
Introduction
Bullous pemphigoid (BP) is the most common autoimmune blistering disease, primarily affecting elderly patients. It is characterized by pruritic, urticarial plaques and tense bullae [1]. Systemic and topical corticosteroids are considered the first-line treatment for BP [2].
Recently there has been a growing interest in alternative treatments for BP to reduce the adverse effects of systemic steroid and classical immunosuppressive therapies [2, 3]. European guidelines published in 2022 recommended omalizumab as a preferable option in corticosteroid-dependent and recurrent BP patients with poor general condition and/or contraindications to immunosuppressive therapies [4]. The involvement of immunoglobulin E (IgE) antibodies in the pathogenesis of BP has been demonstrated. Rates of anti-BP180 IgE autoantibody positivity in BP patients range from 22% to 100% with the use of different tests. This suggests that omalizumab, an anti-IgE monoclonal antibody, may offer therapeutic benefits in BP [5].
Aim
As omalizumab is not immunosuppressive and has a favourable side effect profile, the aim of this study was to examine its clinical effectiveness in the treatment of BP in older adults, adults, a patient group that typically has multiple comorbidities and use multiple medications.
Material and methods
Study groups
We retrospectively reviewed the medical records of 46 patients diagnosed with BP who received omalizumab for at least 6 months between January 2018 and December 2024. Clinical information and laboratory results were retrieved from patients’ medical charts. The diagnosis of BP was established based on clinical examination findings and the criteria proposed in the European guidelines [4]. Patients meeting the following criteria were included in the study: 1) histopathological confirmation of the diagnosis, 2) positive direct immunofluorescence findings, and 3) enzyme-linked immunosorbent assay detection of autoantibodies against BP180 and/or BP230.
Treatment protocol
Patients diagnosed with BP were first treated with topical clobetasol 17-propionate ointment (25–50 g/day) for 1 month. For patients with a Bullous Pemphigoid Disease Area Index (BPDAI) score below 20 at the end of this period, combined topical steroid and omalizumab treatment was initiated.
Patients whose BPDAI score remained 20 or higher during topical steroid treatment received omalizumab with additional systemic steroid treatment. For patients who developed adverse effects during systemic steroid treatment and/or whose BPDAI did not decrease during follow-up, azathioprine, mycophenolate mofetil, dapsone, rituximab, and/or intravenous immunoglobulin treatment were added to treatment. Patients who started systemic steroid therapy were followed up every 15 days in consideration of their comorbidities. The dose of systemic steroid was reduced by 25% every 15 days.
Omalizumab was administered as a single subcutaneous dose of 300 mg every 4 weeks in accordance with the chronic idiopathic urticaria protocol [6]. To evaluate treatment effectiveness and classify treatment response, the following parameters were evaluated at initial presentation, before omalizumab initiation, and after 1, 3, and 6 months of omalizumab treatment: Bullous Pemphigoid Disease Area Index (BPDAI) score [7], Pruritus Visual Analogue Scale (PVAS) [8, 9], treatment response scale (complete response [CR], partial response [PR], no significant clinical improvement [treatment inefficiency], recurrence), eosinophil count, serum total IgE level, D-dimer value, and C-reactive protein [4].
Patients were also evaluated for adverse effects during omalizumab treatment. Injection site reactions, thrombocytopenia, persistence of itching, and exacerbation of BP lesions potentially associated with omalizumab treatment were assessed at 1, 3, and 6 months of treatment.
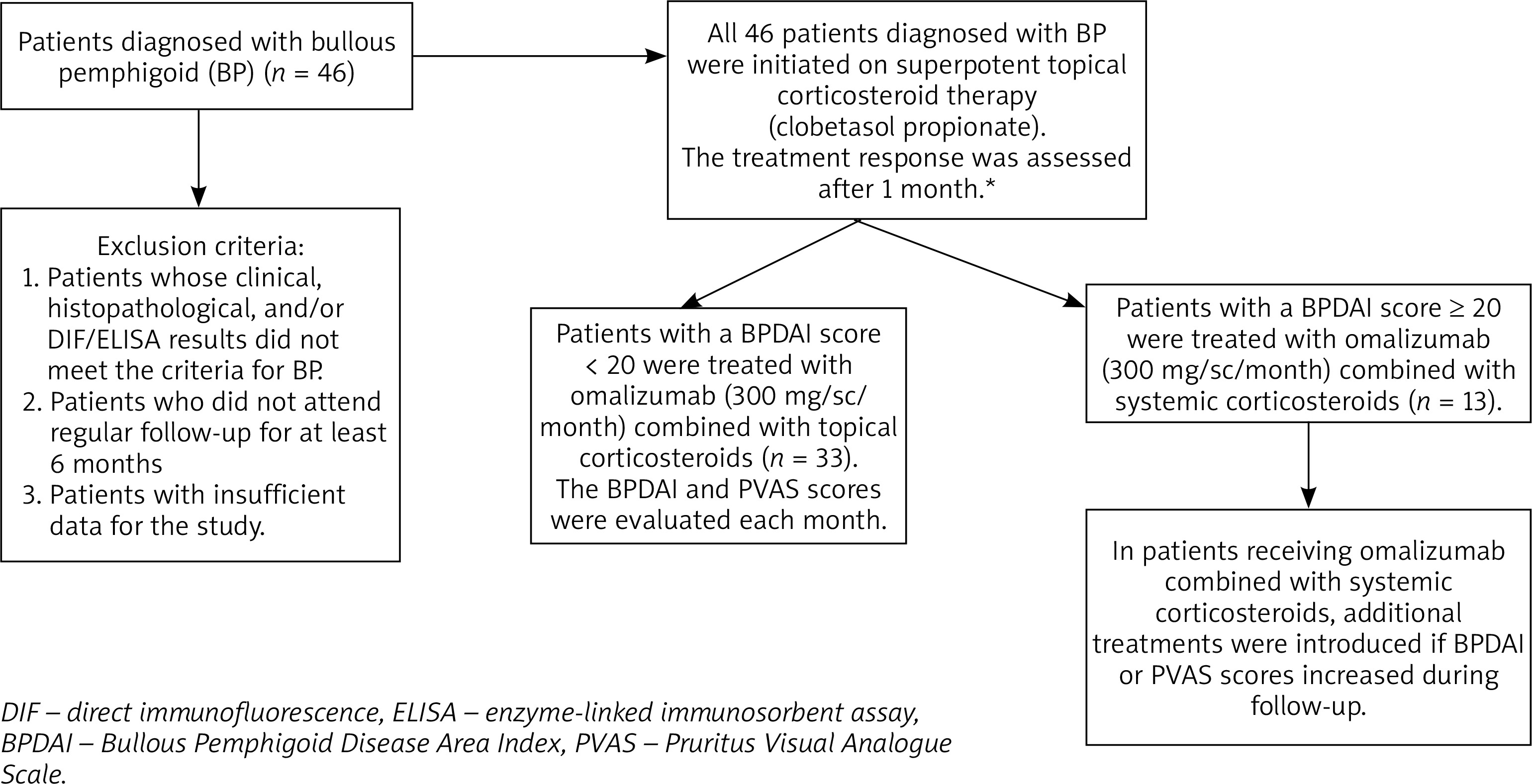
The study protocol is detailed in the flowchart (Figure 1). Permission to conduct the study was obtained from the Ethics Committee of Trakya University (2025/142). Approval was obtained for the off-label use of omalizumab, mycophenolate mofetil, rituximab, and intravenous immunoglobulin therapy. All patients’ follow-up and treatment were carried out by a single dermatologist (Y.G.U.) experienced in autoimmune diseases.
Figure 1
Flowchart illustrating the selection of the study sample (n = 46). *For patients with a BPDAI score ≥ 20 at baseline, treatment was administered in the hospital setting with preparations for potential immunosuppressive therapy. For patients with persistently elevated BPDAI scores, omalizumab combined with systemic corticosteroids was initiated earlier (before completion of the first month)
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics software (version 26.0; IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) and range, whereas categorical variables were presented as numbers and percentages. The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. For comparisons between independent groups (Complete Response vs. Non-complete Response), the Mann-Whitney U test was used for continuous variables, and Pearson’s χ2 or Fisher’s exact test were used for categorical variables, depending on the sample size in the cells. To analyze changes in laboratory parameters (eosinophil count, total IgE, and D-dimer) across multiple time points (baseline, 1st, 3rd, and 6th months), the Friedman test was utilized. Pairwise comparisons between time points were conducted using the Wilcoxon signed-rank test with appropriate adjustment for multiple comparisons.
All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
Results
Among the 46 patients, 45.7% were male. The mean age at diagnosis was 79.6 years. Clinically, the most commonly affected areas were the upper and lower extremities (93.5%, n = 43). The most frequent comorbidities were hypertension (73.9%, n = 34) and type 2 diabetes mellitus (DM) (45.7%, n = 21) (Table 1). Among the triggering factors of bullous pemphigoid lesions, medication use was the most prominent, observed in 94% (n = 32) of cases. The most common triggering drugs were gliptins (n = 16) and hydrochlorothiazide (n = 8) (Supplementary Figure S1).
Table 1
Sociodemographic and clinical characteristics of the patients (n = 46)
| Parameter | Results |
|---|---|
| Gender, n (%) | |
| Male | 21 (45.7) |
| Female | 25 (54.3) |
| Age [years] mean (range) | 76 (54–94) |
| Disease duration [months] mean (range) | 1 (1–12) |
| Lesion location, n (%) | |
| Upper/lower extremities | 43 (93.5) |
| Trunk | 36 (78.3) |
| Oral mucosa | 16 (34.8) |
| Scalp | 6 (13) |
| Comorbidities, n (%) | |
| Hypertension | 34 (73.9) |
| Diabetes mellitus | 21 (45.7) |
| Coronary artery disease | 20 (43.5) |
| Neurological disease* | 13 (28.3) |
| Hyperlipidaemia | 11 (23.9) |
| History of hepatitis B** | 10 (21.7) |
| Chronic kidney disease | 6 (13.0) |
| COPD | 6 (13.0) |
| Malignancy | 2 (4.3) |
| History of hepatitis C*** | 2 (4.3) |
| Clinical presentation, n (%) | |
| Bullae at diagnosis | 42 (91.3) |
| Severe urticarial lesions | 19 (41.3) |
| Eczematous lesions | 18 (39.1) |
Among the patients, 71.7% (n = 33) did not require any treatment other than omalizumab with topical corticosteroid. Thirteen (28.3%) patients required adjunctive systemic treatment in addition to omalizumab. Systemic steroids were the most commonly used treatment in patients in addition to omalizumab (28.2%, n = 13). Among patients who did not respond to omalizumab and systemic steroid therapy, 3 (6.5%) patients received azathioprine and 2 (4.4%) patients received dapsone as additional treatments. Details of the treatments administered are presented in Table 2.
Table 2
Distribution of treatment received by patients with bullous pemphigoid (n = 46)
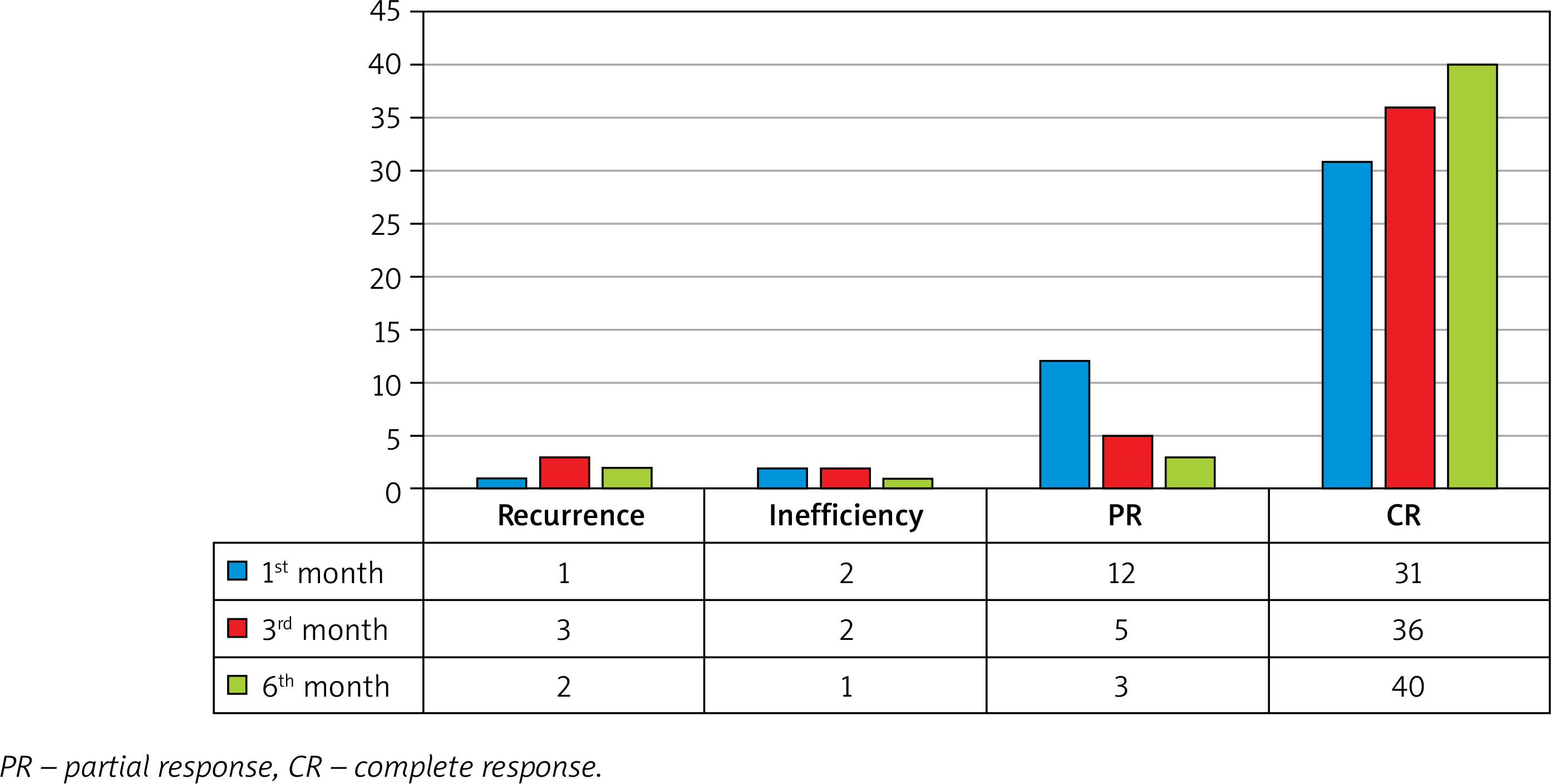
The average BPDAI before omalizumab treatment was 18 (range: 3–51), and the average PVAS was 9 (range: 0–10). Within the first month of treatment, 67.4% of the patients showed a CR to treatment (n = 31). This rate increased to 87% (n = 40) by the sixth month (Figure 2).
Figure 2
Evaluation of the effectiveness of omalizumab treatment after the first, third, and sixth month of treatment
Comparative analysis between patients who did and did not achieve a CR to treatment indicated that patients without CR had a higher mean age (p = 0.030) when compared with patients who did achieve a CR (Table 3).
Table 3
Comparison of the characteristics of patients with and without a complete response after the first month of omalizumab treatment
| Parameter | Clinical response to omalizumab treatment at month 1 | ||
|---|---|---|---|
| Complete response (n = 31) | Non-complete response (n = 15) | P-value* | |
| Gender | |||
| Male | 14 (45.2) | 7 (46.7) | 0.923 |
| Female | 17 (54.8) | 8 (53.3) | |
| Age [years] | 73.94 ±8.4 (54–91) | 80.27 ±8.93 (66–94) | 0.030 |
| Disease duration | |||
| > 1 month | 11 (35.5) | 9 (60) | 0.116 |
| ≤ 1 month | 20 (64.5) | 6 (40) | |
| Mucosal involvement | 10 (32.3) | 6 (40) | 0.605 |
| Accompanying comorbidities | |||
| ≥ 2 | 23 (74.2) | 8 (53.3) | 0.191 |
| 0–1 | 8 (25.8) | 7 (46.7) | |
| Eosinophil count [103/µl] | 553.16 ±719.4 (10–3300) | 507.33 ±471.43 (30–1700) | 0.574 |
| Eosinophil/lymphocyte ratio | 0.43 ±0.99 (0.01–5.5) | 0.37 ±0.45 (0.02–1.41) | 0.647 |
| Total IgE [IU/l] | 889.42 ±978.36 (5–2500) | 948.33 ±824.36 (102–2500) | 0.241 |
| D-dimer [mg/l] | 3.35 ±3.86 (0.24–13.4) | 3 ±3.73 (0.4–11.6) | 0.963 |
| C-reactive protein [mg/l] | 24.97 ±44.63 (0.2–152) | 11.29 ±9.33 (1–27) | 0.664 |
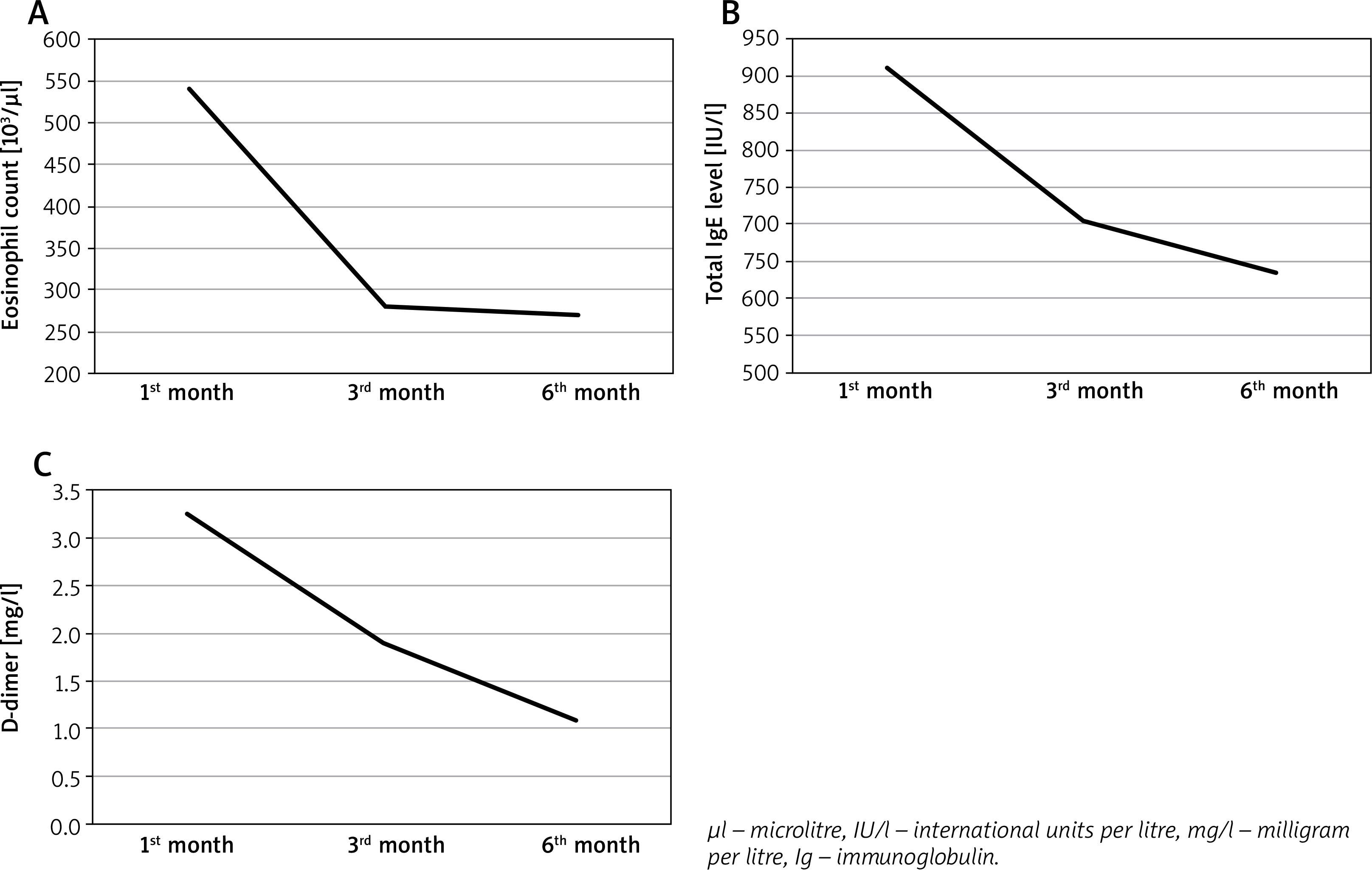
Statistically significant decreases in eosinophil count, total IgE, and D-dimer levels were observed at 1, 3, and 6 months after the initiation of omalizumab (Figure 3, Supplementary Table S1). When compared among the time points, the decrease in eosinophil count was most significant at 6 months (p = 0.001) while the decrease in total IgE was most significant at 3 months (p = 0.001) (Supplementary Table S2).
None of the patients who received systemic treatment developed adverse effects.
Discussion
Diagnoses of BP have increased in recent years as a result of advances in diagnostics, as well as population aging and the subsequent increases in many age-associated diseases [10]. The literature indicates that the overall prevalence of BP is higher in women compared to men. However, the prevalence of BP is higher in men after the age of 70 [11]. In our study, the female-to-male ratio was 1.2 : 1. This relatively balanced sex ratio may be related to the average age of 76 years in our patients.
Patients with BP have many comorbidities associated with advancing age, most frequently cardiovascular and neurological diseases, type 2 DM, and venous thromboembolism [12, 13], and most patients receive pharmaceutical treatment for these conditions. Although many drugs can trigger BP, the most common triggers are dipeptidyl peptidase 4 inhibitors (gliptins) [13]. Recently, immune checkpoint inhibitors and aetiology have also been implicated [14]. In the present study, gliptins were the most frequently implicated drug category among our patients. One of our patients developed BP while receiving cemiplimab for lung adenocarcinoma and achieved CR with omalizumab treatment.
In a 2023 article, the CR rate in BP patients treated with omalizumab was reported as 59.5%. An increase in the CR rate to 81% was observed when patients received more than 10 doses of omalizumab; nevertheless, the difference did not reach statistical significance [15]. We observed an increase in the CR rate with longer duration of use, suggesting that the effectiveness of omalizumab treatment may be higher over a longer period.
Omalizumab treatment in BP patients can be used in combination with other agents [16, 17]. Kwon et al. found that patients who received combined rituximab and omalizumab had a shorter time to disease control with minimum treatment than patients who used rituximab alone [17]. In our data, approximately 28% of patients with BP required other systemic treatments in combination with omalizumab, and 87% of those patients exhibited CR by 6 months of follow-up. Based on these results, omalizumab seems to be a suitable agent for combination therapy.
In the BPDAI scoring system used to determine disease severity in pemphigoid diseases, a score of 15 or higher for patients presenting with erosion/blisters and a score of 20 or higher for patients with urticarial/erythematous lesions indicates moderate disease, and scores of 35 and above indicate severe disease in both clinical pictures [18]. In addition to determining disease severity, the BPDAI is used in treatment follow-up [19]. Few studies have compared changes in BPDAI scores during omalizumab treatment. In one study, the average BPDAI score before omalizumab treatment was reported as 56, while this value was 80.8 in another study [6, 16]. Alexandre et al. observed a rapid response in BPDAI scores after omalizumab treatment, with 6 of 15 patients needing no immunosuppressive treatment [16]. Although the average total BPDAI score was lower in our study, a detailed evaluation of the patients’ initial BPDAI score distribution shows that 6 patients had severe disease, while the others were in the mild and moderate groups. These 6 patients did not achieve CR despite the combination of other treatments with omalizumab. Taken together, these findings suggest that omalizumab treatment can be used alone or in combination with other treatments in patients with mild to moderate BP. It can also be concluded that patients with severe BP are resistant not only to omalizumab but also to other treatments.
Our evaluation of the characteristics of the BP patients who achieved CR with omalizumab treatment indicated that urticarial lesions, blood total IgE concentration, and eosinophil count were not predictive of CR [2, 20]. Similar to the literature, these factors had no impact on good response to omalizumab in our study. Only older age at disease onset was found to be associated with nonresponse to treatment. This indicates that treatment may be more difficult in older adults with BP, possibly due to the increased comorbidity burden.
Oral mucosal involvement varies between 10% and 20% in patients with BP [13]. In one study, it was reported that total BPDAI scores were higher in patients with BP presenting with oral mucosal involvement [21]. Although the prevalence of oral mucosal involvement was higher in our patients than in the literature, there was no difference between patients with and without CR to omalizumab treatment in terms of oral mucosal involvement. This suggests that oral mucosal involvement may not affect response to omalizumab.
The pathogenesis of BP is thought to be associated with type 2 immunity [22, 23]. This is supported by the IgE and eosinophil levels in the peripheral blood and skin lesions of patients with BP. Th2 pathways are considered primary triggers of antibody production in BP [24].
Type 2 proinflammatory cytokines interleukin (IL)-4 and IL-13 play a key role in the pathogenesis of BP [25]. Dupilumab, a monoclonal antibody that blocks the IL-4 receptor α, downregulates the Th2-associated signalling pathway [26]. In recent years, the use of dupilumab in BP treatment has increased [27]. Based on the results of clinical phase studies, the FDA has granted dupilumab accelerated approval for the treatment of bullous pemphigoid [28]. In a review published in 2024, the CR rate was reported as 70.39% among BP patients treated with dupilumab, while the CR rate in patients receiving omalizumab was 76.13%. Both agents were reported to have similar adverse effect profiles [29]. In a comparative study published in 2025 on biologic therapies for BP, dupilumab demonstrated superior outcomes compared with omalizumab. Disease control was achieved in 90.6% and complete remission in 87.1% of patients treated with dupilumab, with lower relapse (10.3%) and treatment discontinuation rates (15.6%) [27]. Although current literature supports the use of omalizumab and dupilumab in the treatment of BP, further studies are needed to better evaluate the efficacy of both agents.
There are different results in the literature regarding the change in eosinophilia and total IgE levels in patients with BP after omalizumab treatment [5, 6, 30]. Similar to our study, D’Aguanno et al. observed decreases in eosinophilia and total IgE after omalizumab treatment [30]. Eosinophilia and total IgE levels may be important in treatment selection and the follow-up of treatment response in patients with BP. However, high levels are not associated with a better clinical response.
Elevated IgE levels are associated with the activation of mast cells, basophils, and eosinophils. Increased eosinophil counts may contribute to vascular wall damage and chronic inflammation, which in turn can activate the coagulation system and lead to elevated levels of D-dimer, a fibrin degradation product [22, 31]. As expected, in our study there was a reduction in D-dimer levels after omalizumab treatment. More comprehensive studies also including a control group are needed to confirm these findings.
Conclusions
The results of this study show that patients with BP can safely use omalizumab as monotherapy or part of combination treatment, and longer duration of use increases the CR rate. Of note, omalizumab alone can be insufficient in the minority of BP patients. Omalizumab may be preferred in patients with high BPDAI scores (moderate or severe disease). Clinical features, total IgE level, and eosinophil level were not predictors of patients’ response to omalizumab treatment. However, reductions in eosinophil, total IgE, and D-dimer levels were observed after omalizumab treatment.
Limitations of the study include its retrospective design, the relatively small sample, lack of control group, and not assessing BP180 and BP230 autoantibodies during treatment follow-up.







