
Extragonadal germ cell tumours are rare neoplasms constituting 3–4% of all germ cell tumours and less than 1% of all tumours [1]. The mediastinum is the most common site for extragonadal germ cell tumours. Teratomas are the most common mediastinal germ cell tumours. Mature cystic teratoma is commonly known as dermoid cyst [2]. Cystic teratomas are mostly asymptomatic and are detected incidentally. However, they can present with clinical features of rupture in the adjacent areas such as the pleura, pericardium, lung or bronchus [2].
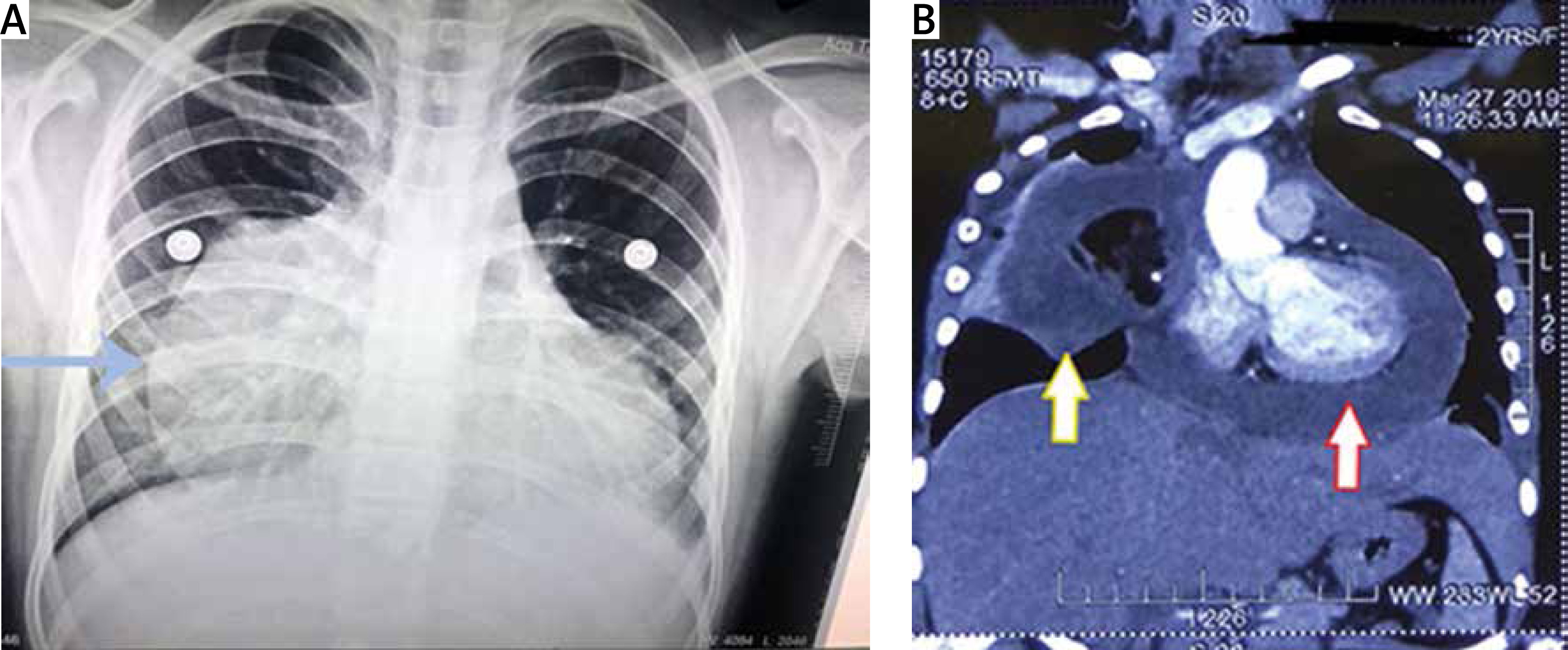
A 12-year-old female patient presented with a 7-day history of low-grade fever, cough, retrosternal chest pain, and generalized weakness. The patient was tachycardic and hypotensive on admission. Elevated levels of total leucocyte count (14,800/mm3) were observed on a hemogram. Other blood tests including liver function tests and renal function tests were within the normal range. She was being treated with antipyretics but without significant symptom relief. X-ray chest revealed widening of the cardiac silhouette without any lung pathology (Figure 1 A).
Figure 1
A – Chest X ray findings suggestive of widening of the cardiac silhouette without any lung pathology; B – CT scan findings of large mediastinal cystic mass, with findings suggestive of a mediastinal dermoid cyst
A 2D echo examination revealed the presence of gross pericardial fluid, with a hyperechoic lesion in the pericardium impinging along the right atrium, with multiple echogenic shadows.
A contrast-enhanced computed tomography scan (CECT) chest revealed an 8.2 × 7.8 × 7.1 cm well-defined fluid density neoformation in the right pericardiac region. Areas of eccentric fat and calcific foci were also observed. There was a focal loss of fat plane with the right atrium, associated with gross pericardial effusion. All the features were suggestive of a dermoid cyst (Figure 1 B).
The patient was stabilised hemodynamically by starting her on inotropes. Under general anaesthesia, the patient was explored. A midline sternotomy was done and a pericardiotomy was done to drain the fluid. The fluid was sent for cytologic examination. The neoformation was in the right pericardiac region and appeared to be originating from the right thymus lobe. It was extra-pericardial in location and had ruptured inside the pericardium. Medially it was abutting the right atrium and laterally the middle lobe of the right lung. It was adherent to the right phrenic nerve posteriorly. The phrenic nerve was dissected cautiously from the cystic lesion using bipolar cautery. The cyst was infected secondarily, as evidenced by the purulent content of the cyst. Complete excision of the cyst was done along with the right lobe of the thymus and part of the adjoining pericardium, sparing the right phrenic nerve.
On gross examination the cyst measured 9.5 cm × 9 cm × 5 cm in size (Figure 2 A). There was evidence of cartilaginous material and hair tufts inside the cyst cavity (Figure 2 B). Histopathology confirmed the diagnosis of a mature cystic teratoma with no immature component. The fluid from the pericardial cavity which was sent for cytologic examination confirmed the presence of pus cells. The patient recovered uneventfully and was discharged on day four.
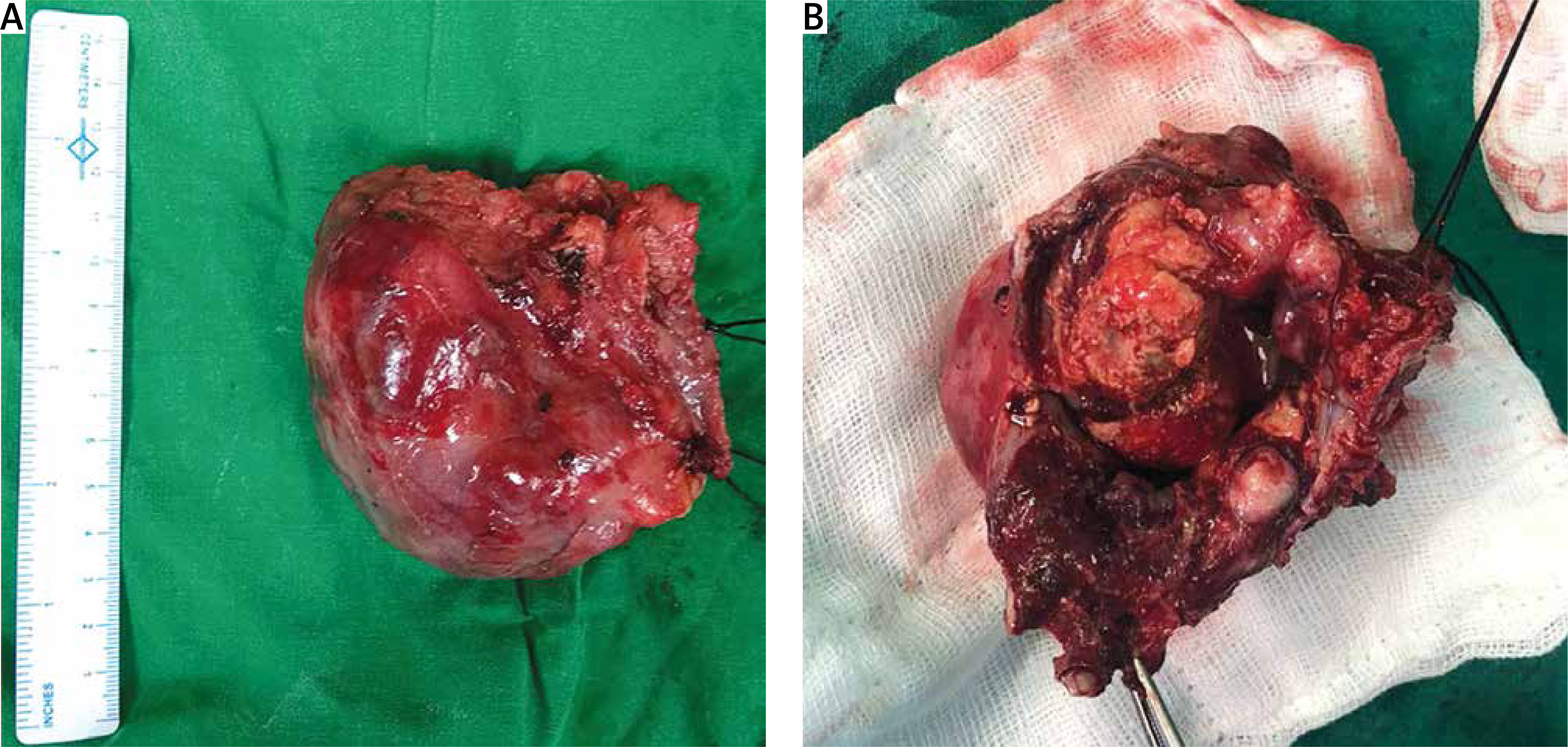
Figure 2
A – Post-excision picture; B – Cartilaginous material and hair tufts inside the cyst cavity
Mediastinal teratomas account for 7–9.3% of mediastinal tumours and 50–70% of all mediastinal germ cell tumours [1]. They are commonly present in the second to third decade.
Dermoid cysts are mostly asymptomatic and are incidentally detected on radiological investigations. When symptomatic there is a wide variety of presentations. They can present with dyspnoea, cough and fever due to compression of the trachea, bronchus or lung [3]. Compression of the superior vena cava and erosion of the bronchus can also occur. Sachdeva and Chawla reported a case of a mediastinal dermoid cyst with bronchial rupture [4]. Pleural effusion can occur due to rupture or secondary infection of the lung following compression. There have been reports of ruptured cystic teratomas resulting in massive pleural effusion. Mature teratoma causing empyema was reported by Raoufi et al. and was secondary to atelectasis of the left lung [5]. Pericardial rupture is very rare for a dermoid cyst. Only 1 case report by Ahmed et al. described a young male patient suffering from chronic pericardial effusion who had a cystic teratoma rupture in the pericardium, where the patient had prolonged symptoms. Our patient, however, had a more acute presentation [6]. In our present case, the young girl presented with cough and fever for 1 week. Teratomas of the mediastinum are more prone to rupture than other sites due to the presence of exocrine pancreatic tissue which causes secretion of proteolytic enzymes in them [1, 2]. We speculate the secondary infection of the cyst to be the probable cause of the rupture of the cyst, which led to an acute presentation in our patient. However, she was found to have a dermoid cyst in the right pericardiac region with gross pericardial effusion on CT. CT is a very helpful diagnostic tool for differentiating mature cystic teratoma from other causes of anterior mediastinal mass such as lymphoma or thymoma. It shows enhancement of the capsule and septa with varying densities due to the presence of bone, soft tissue, fluid, fat, and teeth. The presence of fat and calcification is usually diagnostic of a dermoid cyst [2].
Serum levels of α-fetoproteins and β-HCG are always normal in teratomas [1]. By definition, teratomas are tumours composed of well-differentiated derivations from at least two of the three germ cell layers (ectoderm, mesoderm, and endoderm). Ectodermal elements may be represented by skin, teeth, and hair; mesodermal elements by bone, cartilage, and muscle; and endodermal elements by bronchial and gastrointestinal epithelium and pancreatic tissue [1].
Complete surgical excision is curative and the treatment of choice. These tumours may pose difficulties in surgery due to the close proximity of lung, vascular structures and pericardium [2]. In our case, the tumour was adherent to the right phrenic nerve but was spared by careful surgical dissection.
Teratoma is a rare neoplasm in the mediastinum, with rupture in the pericardium even rarer. They should be suspected in a young patient with non-specific chest complaints and mediastinal widening on X-ray. CT chest is usually diagnostic of a dermoid cyst and tissue biopsy is rarely required. Rupture into the pleura and pericardium can occur and should undergo prompt and early surgery. Complete excision of the tumour is the definitive treatment.









