
Introduction
Pentalogy of Cantrell (PC) is an extremely rare multiple congenital anomaly syndrome, characterized by the presence of five major malformations: midline supraumbilical abdominal wall defect (which results in omphalocele), lower sternal defect, diaphragmatic pericardial defect, anterior diaphragmatic defect and various intracardiac malformations (mostly ventricular septal defect) [1]. Additionally, although not part of the classic PC, some severe cases have been associated with herniation of the heart through the diaphragmatic defect, resulting in ectopia cordis (EC) [2]. Such a diagnosis carries a disastrous prognosis without surgical correction or palliation [3]. Furthermore, miscellaneous intracardiac abnormalities even worsen the survival. Multiple chest interventions and complex anatomy impede their surgical treatment; therefore, the transcatheter approach may be the only possibility. According to our best knowledge, no percutaneous atrial septal defect (ASD) closure has been reported in a patient with PC.
Case report
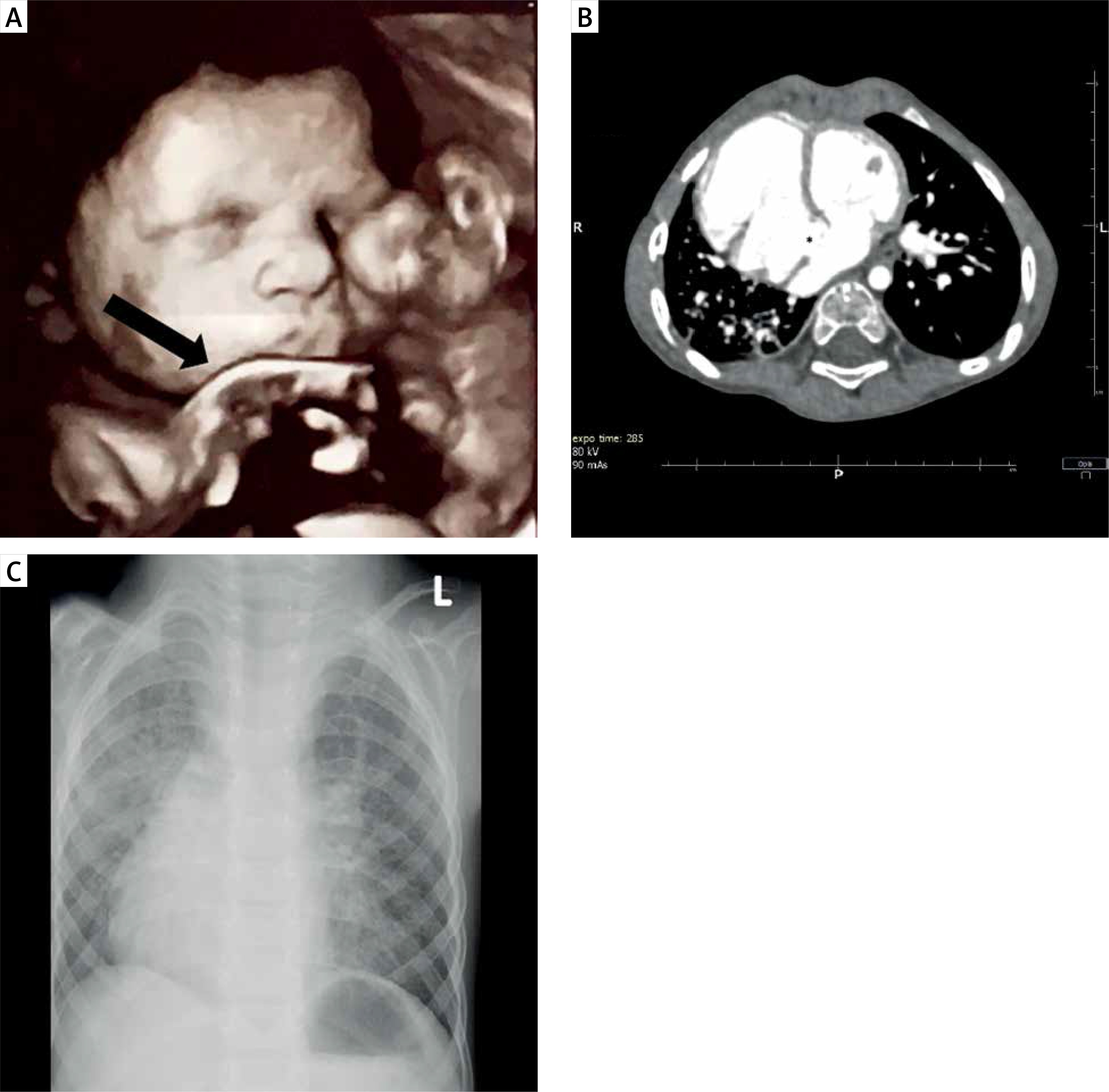
Omphalocele with incomplete ectopia cordis were diagnosed during routine ultrasonography of a 13-week pregnant young woman with celiac disease. Chromosome abnormalities were excluded in amniocentesis soon after. Over the next repetitive fetal echocardiography studies partial withdrawal of the heart from the hernia into the thoracoabdominal cavity was noted. During the last examination at the 36th week the heart’s apex (left-sided) was positioned in the hernia’s gates (Figure 1 A). After successful delivery by caesarean section at 39 weeks, the 3250 g and 54 cm male was transferred to the operating theatre (7/9 Apgar, with multiple syndactyly in both feet). The pericardium was separated from the peritoneum, the heart transferred to the thoracic cavity, the diaphragm reconstructed and the omphalocele content – part of the liver and stomach as well as small intestine – inserted into the abdominal cavity. Because of the thoracic cavity defect, the heart was covered only with skin and its beating was easily seen. Control transthoracic echocardiography (TTE) showed dextrocardia with right-sided apex (as a result of the heart’s surgical displacement) and 7 mm ASD. At 11 months the child had a chest wall reconstruction performed using autologous bone and cartilaginous grafts. At the age of 2 years TTE showed hemodynamically significant ASD with right ventricle (RV) enlargement and computed tomography was performed in order to visualize the heart’s specific anatomy (Figure 1 B). The boy was disqualified from surgical ASD correction in the primary center.
Figure 1
A – 4D Real-time fetal ultrasonography at 36 weeks: 52 × 50 mm omphalocele in the foreground (parent’s courtesy). B – Computed tomography scan (2 years old): heart on the right side, right ventricle enlargement, atrial septal defect – asterisk (no sternum). C – Chest X-ray (3 years old): dextrocardia, significant vascular marking
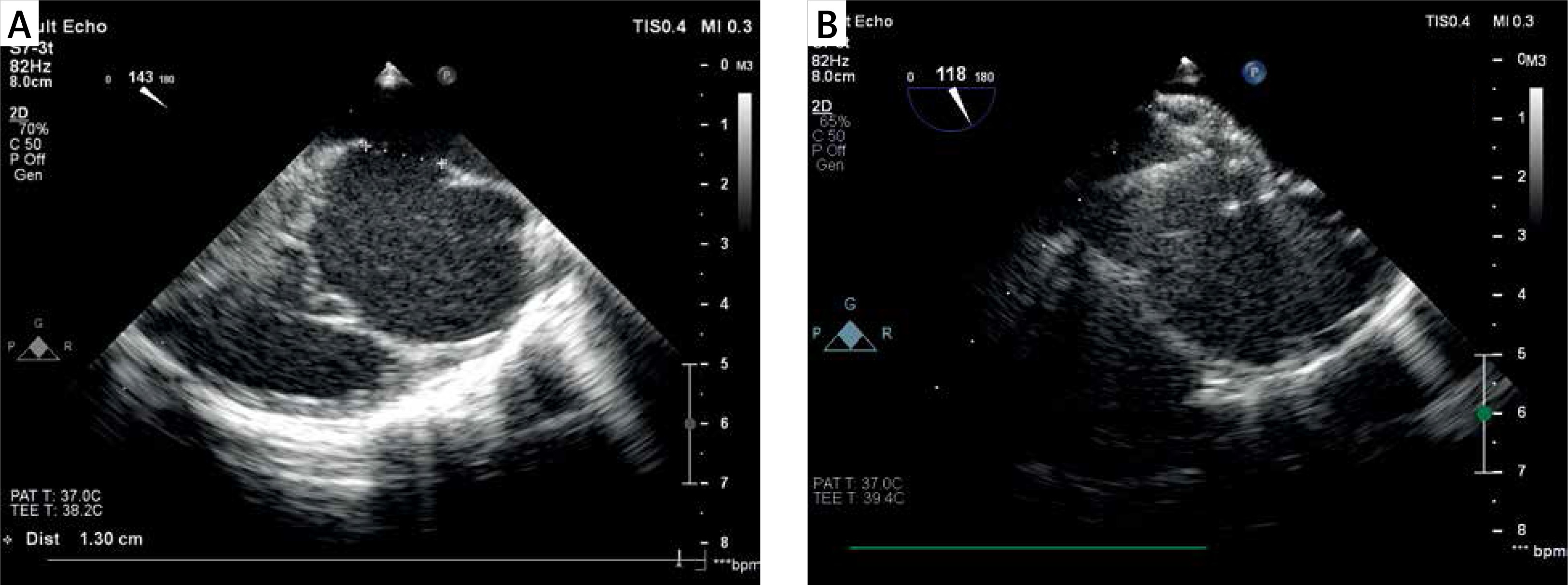
The patient was admitted to our department for the first time at the age of three. He was asymptomatic, but with slow weight gain – only 11 kg (< 3rd percentile) – and on a low dose of diuretics. Physical examination revealed thoracic wall deformation and systolic 2/6 murmur on the right side of the chest. Dextrocardia and significant vascular marking were seen in X-ray (Figure 1 C). Transoesophageal echocardiography (TOE) was performed in nonstandard projections due to the heart’s displacement and showed 13 × 9 mm centrally located ASD with unstable anteroinferior rim and with significant left-to-right flow (Figure 2 A). Despite low weight and possible technical and anatomical difficulties, the patient was qualified for transcatheter defect closure. The procedure was performed under general anaesthesia with intubation and under fluoroscopy and TOE guidance. After obtaining right femoral vein access (5 F), 100 IU/kg of heparin was administered. After diagnostic catheterization the guidewire was positioned in the right upper pulmonary vein in order to provide proper support. Mean pulmonary artery pressure was 12 mm Hg. Due to the satisfactory view, we did not perform balloon calibration of the defect. After insertion of the 8 F transseptal sheath over the Amplatz super stiff guidewire, a 12 mm Amplatzer septal occluder (Abbott Structural, Minnesota, USA) was finally implanted from the position in the left atrium (Figure 2 B). The successful deployment was preceded with several device rotation maneuvers and repositions. The proper occluder position was confirmed with the push-pull maneuver. The fluoroscopy time was 7 min. Both in TOE and TTE a stable device position and no residual flow through the septum were seen after the procedure. Aspirin 3 mg/kg was administered for 6 months. Four-month follow-up has been uneventful with weight gain to 12.5 kg and RV dimension reduction in a routine follow-up TTE after a month.
Discussion
Pentalogy of Cantrell was first described in 1958 [1] and is found in 5.5 per 1 million live births. Although the pathogenesis of the PC has yet to be fully elucidated, it is attributed to a developmental failure of lateral mesodermal folds to the midline migration between day 14 and 18 of embryogenesis, resulting in septum transversum defect [1]. Additionally, although not part of the classic PC, some severe cases have been associated with heart herniation [2]. Ectopia cordis itself is characterized by complete or partial displacement of the heart outside the body. Cervical, cervicothoracic, thoracic, and thoracoabdominal types of EC have been described. Ectopia cordis can be an isolated defect, but more frequently is a part of a PC [4]. Fetal echocardiography is an excellent tool for EC diagnosis [5]; however, the use of prenatal magnetic resonance imaging was described to enhance the exact anatomy visualization [6]. Pentalogy of Cantrell remains a disease with poor prognosis; nonetheless, survival to adulthood with mild thoracoabdominal abnormalities has been reported. Patients with both PC and EC have even worse prognosis [3]. Less than 5% of patients with isolated EC survive [7]. The treatment of PC consists of corrective or palliative cardiovascular surgery, correction of ventral hernia and diaphragmatic defects as well as correction of associated anomalies [8]. A survival rate of 61% has been reported in patients with PC [9]. Concomitant EC requires surgical internalization of the heart into the thoracic cavity, which is associated with high risk of cardiovascular compromise and ischemia, thus needing a staged approach in particular cases [10]. Intracardiac anomalies worsen the prognosis of patients with PC and only a few reports of percutaneous approach have been reported to date. McMahon reported successful palliative right ventricular outflow tract stenting in a patient with partial PC, dextrocardia, double outlet right ventricle and pulmonary stenosis [11].
We report a 3-year-old boy with dextrocardia after surgical correction of PC and partial EC, in whom we closed ASD percutaneously. To the best of our knowledge, transcatheter ASD closure in a PC case has not been reported yet. The patient was qualified for transcatheter ASD closure because of both ASD and right ventricle enlargement as well as a low weight gain (11 kg, < 3rd percentile), which can be attributed, despite other comorbidities, to the hemodynamically significant shunt. Interventional closure of ASD in such small children is not a routine approach, waiting to older age being preferred. However, good results of such treatment have been reported [12]. In selected ASD cases, the defect can enlarge with time, and if the patient is qualified too late, a percutaneous closure may be impossible due to too high device diameter to patient’s weight ratio (mm/kg) [13]. Such a phenomenon was observed in our case and justified early intervention. If the aforementioned ratio is higher than one, as in our patient, the procedure becomes technically difficult with more frequent repositions needed to properly deploy the device. The heart’s displacement (dextrocardia) which was a result of PC and the corrective surgery on the first day of life with the heart insertion into the thoracic cavity and pericardium reconstruction as well as the unfavorable defect anatomy with unstable anteroinferior rim were major challenges during our procedure. Successful occluder implantation needed a few rotations of the delivery system and several repositions of the device. So far, transcatheter closure of ASD in a patient with dextrocardia and situs solitus has been described with favorable results [14]. Three-dimensional image fusion may be helpful in such demanding cases in the near future.







