
Introduction
Current treatments for metastatic liver cancer, hepatocellular carcinoma, and other liver tumors include liver resection, chemotherapy, radiofrequency ablation and other local ablative therapies, transarterial chemoembolization, and liver transplantation [1–4]. Among these, liver resection is currently recommended as the most reliable therapy.
Over the past 20 years, the noninvasive nature of laparoscopic surgery as an alternative to conventional open procedures in gastrointestinal and many other surgical fields has led to dramatic developments. Now, partial hepatectomy and a variety of other liver resections can be performed laparoscopically [3–5]. Many studies have shown that, as an initial surgery for liver tumors, laparoscopic partial liver resection is associated with better short-term outcomes than open partial liver resection, in that it has less intraoperative bleeding, lower rates of surgical site infection, and shorter postoperative hospital stays. It is also preferred owing to its low degree of invasiveness and for aesthetic reasons. This is the result of advances in the instruments used in laparoscopic surgery and improvements in laparoscopic liver resection technique.
Meanwhile, as the geriatric proportion of the population increases, so do conditions requiring operation on elderly patients [6]. A grave problem facing the medical world is responding to the aging of society. As many elderly patients have various comorbidities in circulatory, respiratory, renal, and other important organs and systems [7], less invasive therapies are often selected. While laparoscopic surgery is a less invasive therapy, accurate assessment of surgical risk for patients with comorbid conditions and appropriate perioperative management are extremely important for preventing fatal complications, extended postoperative hospital stays, and increased medical costs. Addressing comorbidities is a particularly urgent priority in the field of gastrointestinal surgery, which includes surgery for diseases of the liver, biliary tract, and pancreas.
With the number of patients with comorbidities, especially cardiac disease, increasing every year, the objective of the present study was to examine the preoperative statuses, perioperative outcomes, and postoperative courses of such patients undergoing laparoscopic liver resection (LLR). We also discuss the problems involved and review the relevant literature.
Material and methods
Patient population and selection
LLR was introduced in our hospital in 1998. Since then, we have gradually standardized the surgical procedure. By 2010, the procedure of LLR was well established due to the cumulative degree of experience acquired over time. Therefore, the subjects of this study were patients who underwent this standardized procedure from 2010 onward.
Between February 17, 2010, and June 13, 2018, we conducted LLR for liver tumors on 339 consecutive patients at Osaka Medical College Hospital in Takatsuki City, Japan. Liver resection was performed whenever a liver tumor could be curatively resected. A tumor size less than 10 cm was the main criterion for LLR. There was no limitation on the number or size of liver tumors with regard to hepatic functional reserve after resection. Patients with portal or hepatic venous involvement and/or metastasis to adjacent organs were not considered candidates for LLR. We evaluated hepatic function using the Child-Pugh classification [8] of liver dysfunction. Patients with complicated cirrhosis (Child-Pugh class C), in whom liver resection would not be appropriate, were excluded from the study. All patients were fully informed of the study design and provided their written, informed consent to participate. This study was approved by the Ethics Committee on Clinical Investigation of Osaka Medical College Hospital (No. 1828 and 1997).
Criteria to convert laparoscopic to open liver resection were as follows: 1) liver stumps of preserved and resected sides that could not both be expanded adequately; 2) uncontrollable intraoperative bleeding; 3) blood loss exceeding 500 ml; 4) total time of Pringle maneuver (hepatic blood flow occlusion) exceeding 120 minutes; 5) uncontrollable intraoperative bile leakage.
Surgical procedure
In this series, all patients received potentially curative liver resection with the complete removal of gross tumor with negative macroscopic margins. All procedures were performed by three experienced hepatobiliary surgeons (YI, FH, KU) during the study period.
All procedures were performed under general anesthesia. The detailed laparoscopic surgical technique routinely used in our department has been described in previous reports [3, 4, 9, 10]. Briefly, patients with tumors involving the right hepatic lobe were placed in a left lateral recumbent position. Patients with tumors involving the left hepatic lobe were positioned supine.
After the introduction of a 12-mm umbilical or other port using an open technique, continuous carbon dioxide (CO2) pneumoperitoneum was induced at a pressure limit of 12 mm Hg at a flow rate of 6 l/min to decrease the risk of gas embolism. Four 5- to 12-mm trocars and a 30-degree laparoscope (1588 AIM; Stryker Japan K.K., Tokyo, Japan) were fixed. For patients with cephalad tumors involving the right hepatic lobe (segment VII and VIII), an intercostal port was inserted (two ports for segment VII; one port for segment VIII).
The mobilization of the liver was then initiated. The lateral hepatic attachment and the triangular ligament were divided using a surgical tissue-management system (Thunderbeat, Olympus Inc., Tokyo, Japan) after the round and falciform ligaments were dissected. This dissection was typically carried up to the diaphragm, allowing more effective mobilization of the liver.
Then, the liver was evaluated in all cases using intraoperative laparoscopic ultrasonography (Prosound α7, Hitachi Aloka Medical Ltd., Tokyo, Japan). In addition to intraoperative ultrasonography, laparoscopic indocyanine green (ICG)-fluorescence imaging was also used to facilitate tumor identification. In ICG-fluorescence imaging, tumors on the liver surface in particular appear fluorescent green, and thus the tumor sites are easily identified.
Next, to perform an extracorporeal Pringle maneuver, blood flow was occluded by clamping a vascular occlusion tube (Vessel-Clude, Argon Medical Devices Inc., USA) from outside the body after adhesion of the hepatic hilar region was confirmed. Intermittent clamping was applied, with 15-minute clamping and 5-minute release periods.
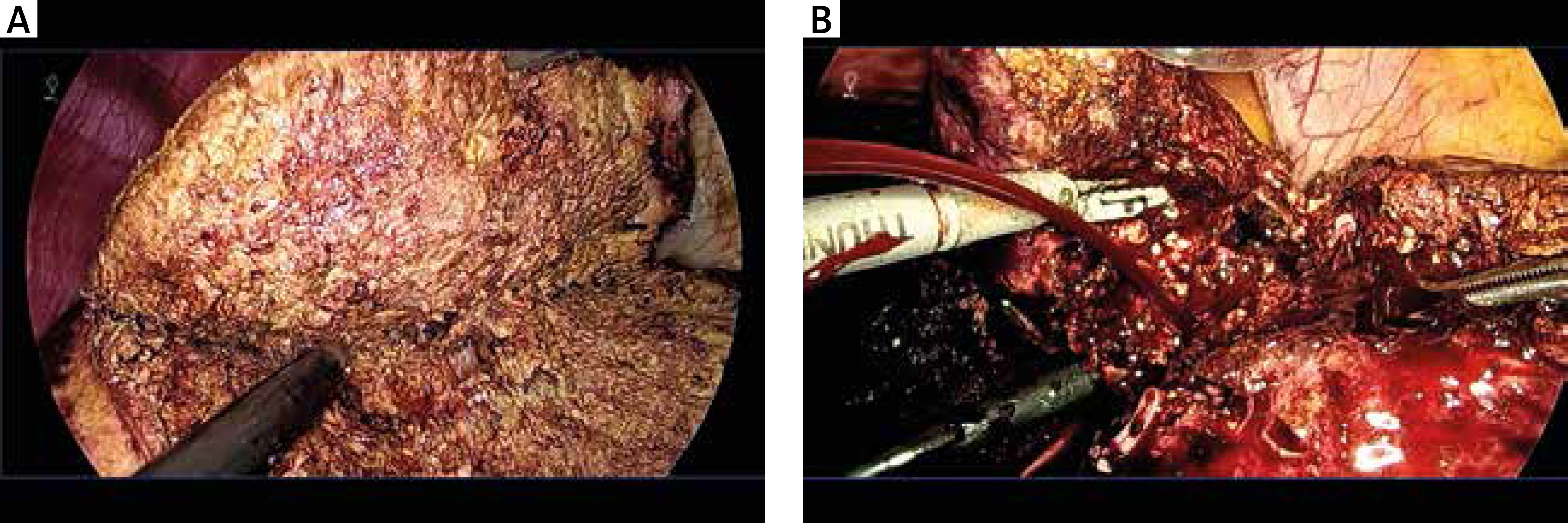
By changing the port of insertion for the laparoscope, the operator formed a triangle with the laparoscope in the center, placing the operator, target area, and the laparoscopic monitor in a straight line, maintaining the co-axial position. Central venous pressure (CVP) was maintained at 0–3 mm Hg during parenchymal transection. Parenchymal transection was achieved using the Cavitron Ultrasonic Surgical Aspirator (Integra CUSA Excel Plus, Integra Neurosciences Ltd, Andover, UK) and Thunderbeat under an extracorporeal Pringle maneuver (Fig. 1A). Small vessels were ligated or coagulated using a soft-coagulation system. Intraparenchymal control of the major vessels was achieved with clips, whereas vascular and biliary radical occlusion were achieved using either clips or staples. Then, the laparoscopic Pringle maneuver was performed. The resected specimen was placed undivided in a plastic retrieval bag and removed through the slightly enlarged periumbilical incision.
Fig. 1
The cut surface of the liver during hepatic parenchymal resection: A) without severe cardiac disease, B) with severe cardiac disease. In patients without severe cardiac disease, intraoperative blood loss can be decreased, surgery can be performed safely, and the isolated side of the liver can be kept dry. In patients with severe cardiac disease, CVP values may increase, as in this case with free bleeding from the incised side of the liver
Data examined included preoperative factors, surgical factors, and pathological factors.
Preoperative factors
Preoperative factors investigated were age, sex, body mass index (BMI), viral hepatitis infection status, left ventricular ejection fraction, pathology, total bilirubin, albumin, prothrombin time (PT), platelet count, and Child-Pugh classification.
Surgical and pathological factors
Surgical factors included open conversion rate, CVP, surgical duration, intraoperative blood loss, and blood transfusion requirements. Pathological factors evaluated included the size of the largest tumor, number of tumors, and surgical margin status. “R” classification denoted the absence or presence of residual tumor after surgery [11]. R0 resection refers to excision of the tumor in one piece without violating the tumor plane or achieving negative margins after sequential re-excision of the involved margins. R1 resection involves a microscopically positive margin anywhere, and R2 resection involves (a) macroscopically positive margin(s) with visible tumor.
Postoperative evaluation
The following parameters were evaluated: transfusion rate, pathological margins, postoperative complications, 30-day mortality, and hospital stay. Morbidity was graded according to Clavien’s classification [12, 13]. Surgical site infections (SSIs) were defined according to the CDC’s National Nosocomial Infection Surveillance (NNIS) system [14].
Statistical analysis
Continuous variables were expressed as median ±standard deviation. Univariate analysis results were compared using Student’s t test, χ2 test, Mann-Whitney U test, Wilcoxon signed-rank test, or Fisher’s exact test, as appropriate. Values of p < 0.05 were considered statistically significant. All statistical analyses were performed using JMP version 12 (SAS Institute, Inc., Cary, NC, USA).
Results
Patient demographics
LLR was performed on 339 patients, one of whom had pre-existing severe valvular disease before therapy. In this case, CVP rose to 10 mm Hg, and multiple eruptions of venous blood from the transected liver surface were observed during parenchymal transection, despite performing total hepatic blood flow occlusion (Fig. 1B). Moreover, blood pressure decreased, and we converted to open liver resection for hemodynamic instability. Therefore, this case was excluded from this study. In all other patients, LLR was performed after cardiac functions were stabilized.
Of the remaining 338 patients who had undergone LLR, 16 had concomitant cardiac disease, and 322 patients were without concomitant cardiac disease. The group with coexisting cardiac disease included 13 patients being treated with medication for unstable angina, two patients with valvular disease, and two patients with cardiomyopathy. While the group without cardiac disease did not undergo echocardiography or any other preoperative examinations, their left ventricular ejection fraction was better than the mean of 66% (22–74%) observed among patients with cardiac disease (Table 1). There were no significant differences in demographic (except for age) or operative characteristics between the groups. Surgical outcomes are reported in Table 2.
Table 1
Preoperative clinical and laboratory patient data
| Parameter | Cardiac disease | No cardiac disease | p-value |
|---|---|---|---|
| Number, n | 16 | 322 | |
| Age, years | 77 (62–84) | 69 (13–93) | 0.008* |
| Sex (M/F) | 13/3 | 194/128 | 0.092 |
| Body mass index, kg/m2 | 22.7 (17.8–34.5) | 22.8 (15.4–35.3) | 0.668 |
| HCC/CCC vs. others | 11/5 151/171 | 0.088 | |
| Hepatitis viral infection, n (%) | 6 (37.5) | 148 (46) | 0.507 |
| Serum albumin, g/dl | 4.0 (3.1–4.7) | 4.0 (2.6–5.2) | 0.824 |
| Serum total bilirubin, mg/dl | 0.4 (0.3–1.0) | 0.6 (0.2–2.1) | 0.088 |
| Prothrombin time, n (%) | 97 (64–117) | 101 (43–150) | 0.247 |
| Platelet count, ×104/μl | 17.0 (9.3–26.2) | 17.7 (2.6–45.5) | 0.507 |
| ICGR-15, n (%) | 9.6 (3.8–49.3) | 13.2 (0.4–72.2) | 0.852 |
| Child-Pugh classification, A, n (%) | 16 (100) | 312 (96.9) | 0.474 |
| PNI | 45.4 (38.1–51.2) | 47.7 (32.3–64.3) | 0.051 |
| EF, n (%) | 66 (22–74) | – | |
| Number of lesions | 1 (1–4) | 1 (1–12) | 0.592 |
| Size of largest tumors, cm | 2.6 (1.5–4.8) | 2.4 (0.6–7.5) | 0.704 |
| Total liver volume, cm3 | 1045 (782–1594) | 1125 (689–2675) | 0.140 |
Table 2
Outcomes of hepatic resection surgery
The Pringle maneuver was performed in 11 of the 16 patients (68.8%) in the cardiac group and in 170 of the 322 patients (53.5%) in the non-cardiac group (p = 0.231). LLR was performed after cardiac functions were controlled in all 16 patients with cardiac disease, and there were no instances of increased CVP or destabilized vital signs during surgery. Intraoperative CVP did not differ between the groups (p = 0.521).
No significant differences were observed in surgical time, amounts of bleeding, intraoperative transfusion volume, or other outcomes. Furthermore, no differences in the rate of Clavien 3A or higher complications, postoperative bile leakage, post-hepatectomy liver failure incidence, or postoperative hospital stay were observed (p = 0.733, 0.229, 0.698 and 0.713, respectively).
Discussion
We have previously reported on the low invasiveness of laparoscopic liver resection compared to open liver resection, primarily with regards to reduced intraoperative bleeding [5, 14]. There have been many similar reports in recent years, and while surgical instrumentation and techniques have improved, intraoperative bleeding still requires the most attention in laparoscopic liver resection. This is because intraoperative bleeding greatly affects surgical outcomes, primarily conversion to open surgery and the incidence of postoperative complications.
During laparoscopic liver resection, the greatest increase in intraoperative bleeding is during parenchymal transection. Bleeding during parenchymal transection can occur from hepatic arteries, hepatic veins, or portal veins. Limited forceps movement and difficulty developing a field of view during laparoscopic liver resection can make it difficult to address these kinds of bleeding. As we have reported previously, at our institution the first choice for addressing intraoperative hepatic arterial and portal vein bleeding during laparoscopic liver resection is occluding blood flow to the liver using the Pringle maneuver [15]. The Pringle maneuver was first reported in 1908 by Pringle et al. as a method of occluding blood flow to the liver during open surgery [16] and is now used throughout the world. Randomized controlled trials (RCTs) have shown that it can reduce bleeding during liver transection without impacting liver functions [17]. Options for addressing venous bleeding during laparoscopic liver resection include increasing pneumoperitoneal pressure, reducing CVP, reducing the ventilatory volume, and reducing positive end expiratory pressure (PEEP) [18–20]. If possible, CVP is lowered to 0–3 mm Hg, ventilatory volume to 6.5–7 ml/kg, and PEEP to 0 mm Hg.
However, as the cases examined in the present study indicate, these countermeasures may be insufficient to address intraoperative bleeding in certain environments, such as in patients who present with severe cardiac comorbidities before therapy. In the presence of cardiac comorbidities, increasing pneumoperitoneal pressure or decreasing cardiac output can raise CVP, which can increase venous bleeding on the liver parenchymal transection surface [21]. Furthermore, while laparoscopic liver resection may be a less invasive procedure involving less postoperative pain, intestinal paresis, and tissue disturbance, the increase in pneumoperitoneal pressure and decrease in venous return can reduce cardiac output and raise peripheral vascular resistance, which may actually increase the risk of acute complications [22].
Occasions for operating on patients with some type of cardiac disease are increasing, particularly in developing countries facing unprecedented aging of their societies. In patients with latent or well-defined cardiac disease, the invasiveness of liver resection carries a risk of causing fatal cardiac complications. This must be addressed during laparoscopic liver resection.
The objective of preoperative cardiovascular assessments is not only to obtain information needed to execute the surgery safely, but also to establish a comprehensive treatment plan for patients with coexisting cardiovascular diseases [23–25]. In addition to the severity of the cardiac disease, factors such as the patient’s age, the invasiveness of the planned surgery, survival prognosis, quality of life, and the presence or absence of other severe complications should be given comprehensive consideration.
Based on the ACC/AHA and other guidelines [24, 25], if the cardiac complications are not severe and a low-risk procedure is planned, a more extensive cardiovascular assessment is not considered necessary. However, in the presence of risk factors such as severe cardiac disease – which may include unstable angina, recent acute myocardial infarction, acute heart failure, high-grade atrioventricular block, uncontrolled ventricular tachycardia and other forms of severe arrhythmia, or severe valvular disease – a detailed assessment of the cardiovascular system should be performed preoperatively and the surgery should be performed only after the condition has been treated and stabilized [26]. Basically, a cardiovascular specialist should be consulted to perform a detailed examination, and a change in treatment method should also be considered. While performing a planned liver resection is extremely important, in some patients treating cardiovascular diseases should be prioritized. Simply changing the order of treatments may help ensure a good long-term prognosis. Even if these precautions do not have an impact on the surgery itself, they may be helpful in general postoperative management.
Conclusions
Currently, the procedures used in LLR can be modified in several ways to ensure the operation is carried out safely, leading to less invasiveness and better outcomes than open liver resection. However, as society ages there will be more patients with coexisting cardiac disease who require full preoperative assessments. Patients with non-severe or controlled severe cardiac disease did not exhibit different postoperative courses compared to the patients without coexisting cardiac disease. The presence of severe cardiac disease before LLR can lead to unstable vital signs during surgery, such as increased CVP. In such cases, treating the cardiac disease should be prioritized, and ideally it should be controlled before proceeding with LLR. Limitations of this study include the small number of subjects and a variety of possible biases, such as those related to the types of cardiac disease, variations in treatment of pre-existing cardiac disease, or the types and quality of the liver resections. In future, larger sample sizes and further study through RCTs or meta-analyses are needed.






