
Purpose
Management of esophageal cancer still is a challenge for contemporary medicine. In 2018 about 572 thousand people were diagnosed with this cancer worldwide, of whom over 508 thousand died [1]. In 2016 in Poland, over 1400 people contracted esophageal cancer, and over 1500 died [2]. Unfortunately, despite the progress in availability and quality of diagnostics very often only palliative treatment can be offered to these patients as they mostly present with distant metastases at diagnosis and dysphagia-related progressive cachexia. Dysphagia is the first symptom of the disease, which causes that the patient decides to visit the doctor. Palliation of dysphagia may be achieved with stenting, laser, mechanical dilatation, photodynamic therapy (PDT), external beam radiotherapy (EBRT) or brachytherapy (BT). Currently, the most commonly used methods are stenting and radiotherapy [3,4,5]. Quality of life improvement is one of the main goals of palliative treatment, which brachytherapy, as one of the radiotherapeutic methods, seems to fit perfectly. The randomized clinical trial SiREC revealed comparable dysphagia reduction one month after BT with 1 × 12 Gy in 73% of patients and 76% of patients after stenting (p = 0.61) [6]. Although prosthetics offer a faster release of dysphagia in 2 weeks, after 6 weeks dysphagia relief was significantly more pronounced after BT [6]. Also, the authors found in the cohort that patients treated with BT reported better quality of life and had lower incidence of treatment sequelae (21% vs. 33%; p = 0.02) [6,7]. Palliative treatment would be even more effective if it were related to more prolonged survival in good comfort or patients requiring different management to provide it could be identified. The purpose of this study was to assess dysphagia reduction in esophageal cancer patients treated with 2D BT and the treatment response influence on their overall survival.
Material and methods
In retrospective research, 133 consecutive esophageal cancer patients’ medical records were analyzed. All patients were not amenable to curative treatment and were palliated with intraluminal high-dose-rate (HDR) brachytherapy in a regional cancer center from October 2010 to December 2016. Forty patients were excluded from the analysis due to lack of data (dysphagia was not assessed before or after treatment), previous treatment with EBRT or a metal prosthesis. Finally, 16 women and 77 men were included in the statistical analysis, together 93 patients with the median age of 65 years (range 45-88 years). The pathological report confirmed squamous cell carcinoma (SCC) in 64.5% of cases, adenocarcinoma (AC) in 20.4%, other types in 6.5% and in 8.6% pathological report information could not be obtained. In all patients, despite possessing additional diagnostic images, cancerous invasion length was measured by the dynamic esophageal X-ray with oral barium contrast, which was used to mark the proximal beginning of the infiltration in relation to the bifurcation of the trachea. All grades of dysphagia were treated because the accessibility to BT and EBRT is not sufficient in our country. The treatment was prescribed to reduce symptoms or to maintain the low grade for a longer time.
The mean tumor length was 81 mm (median 72.5 mm; range 50-200 mm). The tumors were located in the cervical, upper thoracic, and lower thoracic part of the esophagus and in the gastro-esophageal junction (GEJ) in 4.3%, 16.1%, 65.6% and 13.9% of cases, respectively. The clinical stage could be reliably assessed in 59 patients and was stage IV in 47.4%, stage III in 39%, stage II in 10.2% and stage I in 3.4%, as shown in Table 1.
Table 1
Patient characteristics
Treatment
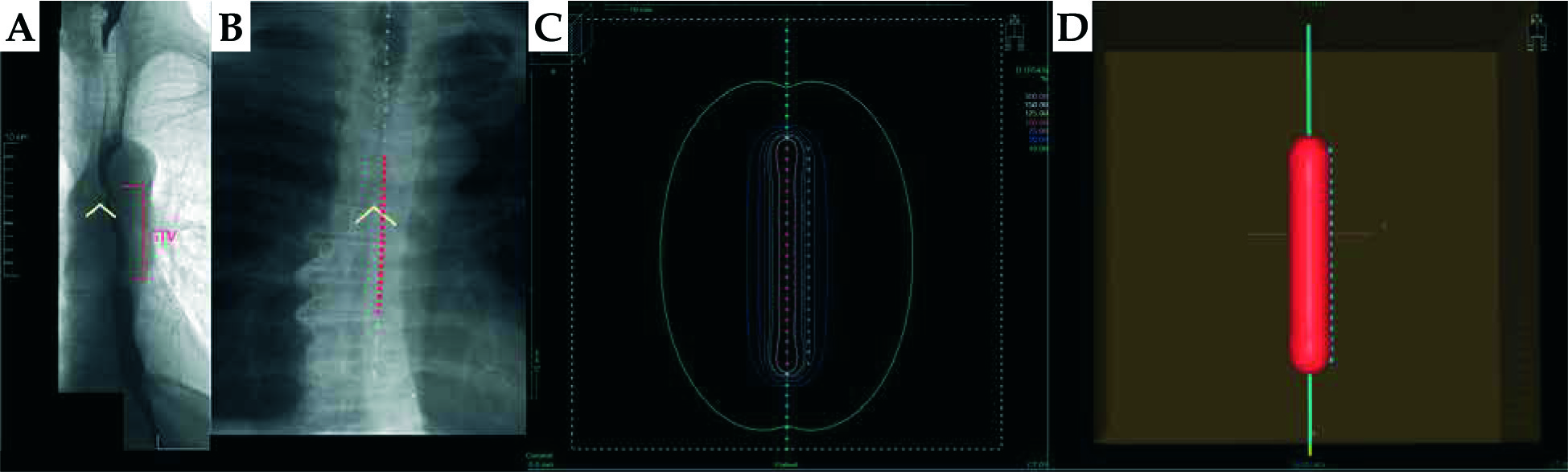
Outpatient treatment was carried out using a micro-Selectron HDR-BT unit (Nucletron/Elekta Company, Stockholm, Sweden) equipped with an iridium-192 (192Ir) radioactive source characterized by average radiation energy of 0.38 MeV and nominal activity around of 370 GBq (reference air kerma rate 41 mGy/h). The procedure started with local anesthesia of the throat (10% xylocaine), then with the help of a cooperating patient an esophageal applicator covered with gel (1% lignocaine) was introduced under the control of sight through the patient’s mouth to the esophagus. Flexible esophageal 4-8 mm wide tubes were used (Nucletron/Elekta Company, Stockholm, Sweden). Most often, the 6 mm one was used depending on the severity of the dysphagia, previous results of X-ray with barium contrast and patient’s compliance during the procedure. Subsequently, an X-ray image was taken (70-80 kV, 2.74-2.81 mA, Endura, Philips, Amsterdam, the Netherlands). The treated length was marked on the X-ray images by analysis of applicator position relative to the tracheal bifurcation and was a sum of the previously measured length of tumorous infiltration plus a 2 cm margin proximally and distally. The planning process was performed without computed tomography imaging. The reference dose was specified to 1 cm from the source axis independently from the applicator size (Figure 1) [8]. Then a two-dimensional (2D) treatment plan was prepared in the Plato system (Nucletron/Elekta, Stockholm, Sweden). The total time of the whole procedure including irradiation took from 30 to 45 minutes.
Fig. 1
The process of treatment planning of 2D HDR brachytherapy. A) Fluoroscopy image with contrast of the patient with 7 cm long lesion, whose cranial edge was localized 2 cm above the carina (white lines). B) Applicator was inserted 4 cm beyond tumor in the esophagus. The patient was irradiated with 2 cm proximal and distal margin. Red dots present the active dwell positions; white lines mark the carina. C) The applicator reconstruction in treatment planning system with dwell positions (pink – active, green – inactive). The treatment planning was performed with a 5 mm source step, and the dose was prescribed on dose points (blue crosses) calculated 10 mm laterally from the axis of the applicator. D) 3D reconstruction of the applicator (blue line) with 100% isodose (red structure) and axis dose points (blue dots)
Eighty-three patients were administered the dose of 22.5 Gy in 3 weekly fractions. Six patients received 15 Gy in 2 fractions, and 3 patients finished their treatment with one dose of 7.5 Gy due to severe early toxicity, complications, and dysphagia intensification during the treatment. One last patient received 30 Gy in 4 fractions. Nineteen patients were also treated with chemotherapy before or after BT.
Follow-up
The first control visit was carried out one month after the treatment completion and the next visits every 1-2 months, depending on the patients’ overall health status. During each visit, the history check and physical examination were performed along with the control esophageal contrast X-ray to assess the tumor remission and rule out the presence of a fistula. Other additional diagnostic examinations were ordered on occasional indications. Dysphagia was evaluated on a 5-grade scale: grade 0 (ability to eat regular diet), grade I (ability to eat some solid foods), grade II (ability to eat semisolid food), grade III (ability to swallow liquids), grade IV (complete obstruction) [9].
Statistical analysis
All data were gathered in the MS Excel spreadsheet, and descriptive statistics were developed. Then data were imported to the program Statistica 12 (StatSoft Inc.). To assess the differences regarding dysphagia the Wilcoxon test was used for related variables on an ordinal scale. For overall survival assessment in the investigated group of patients and subgroups Kaplan-Meier’s curves were used, then to find differences between the curves log-rank and chi-square tests were applied. Patients’ vital status was verified by the regional cancer registry. The logistic regression model was chosen to check the influence of particular factors on dysphagia improvement or worsening after the treatment. A p-value < 0.05 was considered statistically significant.
Results
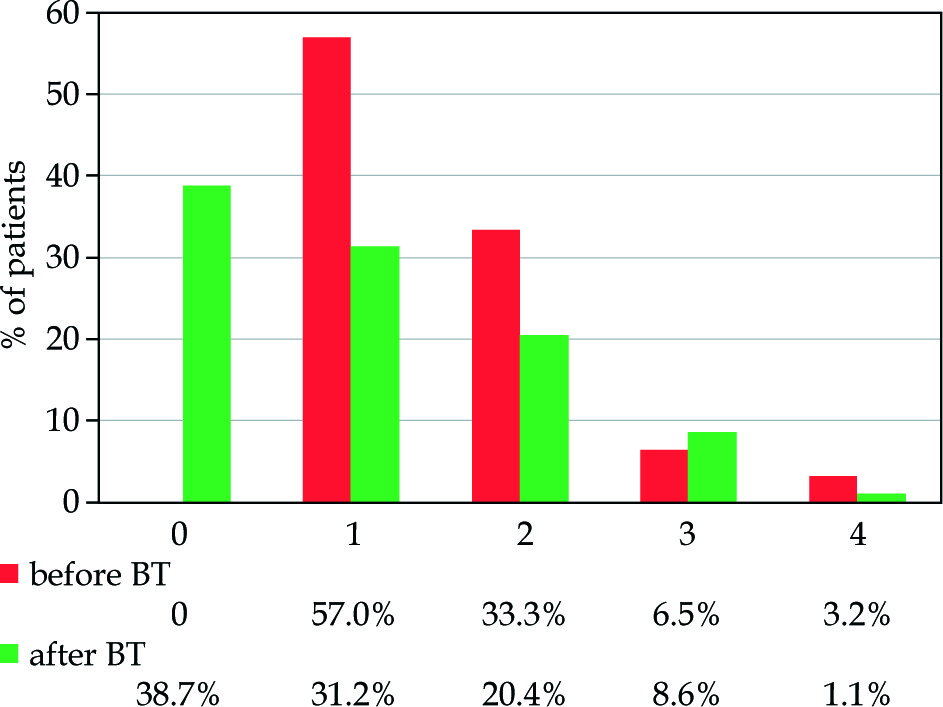
The median overall survival (OS) of all our patients was 5.0 months (range 1.0-43.6 months). Before the treatment patients presented the following grades of dysphagia: 0 – 0%, I – 57%, II – 33.3%, III – 6.5%, IV – 3.2%. Total or partial dysphagia relief after BT was achieved in 55% of patients. The mean duration of improvement was 4.6 months (range 0.6-34.0 months). Stabilization of the symptoms was achieved in 31% of patients and progression in 14%. Of note, the degree of dysphagia relief (grade 0 – 38.7%, I – 31.2%, II – 20.4%, IV – 1.1%) reached statistical significance (p < 0.001; Figure 2).
Fig. 2
The grade of dysphagia in patients with esophageal cancer before and after brachytherapy (BT). The dysphagia grade was significantly reduced after BT (Wilcoxon test p < 0.001)
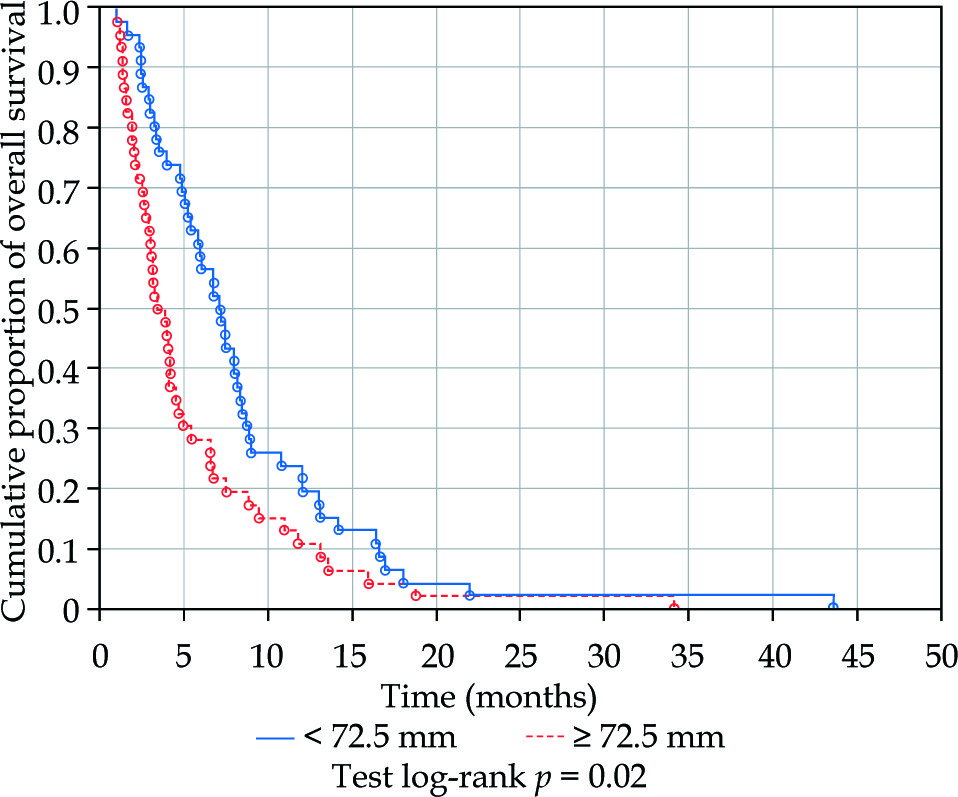
Patients with complete or partial response to the treatment lived longer than patients with stabilization or progression (5.8 vs. 4.1 months; p = 0.02; Figure 3). Patients suffering from adenocarcinoma type lived longer than those with squamous cell carcinoma (8.0 vs. 4.1 months; p = 0.01; Figure 4). Patients in whom cancer infiltration was longer than 72.5 mm on contrast X-ray lived shorter than those in whom infiltration was less (median 7.1 vs. 3.6 months; p = 0.02; Figure 5).
Fig. 3
Kaplan-Meier graph presenting the cumulative proportion of overall survival in patients with esophageal cancer with complete (CR) or partial response (PR) and stabilization (SD) or progression (PD) of grade of dysphagia after brachytherapy (BT)
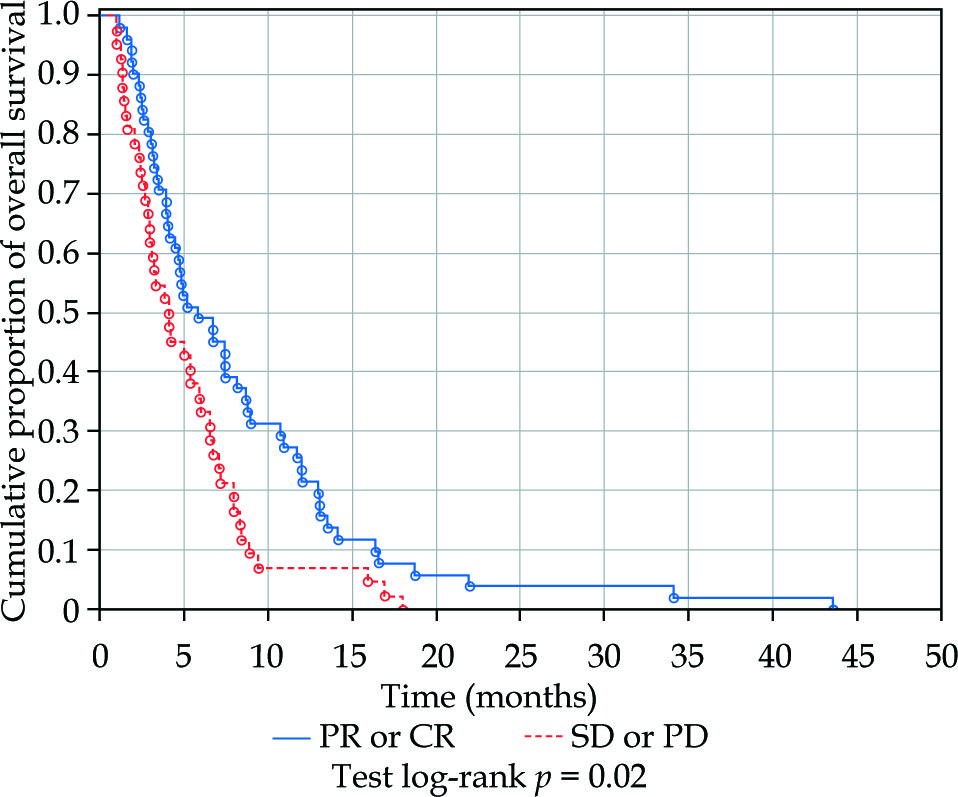
Fig. 4
Kaplan-Meier graph presenting the cumulative proportion of overall survival in patients with esophageal cancer with carcinoma planoepitheliale or adenocarcinoma after brachytherapy (BT)
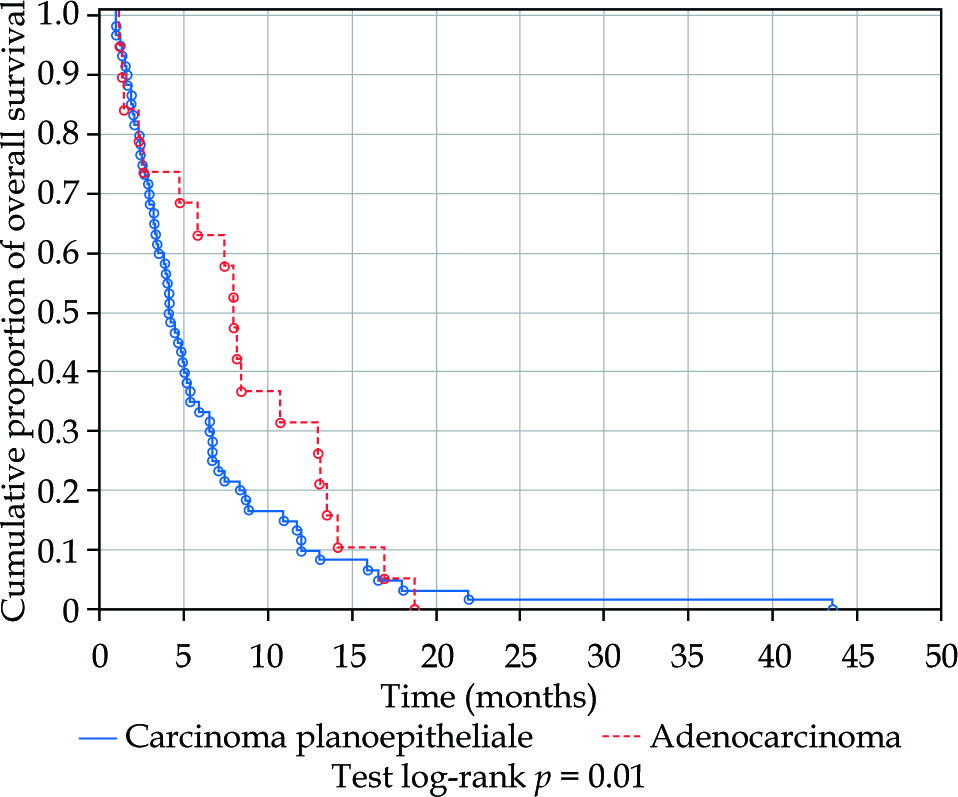
Fig. 5
Kaplan-Meier graph presenting the cumulative proportion of overall survival in patients with esophageal cancer with tumor length ≥ 72.5 mm or < 72.5 mm after brachytherapy (BT)
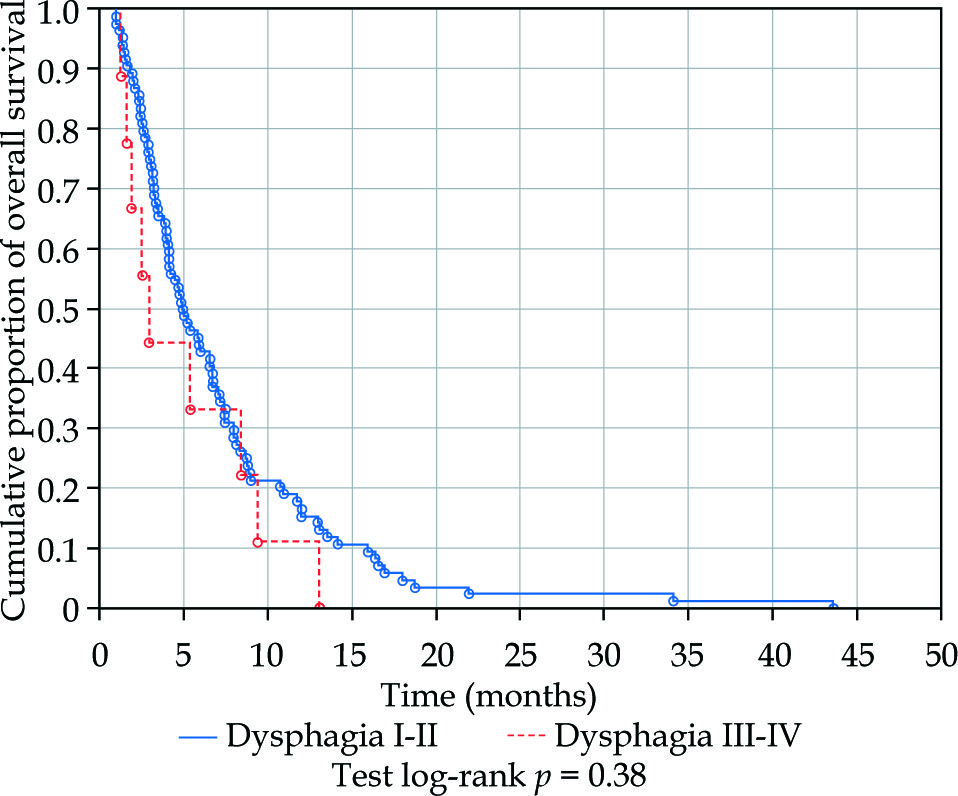
After dividing the patients into the group with mild dysphagia (grade I-II) and severe dysphagia (grade III-IV) before BT, an influence of dysphagia intensity on survival was not detected (4.9 vs. 2.9 months, p = 0.38; Figure 6).
Fig. 6
Kaplan-Meier graph presenting the cumulative proportion of overall survival in patients with esophageal cancer with initial dysphagia grade I or II and III or IV after brachytherapy (BT)
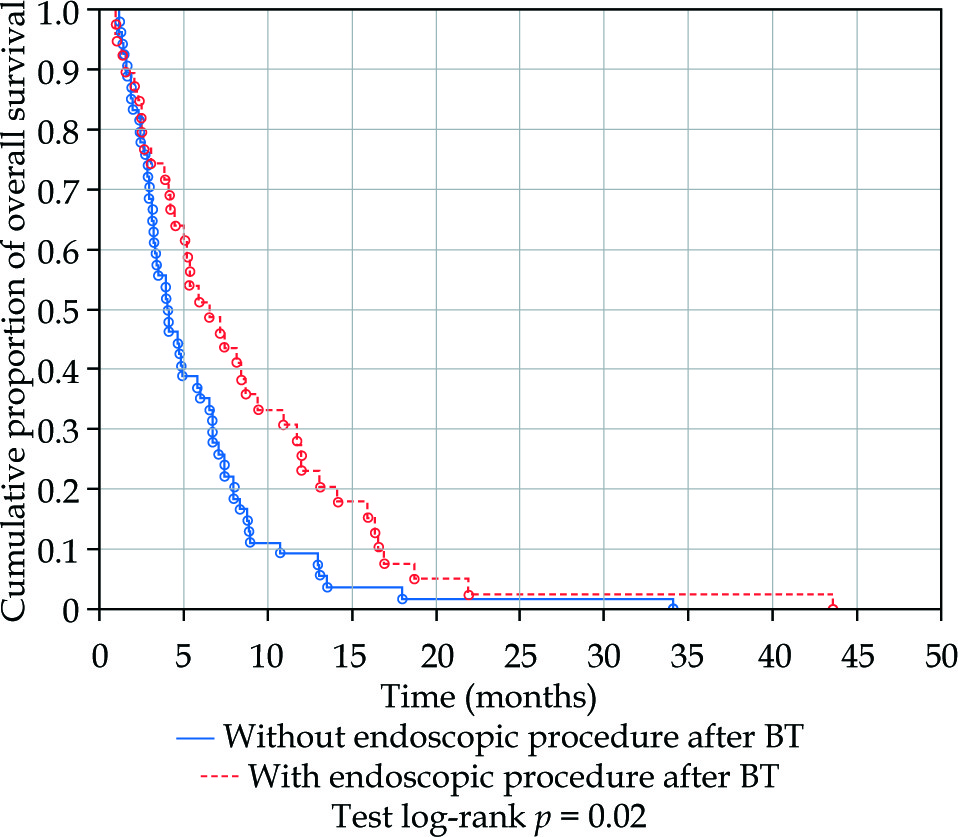
In the treated group of patients an influence of tumor location in the cervical, upper thoracic, lower thoracic part of the esophagus and in the gastro-esophageal junction (GEJ) on survival after BT was not revealed (median 2.6 vs. 3.3 vs. 5.3 vs. 6.6 months, respectively; p = 0.11; Figure 7). All patients with persistently severe or progressive dysphagia despite BT treatment or with dysphagia recurrence during the follow-up period were redirected for endoscopic procedures. The cumulative group of 42% of patients had endoscopic procedures after BT (stenting 25 patients, dilatations 2 patients or nutritional stoma 12 patients). Patients who had endoscopic procedures lived longer than those who were not qualified for them (6.5 vs. 4.0 months; p = 0.02; Figure 8).
Fig. 7
Kaplan-Meier graph presenting the cumulative proportion of overall survival in patients with esophageal cancer located in the upper, middle, lower part of the esophagus or gastro-esophageal junction (GEJ) after brachytherapy (BT)
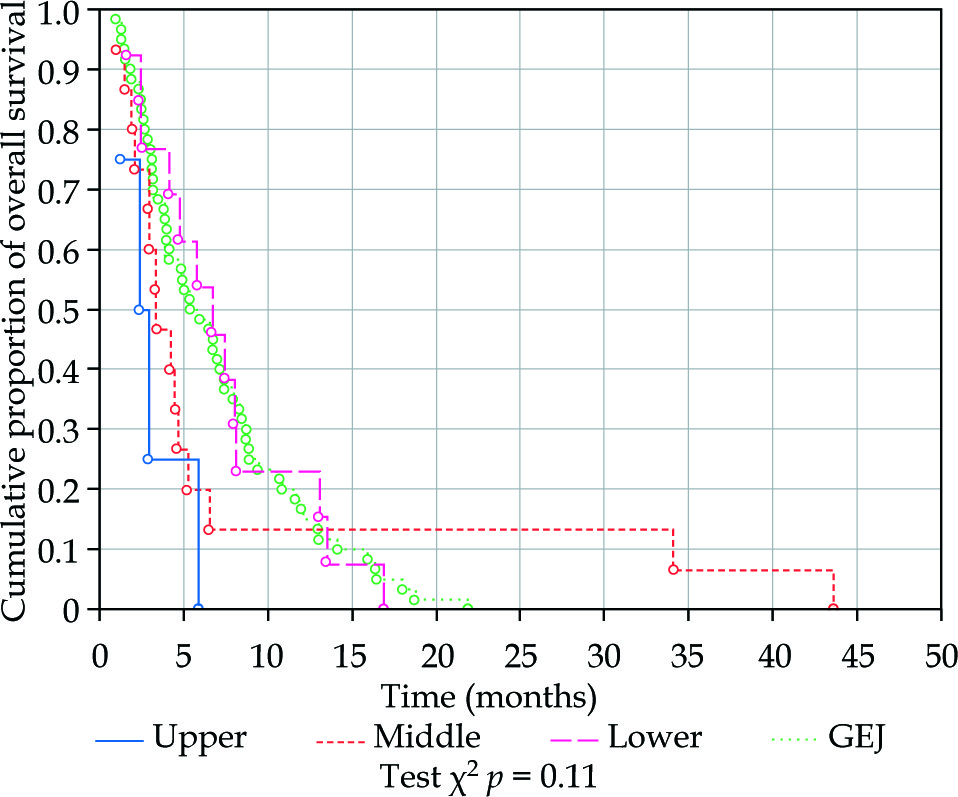
Fig. 8
Kaplan-Meier graph presenting the cumulative proportion of overall survival in patients with esophageal cancer with endoscopic procedure or without endoscopic procedure performed after brachytherapy (BT)
Analysis of factors predisposing to the desired treatment response such as age, grade of dysphagia before treatment, length of infiltration, tumor location and histopathological tumor subtype were statistically insignificant in the logistic regression model (Table 2).
Table 2
Results of univariate logistic regression for predictive factors for dysphagia relief after brachytherapy.
| OR | –95% CI | +95% CI | p | |
|---|---|---|---|---|
| Age | 1.055 | 0.200 | 5.561 | 0.949 |
| Tumor length | 0.226 | 0.017 | 2.978 | 0.251 |
| Localization | 0.202 | 0.029 | 1.390 | 0.099 |
| Dysphagia before | 0.893 | 0.171 | 4.659 | 0.893 |
| Histopathology | 0.479 | 0.121 | 1.899 | 0.289 |
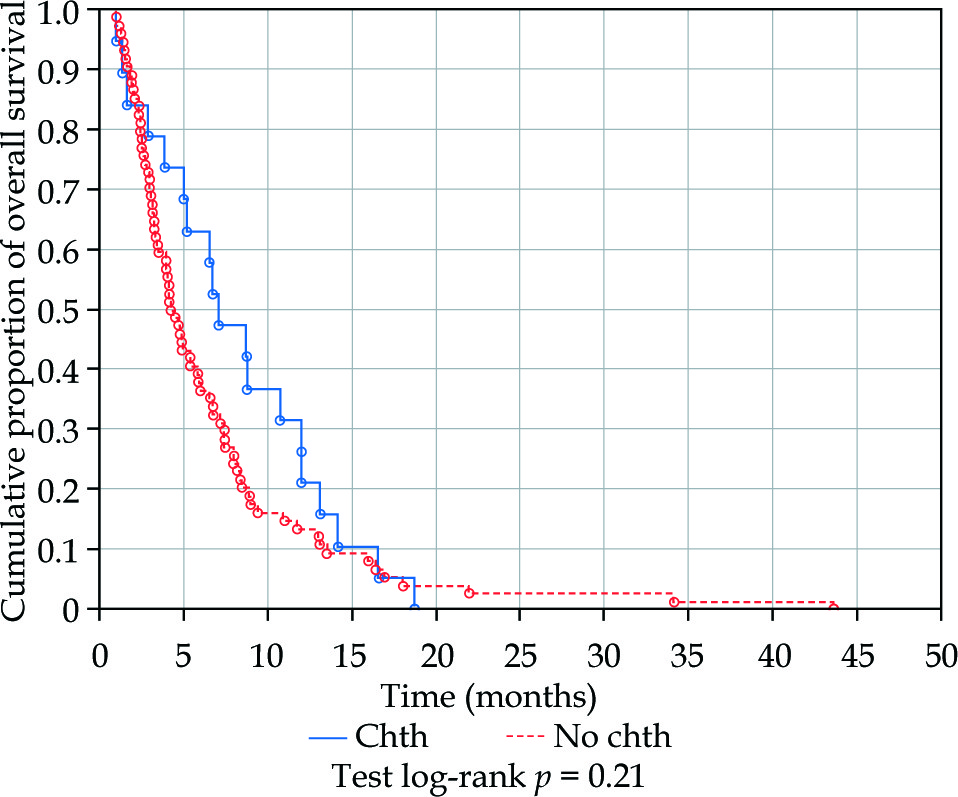
There were observed 4 cases of grade 4 toxicity in the form of tracheoesophageal fistula (5.3%) and 1 case of grade 3 toxicity in the form of bleeding (1.1%). Two fistulas occurred in patients with tumors located in the upper thoracic esophagus, one in the lower thoracic esophagus and in one case of the cervical part of the esophagus. Patients with fistulas were salvaged with coated prostheses or nutritional stoma. The mean infiltration length in those patients was longer than 9 cm. Three of them received chemotherapy despite the recognition of the fistula. However, adding chemotherapy in the whole group of patients (n = 19) did not influence overall survival (7.0 vs. 4.3 months; p = 0.21; Figure 9).
Fig. 9
Kaplan-Meier graph presenting the cumulative proportion of overall survival in patients with esophageal cancer treated only with brachytherapy (No chth) or who additionally received chemotherapy before or after brachytherapy (Chth)
One patient, in whom bleeding occurred, discontinued BT and received delayed palliative EBRT. Three other patients were salvaged with EBRT 20-30 Gy after progression.
Discussion
The prognosis in patients with advanced esophageal cancer is poor. Only 20-25% of patients in stage IV live longer than a year from diagnosis [10]. The primary purpose of oncological treatment is prolonging life and maintenance or improving its quality is the aim of palliative treatment [3].
Brewster et al. in a retrospective study stated, as in this paper, that dysphagia relief after BT was related to the improvement of overall survival. The authors revealed a profit in survival in those patients who responded well to brachytherapy in comparison to those with stable or progressive disease (respectively 193 vs. 121 vs. 118 days; p = 0.0001). In their study, 197 patients were administered HDR-BT in one fraction of 15 Gy. Dysphagia relief occurred in 54% of patients. Tumor pathological subtype proportions were comparable to ours (65% of SCC and 25% of AC), the median OS was approx. 4.4 months. However, the median patients’ age was higher (73 years), and patients were previously treated against dysphagia with various methods: esophageal dilatation (37%), surgery (14%), EBRT + BT (14%), EBRT (6%) or laser (6%) [11]. The current study focuses on patients who were not treated with any of these methods, and it makes it easier to assess the influence of 3 × 7.5 Gy BT on dysphagia relief.
Skowronek et al. published in 2004 the results of a retrospective study on 91 patients who also lived longer after a good response to BT. They were treated with the same schedule of 3 × 7.5 Gy, but were younger (median 59 years) and in the majority diagnosed with SCC (78%). Response to the treatment was assessed only at the first follow-up visit: complete remission (CR) was achieved in 21/91 patients (23.1%), partial remission (PR) in 52 (57.1%), stable disease (SD) in 17 (18.7%) and progressive disease (PD) in one patient (1.1%). Median OS was 8.2 months at a mean follow-up of 7.4 months. The response to the treatment had a statistically significant influence on overall survival (CR – 14.6 months; PR – 7.2 months; SD – 3.8 months; p = 0.00001). Also, the authors showed that besides the response to treatment, the factors related to prolonged survival were older age, better performance status and shorter length of tumorous infiltration [12].
Rupinsky et al. presented results of a randomized study on patients with dysphagia treated with argon plasma coagulation (APC). Then in one arm of the study, patients were administered photodynamic therapy (PDT) and in the second arm BT with a single dose of 12 Gy. In the BT arm they obtained the lowest complication rate, the best quality of life and the longest time of life without dysphagia after treatment (35 vs. 59 vs. 88 days for APC, APC + PDT and APC + BT, respectively; p = 0.006). In this study factors related to survival after BT and differences in OS between the arms were not investigated [13]. Similarly, a group of researchers from the Republic of South Africa did not analyze those factors in terms of OS after BT. In their randomized study on a group of 172 patients treated with 12 Gy in 1 fraction, 16 Gy in 2 fractions and 18 Gy in 3 fractions dysphagia relief was observed in 90-96%. The study included 43 patients previously endoscopically dilated, which undoubtedly influenced the final high number of responses. Moreover, 22 subjects (13%) died before or during the treatment and were not statistically analyzed, which could also have significantly influenced the final results presented [14].
In another randomized study, Sur et al. analyzed 232 patients in the median age of 56 years and diagnosed with SCC, without initial treatment. Patients were administered 18 Gy in 3 fractions (group A) and 16 Gy in 2 fractions (group B). They observed dysphagia relief in 78-84%. About 12% of patients did not improve after treatment, 10% had consequential esophageal stenosis, and 10% had bronchial fistulas. There were no differences in dysphagia relief, survival or toxicity regarding the dose delivered [15].
Researchers from the Netherlands attempted to distinguish the patient groups that should undergo BT or stenting. They combined a group of patients from the previously mentioned trial SiREC (n = 209) with a group of patients treated with BT (doses of 12-15 Gy) or stented in Erasmus MC hospital in Rotterdam. There were 605 cases analyzed, and on that basis, a prognostic model for the best alternative option was developed. In the model, sex, age, tumor length, presence of metastases and general health status were analyzed. Results of 5 or more points were related to shorter survival, and then the prosthesis should be offered. Results of less than 5 points in the model indicated the patients with a prognosis of more prolonged survival, and these should be directed to only BT treatment [16]. It is worth noting that similarly to the current study the tumor location and the grade of dysphagia were not related to worse survival and were not included in the model.
The randomized studies listed above were included in a meta-analysis presented by Fuccio et al. from Italy. They showed in the meta-regression model that expected dysphagia-free survival after 3 months for a cumulative dose of 12 Gy was 50.3%, and after 9 months it was only 17.2%. Results for a dose of 21 Gy were significantly better and were 84.1% and 64.1%, respectively. It was stated in the conclusion that a higher dose may be related to longer dysphagia-free survival [17]. In the current study an even higher dose of 22.5 Gy in 3 fractions was used, and such good results as calculated in the meta-analysis were not achieved. Nevertheless, in our group of patients, BT was the initial treatment, and only 42% of patients demanded subsequent endoscopic treatment, which was much more often used in the mentioned studies. Also, placing the prosthesis influenced survival favorably in our patients. In the mentioned study by Rupinsky et al. subsequent endoscopic treatment was much more frequently necessary irrespective of the method of treatment (61-70%) [13].
Another study by Sur et al. from 2004 was based on an analysis of 60 patients treated with BT because of dysphagia caused by inoperable esophageal cancer. Treatment consisted of 16 Gy in 2 fractions. Afterward, one arm received EBRT (30 Gy in 10 fractions) and the second arm was treated conservatively. Results concerning OS and dysphagia-free survival were similar in both groups [18].
A similar study schema was conveyed by Rosenblatt et al., who published in 2010 the results of a randomized trial of the same structure but a larger group of 219 patients. This time they showed that adding EBRT (10 × 3 Gy) to BT (2 × 8 Gy) results in longer dysphagia-free survival. Both arms of the study had the same toxicity rates. This trial points to the validity of 10 × 3 Gy EBRT after BT [19]. A shorter regimen of 5 × 4 Gy in combination with BT was the basis of the randomized trial IAAE NCT00665197, closed in 2011, but its results have not been published yet [20]. Moreover, in the Netherlands, accrual has begun for the POLDER1 study comparing BT (1 × 12 Gy) with EBRT (5 × 4 Gy), the results of which may bring some new information about managing esophageal cancerous dysphagia [21]. Despite convincing study results proving the role of BT in prolonging dysphagia-free survival and improving the quality of life, BT is more often displaced by other methods of treatment, probably due to its limited availability [22]. Additionally, many cancer centers, especially in developing countries, still have a problem with access to computed tomography-based treatment planning for palliative purposes. 2D HDR-BT seems to be a convenient treatment method, especially for these populations.
Conclusions
2D HDR-BT is a quick and effective method of dysphagia treatment in patients with advanced esophageal cancer. Results of several studies indicate that partial or complete dysphagia relief prolongs OS. Progression after BT relates to poorer prognosis and suggests that the patients need different management, and the most favorable appears to be endoscopy procedures. To reach a conclusion on which management to choose after BT to achieve a good quality of life and longer overall survival, further research is required. In summary, 2D HDR-BT meets the assumptions of palliative treatment for advanced esophageal cancer.








