
Introduction
Leiomyosarcoma of the rectum (LMS) is a rare entity that comprises less than 0.1% of all rectal malignancies [1]. The prognosis in anorectal LMS, i.e. 5-year overall survival and disease-free survival are approximately 75% and 46%, respectively [2]. The standard of care involves surgical resection with optional adjuvant chemotherapy based on doxorubicin [3]. The choice of the applied treatment is usually based on radiographic findings, i.e. computed tomography (CT) and positron emission tomography (PET) imaging. Although the high efficiency of these methods in the identification of primary soft-tissue tumours is widely recognized, there are numerous reports of their limited specificity and sensitivity for the detection of metastases [4]. As presented here, these shortcomings of PET/CT, further accentuated by an unusual presentation of the metastatic lesion, may lead to an unprecedented diagnostic challenge and dismal disease outcome.
Case report
A 44-year-old patient was admitted to the Department of Surgery in December 2006 for complaints of blood in stool and difficult defecation. He was a non-smoker, did not consume alcohol, and had no history of previous surgery. Results of the blood tests, except for the lowered levels of haemoglobin (11.5 g/dl) and haematocrit (33.6%) indicative of anaemia, were within normal range. On physical examination, a palpable mass was found in the anal canal. Abdominal contrast-enhanced computed tomography (ceCT) revealed a nodular lesion 44 × 41 × 35 mm in size, approximately 80 mm from the anal verge. In addition, abdominal CT showed a well- demarcated lesion 5 mm in diameter in the anterior subcapsular area of the right lobe of the liver (Fig. 1 A). However, because PET imaging did not show any signs of elevated glucose metabolism in this area, the disseminated process was categorically ruled out. The lesion was diagnosed as a benign cyst, and surgical resection of a part of the rectum and sigmoid colon containing the tumour was performed. The histopathological and immunohistochemical examination revealed a non-epithelial malignant neoplasm positive for desmin and negative for cytokeratins, CD117, and S100. Based on histopathological and immunohistochemical results, a diagnosis of leiomyosarcoma G3 was put forward (Fig. 2 A, B).
Fig. 1
Radiographic computed tomography study of the lesion in the liver in 2007, a cystic lesion 5 mm in diameter (arrow) (A), 2009, the lesion 36 mm in diameter (arrow) (B)
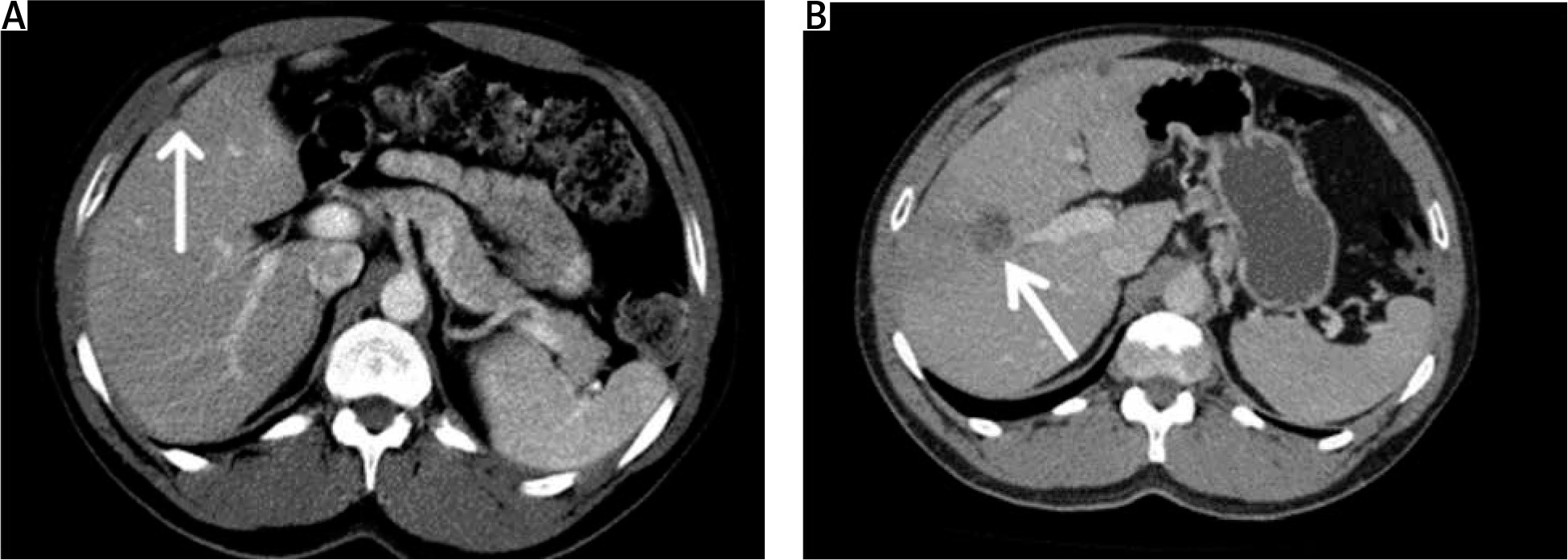
Fig. 2
Histopathological analysis of the metastasis in the liver. Haematoxylin and eosin staining showing high-grade metastatic neoplasm (40× and 100× magnification, respectively) (A, B), immunohistochemical staining for the caldesmon shows positivity on the periphery of the lesion (white arrow) and the necrosis in the centre (black arrow) (40× magnification) (C), immunohistochemical staining demonstrates positivity for caldesmon (arrow) (100× magnification) (D)
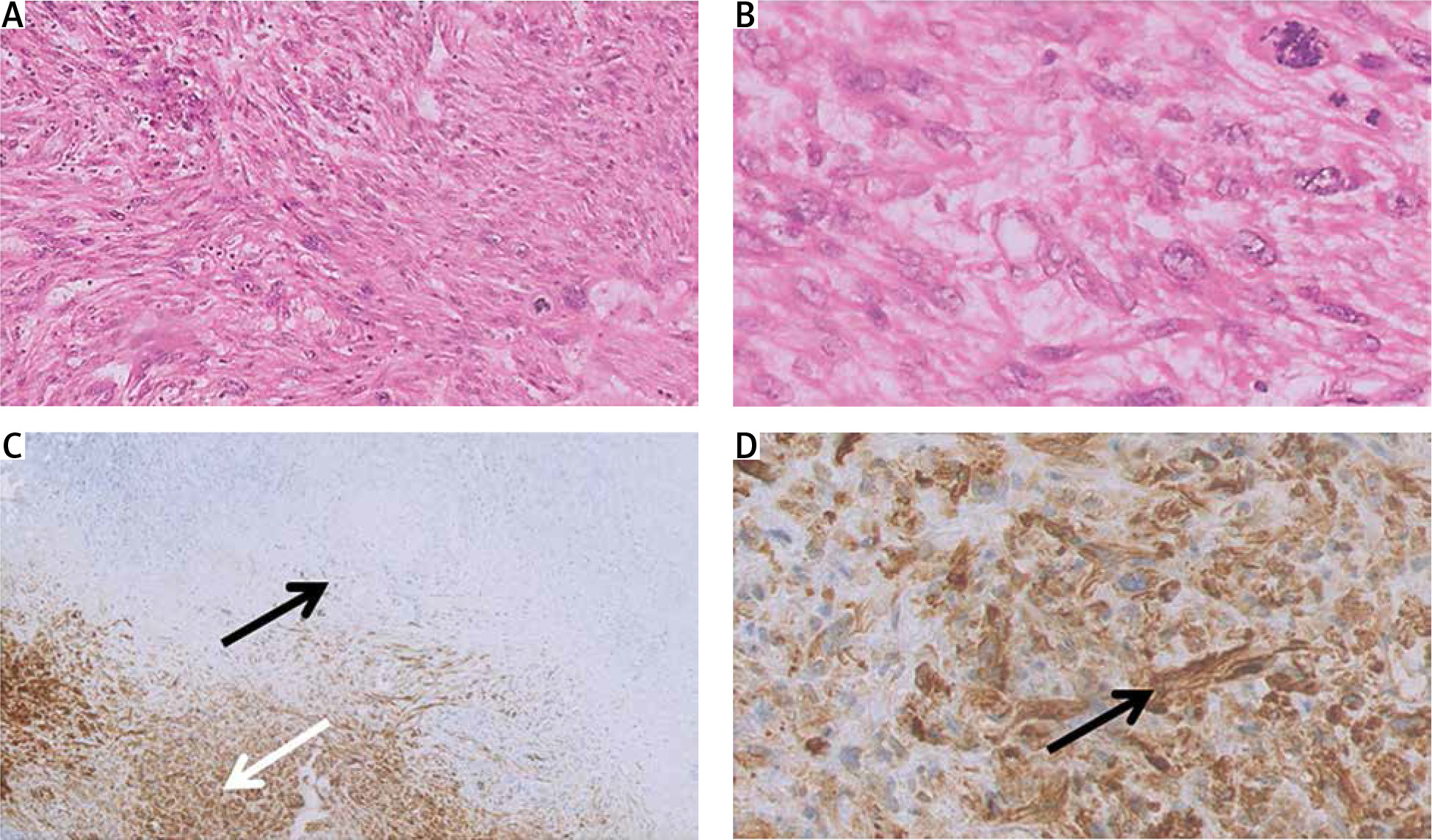
During the 3-year follow-up, the patient was in good clinical condition (PS0 on the ECOG scale), and the lesion in the liver was regularly monitored by ceCT and PET. Despite the lack of any features of disease dissemination as assessed by both ceCT and PET (5 ceCT and 6 PET scans in total in that period), deterioration of the patient’s condition in January 2010 (PS1 on the ECOG scale) prompted a biopsy of the lesion. The histopathological examination showed areas of extensive central necrosis and fibrosis in its centre (Fig. 2 C), with atypical cells on the periphery, positive for desmin, HHF35, MIB, and caldesmon and negative for CD117, CD34, myogenin, and SMA (Fig. 2 D), consistent with metastasis of leiomyosarcoma. A subsequent ceCT scan of the abdomen revealed multiple solid lesions in the liver ranging from 10 to 36 mm in diameter with homogenous enhancement (Fig. 1 B). Surgical resection of the right lobe and local excision of the lesion from the 2nd segment was performed, and the patient received treatment according to the ADIC regimen (doxorubicin, dacarbazine). A ceCT scan performed 3 months later revealed in the lungs 2 irregular solid structures 25 × 16 mm and 31 × 23 mm in size and expansion of the previously described lesions in the liver, indicative of disease progression, and chemotherapy with 7 cycles with Taxol and gemcitabine was administered. During chemotherapy (May – November 2011), apart from persistent lymphopaenia (2.71 × 103/ul), morphological parameters remained within normal range and the patient’s physical condition remained stable (PS0 on the ECOG scale). A consecutive ceCT scan performed one month after the completion of the prescribed course of chemotherapy revealed 3 new hypodense lesions in the liver (scan of the lungs remained unchanged), which led to the decision of the 3rd-line treatment, namely one cycle of trabectedin (consisting of 3 consecutive doses). Three days after the last administration of the trabectedin (2 months after implementation of this therapy) the patient was referred to the hospital due to acute dyspnoea, swelling of the lower limbs, and oliguria. Results of the blood test revealed increased levels of troponin T (766.8 pg/ml), creatinine (3.1 mg/dl), urea (87.9 mg/dl), and CK-MB (229 U/l), which indicated trabectedin-induced rhabdomyolysis and renal failure, and the patient was admitted to the Department of Nephrology for urgent medical intervention. However, this was ineffective, the patient’s condition rapidly deteriorated, and he died within 2 days.
Oral informed consent was obtained from the patient’s next of kin for publication of this case report and any accompanying images.
Discussion
Here we present an unusual case of a metastatic rectal leiomyosarcoma, whose secondary lesion in the liver was, for the 3 years of observation accounted in this report, perceived by ceCT and PET as a stable pseudocyst of small diameter (5 mm). To our knowledge, this is the first report of a liver LMS metastasis that, despite its small size, developed central necrosis and thus, portraying as a pseudocyst, generated false-negative results by both CT and PET. The scans were performed at regular intervals over 3 years, but the progression of the disease was never picked up. A necrotic mass in the centre of the lesion, which was probably responsible for the misdiagnosis, could be revealed only by histopathology.
Metastases in the liver, the most common site of metastatic spread from rectal malignancies [5], usually form solid lesions easily detected by CT and PET scans. Although PET has been commonly recognized as a modality of maximum sensitivity and specificity, numerous reports demonstrate that combining PET and CT imaging (PET/CT) is often crucial for the diagnostic process [6]. For example, higher accuracy of PET/CT than PET alone was documented in a study evaluating the staging of colorectal cancer [7]. PET/CT was also shown to enable the correct diagnosis of liver lesions, undetectable by CT alone [8]. Conversely, in some cases, an additional CT scan was required to establish an accurate diagnosis [4, 9]. CT imaging was shown to have a higher sensitivity for detection of intrathoracic metastasis [10]. Roberg et al. reported cases of different types of sarcomas, where 10/91 PET negative results of distal metastasis turned out to be incorrect, while CT scans provided reliable data [4]. In a study by Bélissant et al., in 2 described cases of patients with leiomyosarcoma, metastases in the lung and peritoneum were not detected by PET [11]. However, the use of CT alone is not advisable either. As demonstrated in a study of a soft-tissue sarcoma by Roberge et al., analysis of PET but not CT scans enabled an accurate diagnosis [4].
False-negative results of PET scans are usually reported in high-grade tumours, small lesions, or large tumours with necrosis [12]. Both necrosis and poor differentiation are associated with a low level of glucose metabolism, which is probably responsible for the inability of PET to provide the correct results.
Development of pseudocysts in the liver can often be caused by infarction and liquefication of necrosis, but it usually takes place in cases with large lesions (> 5 mm) [13–15]. However, it must be emphasized that sensitivity of PET (i.e. t detectable threshold of tumour volume) varies between analysed anatomical locations [16, 17]. Although in the presented case the lesion was very small, the above process, even though extremely rare, seems to provide the most plausible explanation for the negative PET results.
In 2004, trabectedin was approved by US Food and Drug Administration (FDA) for the treatment of patients with soft tissue sarcomas. In 2015, based on the results of a single, randomized, active-controlled, 518-patient, multicentre study, FDA approval for trabectedin was further extended to include the treatment of patients with unresectable or metastatic liposarcoma and leiomyosarcoma who received a prior anthracycline-containing regimen [18]. Although in most cases the compound has shown a favourable toxicity profile, in some patients the treatment induced serious adverse reactions, including severe rhabdomyolysis (in 3 patients), and subsequent death (in one case) [19, 20]. Here we present another case of this rare but deadly side effect of trabectedin.
Conclusions
The reported case attempts to increase awareness of the diversity that forms rectal leiomyosarcoma can create. It also indicates that in the case of any rare neoplasm, radiographic findings should be perceived very critically, at best as a guidance, but not as the decisive factor for the choice of therapeutic strategy, the design of which should always be carefully selected.






