
Introduction
The presence of hepatitis C virus (HCV) RNA in hepatocytes or peripheral blood mononuclear cells (PBMCs) in the absence of detectable plasma HCV-RNA is defined as occult HCV infection (OCI) and was first described in 2004 [1]. There are two known types of OCI: seronegative OCI (anti-HCV antibody- negative and serum HCV-RNA-negative); seropositive OCI (anti-HCV antibody-positive and serum HCV-RNA-negative) [2]. Egypt has one of the highest global burdens of HCV infections with estimated prevalence ranges from 4.5% to 6.7% [3]. In a recent meta-analysis based on HCV prevalence and genotype studies, HCV genotypes 1 and 3 were found to be the most common causes of HCV infections worldwide (44% and 25% respectively), but in Egypt genotype 4 was the commonest [4].
Chronic HCV and chronic HBV infections are the main causes of end-stage liver disease and hepatocellular carcinoma (HCC) worldwide depending on the population studied [5]. Liver transplantation (LT) is the definitive treatment in patients with advanced liver disease as well as selected patients with HCC. Since Egypt had the highest prevalence of HCV infection worldwide before the advent of direct acting antiviral (DAA) treatment (14.7%), advanced liver disease and HCC secondary to chronic HCV infection were the most common indication of living donor liver transplantation in Egypt [6]. However, HCV recurrence after LT with graft loss was a serious problem in the interferon era because of the poor response rates and tolerability when retreated [7, 8].
With the advent of DAAs, there is emerging research testing their efficacy and safety in this issue. In a study on 79 patients with HCV genotype 1-4 recurrence after liver transplantation, the use of sofosbuvir/velpatasvir for 12 weeks was associated with a 96% cure rate [9]. Sofosbuvir/ledipasvir combination was tested in a larger multicenter study on 204 patients with HCV recurrence after liver transplantation, with SVR of 100% and 96% at 8 and 12 weeks respectively [10]. These results were reproduced in the larger openlabel MAGELLAN-2 trial and the HCV-TARGET study [11, 12]. The aim of the current study was to detect OCI in patients with living donor liver transplantation (LDLT) who achieved SVR after sofosbuvir (400 mg) based antiviral treatment, to detect risk factors associated with the development of OCI, as well as to detect the impact of HCV infection recurrence on both patient and graft during the follow-up period.
Material and methods
Study participants
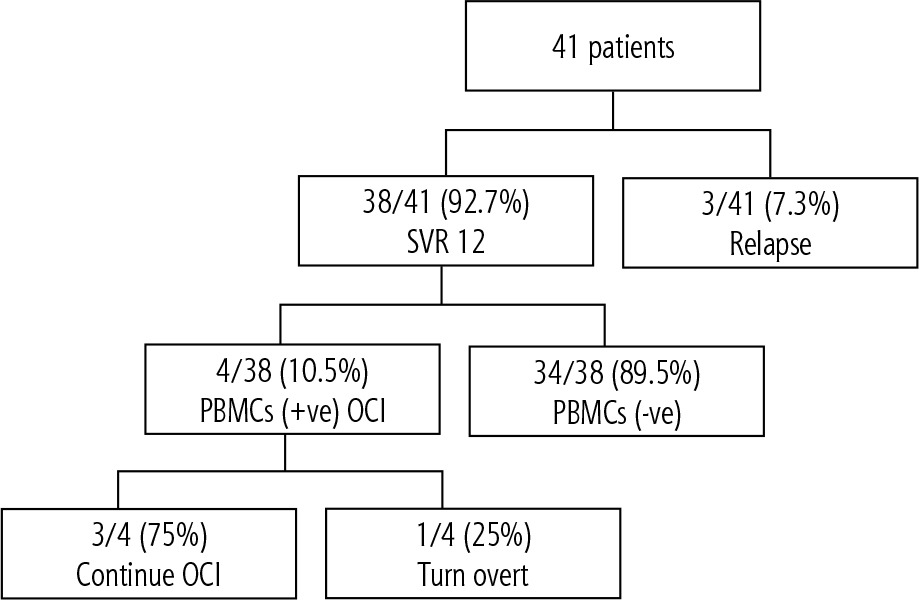
This prospective study was carried out to investigate the frequency of OCI in patients with LDLT and to detect risk factors of recurrence as well as the impact on the patient and graft. The participants were recruited from the liver transplantation unit, Faculty of Medicine, Cairo University in the period from December 2014 to June 2016 with extended follow-up of positive cases to June 2018. The study enrolled 41 patients who had undergone LDLT for HCV related liver disease who did not receive antiviral therapy before LDLT, as shown in Figure 1. The inclusion criteria were recipients of living donor liver transplantation, age > 18 year, patients who achieved and maintained SVR 12 weeks after therapy with sofosbuvir based therapy. The exclusion criteria were co-infection with hepatitis B virus (HBV) or human immunodeficiency virus (HIV), positive serology for cytomegalovirus (CMV) and Epstein-Barr virus (EBV) and LT not related to HCV infection (e.g., Budd-Chiari syndrome, autoimmune hepatitis, primary biliary cirrhosis). The included patients had received sofosbuvir based therapy and had achieved SVR 12 weeks as confirmed by HCV-RNA measurement in their serum. Also, peripheral blood mononuclear cell (PBMC) HCV-RNA content was determined in those patients at 12 weeks after treatment. At follow-up, blood samples were obtained for liver transaminases and HCV-RNA in serum every 6 months to detect any change to overt HCV in patients who were positive for OCI. The primary objective was to determine the frequency of OCI in LDLT patients; meanwhile the secondary objective was to determine the effect of DAAs after transplantation and reflect on patient and graft survival.
Clinical data collection and laboratory methods
Demographic data and patient’s history were taken. Also, data regarding body mass index (BMI), time since liver transplantation, and current immunosuppressive drugs were obtained at enrollment. Abdominal ultrasound was performed after overnight fasting in the supine, right and left lateral positions using a real time scanning device: the Siemens ACUSON S3000 Ultrasound System (Siemens AG, Erlangen, Germany) with convex, 6C1 HD transducer, 1.5-6.0 MHz. Scanning was done through several longitudinal, oblique, and transverse scans to identify liver graft texture, presence of intrahepatic biliary radicle dilatation, peak systolic velocity, and resistance index (RI) of the hepatic artery and the mean portal vein velocity. Measurements were taken in quiet respiration. Assessment of liver fibrosis by transient elastography (TE) using a FibroScan device (Echosens, Paris) was performed to measure liver stiffness (LS). TE was performed with a standard M probe, an XL probe (for obese patients).
Blood samples were drawn for measuring transaminases, alkaline phosphatase (ALP), γ-glutamyl transferase (GGT), total and direct bilirubin, albumin, creatinine, blood urea nitrogen (BUN), complete blood count (CBC), international normalized ratio (INR) and partial thromboplastin time (PTT). Detection of HCV viral load in serum samples was performed by real-time quantitative reverse transcriptase-polymerase chain reaction (qRT-PCR) both initially to document overt HCV infection and during follow-up to detect possible conversion to overt HCV. Additionally, qRT-PCR was used for detection of HCV-RNA in PBMCs of all cases. PBMCs were separated from plasma by density gradient centrifugation and prepared via standard Ficoll Hypaque centrifugation protocols then stored at –80°C until total RNA isolation. HCV-RNA was extracted using an RNeasy Mini Kit (Qiagen, Santa Clarita, USA) then qRT-PCR was performed with the Abbott RealTime HCV assay kit (Abbott Molecular Inc.) according to the manufacturer’s specifications. The assay was performed through real-time PCR fluorescence detection on an ABI PRISM 7500 Real-Time PCR System (Applied Biosystems, Foster City, CA, USA) using fluorescent labeled probes which were used for reverse transcription, PCR amplification, and detection/quantitation. The lower limit of assay detection is 12 IU/ml, with ≥ 95% probability and the dynamic range of the assay extends from 12 to 100,000,000 IU/ml. The test has a precision of ≤ 0.25 log IU/ml SD and 100% specificity.
Statistical analysis
The collected data were tabulated and statistically analyzed using SPSS Statistics software version 25 (IBM, New York, USA). Descriptive statistics were done for parametric quantitative data by mean, standard deviation beside minimum and maximum of the range. The non-parametric quantitative data were presented as median, while they were done for categorical data by number and percentage. Comparisons were done for parametric quantitative data using the paired sample t test, and for non-parametric quantitative data using the Wilcoxon signed rank test. The level of significance was taken as p value < 0.05.
Results
The study enrolled 41 patients with living donor liver transplantation who received different sofosbuvir based regimens for recurrent HCV genotype 4 after liver transplantation with 38 patients out of 41 (92.7%) achieving SVR after 12 weeks of treatment (Fig. 1 shows the flow chart of study design). These 38 patients were studied to detect OCI. The mean age of the patients was 52.4 ±4.9 years; most of them (36 out of 38) were men (94.7%). The average BMI was in the overweight category (29 ±3.2 kg/m2), 12 patients out of 38 were diabetics (31.5%), and 4 out of 38 were hypertensive (10.5%). In 36 patients the cause of liver transplantation was decompensated liver cirrhosis with an average MELD score > 13, and the other 2 patients had hepatocellular carcinoma on top of liver cirrhosis. They received a different sofosbuvir-based regimen as mentioned in Table 1, for 12 weeks in 20 patients (~53%) and for 24 weeks in the other 18 patients (~47%). Adherence to treatment was 100%.
Table 1
Demographic, laboratory, clinical and therapeutic characteristics of the SVR 12 study group
By comparing the liver enzymes, serum albumin and bilirubin in the studied group (38 patients with SVR) before and after treatment with antiviral drugs, there was a significant reduction in total bilirubin (p = 0.04) and ALP (p = 0.04) after treatment, as shown in Table 2.
Table 2
Comparison between liver function test before and after antiviral treatment within the study subjects
At week 12, a blood sample was drawn from the 38 patients who achieved SVR to test for occult HCV-RNA in PBMCs using RT-PCR. Occult HCV was detected in 4 cases out of 38 (10.5%), as shown in Figure 2. These 4 patients were males in the sixth decade. None of them was hypertensive, but one patient was diabetic. 2 patients received sofosbuvir plus ribavirin for 24 weeks, one patient received sofosbuvir (400 mg) plus ribavirin (800 mg) and pegylated interferon for 12 weeks and one patient received sofosbuvir (400 mg) plus daclatasvir 60 mg for 12 weeks. The transient elastography performed after treatment was F1 in one patient and F2 in 2 patients and F3 in one patient. One patient presented high aspartate aminotransferase (AST) and alanine aminotransferase (ALT); however, the other 3 patients had normal enzymes in the post-treatment phase. As regards immunosuppressive medications, one patient received cyclosporin, two patients received tacrolimus plus mycophenolate mofetil (MMF), and one patient received tacrolimus only.
We followed up these 4 patients using AST and ALT in addition to HCV-RNA in serum using PCR every 6 months for about 2 years. Three patients continued to have relatively normal liver enzymes with occasional minimal elevation. Their serum HCV PCR continued to be negative, as shown in Table 3. Only one patient showed progressive elevation of liver enzymes and after 18 months the patient turned HCV PCR positive in serum, as shown in Table 4. This patient was re-treated using sofosbuvir 400 mg and ledipasvir 90 mg daily for 12 weeks and then was tested 12 weeks after treatment with HCV PCR in serum and HCV in PBMCs. Both tests turned out negative, which coincided with normalization of liver enzymes.
Table 3
Follow-up data of occult hepatitis C virus infection patient who developed overt disease
| Parameter | 2016 | 2017 | 2018 | 12 weeks post sofosbuvir + ledipasvir |
|---|---|---|---|---|
| ALT (IU/l) | 45 | 60 | 90 | 35 |
| HCV RNA in serum | Negative | Negative | Positive | Negative |
| HCV RNA in PBMCs | Positive | Positive | Positive | Negative |
Table 4
Data of patient with occult hepatitis C virus (HCV) who developed overt HCV
Discussion
Hepatitis C virus infection is the leading cause of chronic hepatitis, liver cirrhosis and hepatocellular carcinoma worldwide, and is one of the primary indications for liver transplantation [13]. Recently, Egypt launched the largest medical campaign to scan for HCV infection and to treat infected patients with the novel DAAs. Despite the high treatment efficacy with SVR higher than 95% and better tolerability than the interferon-based regimen, there are still unmet needs such as difficult-to-treat populations and emerging underestimated issues including persistent OCI.
Occult hepatitis C virus infection can be present without any evidence of liver disease [14]. OCI can be a potential source of relapse with subsequent graft damage in liver transplanted patients. The clinical significance of occult HCV infection in liver tissues of patients with HCC of negative serology is another concern that had been studied in a retrospective study with OCI detected in 3 patients of 42 (7%). However, the clinical significance of OCI in HCC needs further research [15].
In our study, 38 patients out of 41 patients achieved SVR at 12 weeks (92.7%) and OCI was detected in 4 patients (10.5%). Our results are in accordance with a previous study that included 998 naïve chronic HCV infected patients who achieved 24-week SVR, of whom 74 had persistent elevation of transaminases compared to another age- and sex-matched group with normal transaminases. OCI was detected in 14 patients out of 74 (18.9%) with elevated transaminases and 4 patients out of 67 (5.9%) with normal transaminases [16]. In another cross sectional multicenter study that enrolled 1280 treated HCV patients who achieved SVR 12 weeks after treatment, HCV-RNA was found in PBMCs of 50 (3.9%) of them [17]. This relatively low prevalence in the previous two studies could be attributed to the search for OCI in all the patients who achieved SVR 24 with normal or elevated enzymes. However, in a more recent prospective study that included patients with recurrent HCV infection following liver transplantation, a higher incidence was noted with 5 patients out of 9 having OCI (55%). The higher incidence in this study was attributed to selection of patients with only elevated transaminases [18]. In the general population, the prevalence of OCI is around 3.3%, but this percentage increases after treatment or spontaneous clearance of HCV infection, with much higher prevalence reaching up to 57% in cases of elevated liver enzymes [1, 19].
In the current study, the four patients who were detected to have OCI were males in the sixth decade of life, not hypertensive, but one of them was diabetic with grade F1, F2 and F3 on FibroScan and with high BMI. Thus, we suggest that diabetes mellitus does not represent a risk factor for OCI, but obesity and cirrhosis were associated with increased risk of OCI. This is in accordance with the work of Mohamed et al., who found no significant difference between the occurrence of OCI and the presence or absence of diabetes mellitus or obesity. They attributed the effect of obesity to its association with hepatic steatosis, which could lead to hepatic inflammation and fibrosis progression [16].
Our study showed that 3 patients with OCI received the initial sofosbuvir based regimens, either sofosbuvir plus ribavirin for 24 weeks or sofosbuvir plus ribavirin and interferon α2a for 12 weeks; hence, we suggest that these regimens could have lower efficacy than other DAA regimens. However, we cannot confirm this as these are just 4 case reports. As regard immunosuppressive drugs, one patient received a single drug (cyclosporin), second patient received tacrolimus and the other two patients received dual therapy (tacrolimus + mycophenolic acid), so the number or type of immunosuppressive medications does not contribute to the OCI occurrence. A case report of three cases with OCI and kidney transplantation showed that there was no association between OCI and type or dose of immunosuppressant drugs [20].
During follow-up, only one of the four OCI patients developed overt HCV. This patient was not diabetic or hypertensive, but his liver enzymes were elevated from the start of the study; however, he was obese with high BMI and F3 fibrosis (Table 3). These data may suggest that the association of OCI with advanced degrees of fibrosis or higher BMI may cause nonalcoholic steatohepatitis (NASH), which predisposes to deterioration or occurrence of OCI or even its change to overt HCV. This in accordance with an older study that found that one of three patients with OCI developed overt HCV with a low level of viremia [17]. Also in another study, Hanno and his colleagues found that patients with OCI had an overall significantly higher relapse rate up to 50% after two years [21]. One of the patients in this case series presented with progressive elevation in the level of liver enzymes, suggesting that OCI may be accompanied with persistent liver injury and damage. Paired liver biopsies at baseline and SVR 24 were analyzed in a recent study which recruited 140 patients from 3 hospitals who had achieved serum HCV, finding that OCI was associated with increasing fibrosis and active inflammation [22]. Patients with liver transplantation with OCI represent a special group with high risk for graft damage. Hence, we treated the patient who developed overt HCV using sofosbuvir (400 mg) and ledipasvir (90 mg) daily for 12 weeks. This treatment was accompanied with normalization of the liver enzymes and clearance of HCV from serum and PBMCs after 12 weeks of treatment (Table 4).
Conclusions
Occult hepatitis C virus infection could represent a potential source of HCV relapse. Although it is infrequent, it could explain raised transaminases after SVR, although OCI could be detected in patients with normal liver enzymes. Patients with liver transplantation represent a high-risk group, so to avoid relapse and graft damage, we recommend screening for OCI in PBMCs or liver biopsy in these patients. Further studies with a larger number of patients and prolonged periods of follow-up will be needed for a better understanding of the natural course of OCI and identification of its risk factors. A scoring system for prediction of OCI and relapse in liver transplantation may be needed to select patients for screening.





