomes, which were gathered retrospectively from the administrative database. A similar proportion of missing data has been reported in other OHCA registries [24, 33]. Prospective collection of structured in-hospital data might help to overcome this limitation in future OHCA registries. Moreover, given the retrospective nature of in-hospital data analysis, we could not assess both the implementation of targeted temperature management (which might improve survival in patients after OHCA [14, 34]) and neurological outcomes at hospital discharge, which are not routinely reported to the NHF.
Conclusions
The prehospital and in-hospital survival rates of patients after OHCA in Poland are low. Only one-fourth of EMS-treated patients after OHCA are transported to the hospital after ROSC, and less than 30% of hospitalized patients are alive at hospital discharge. There is still room for improvement in increasing the prevalence of CPR performed by bystanders and AED use before EMS arrival.
ClinicalTrials.gov Identifier: NCT03654859.







