
Introduction
Bladder cancer (BC) is the ninth most common malignancy worldwide with a yearly incidence of approximately 430,000 cases, and it is positioned 13th in terms of yearly oncological mortality [1]. It is estimated that 3/4 of primary diagnosed bladder tumours present as non-muscle invasive cancers (NMIBC) – a group comprising lesions limited to bladder mucosa (stage Ta and CIS) and infiltrating submucosal layer of the bladder wall (stage T1). Due to non-advanced stage, correctly managed NMIBCs present relatively good survival rates, but with a high perpetual risk of tumour recurrence or progression to muscle invasive disease. Therefore, precise and meticulous diagnostic and therapeutic proceedings must be employed.
It must be emphasised that both NMIBC diagnosis and treatment rely on endoscopic transurethral resection of bladder tumour (TURB). Because of the importance of TURB in BC management and the fact that TURB is one of the most commonly performed urologic procedures, it is the subject of continuous technological development.
The aim of this paper is to present available data on new technological developments in the surgical technique of TURB.
Evidence acquisition and evidence synthesis
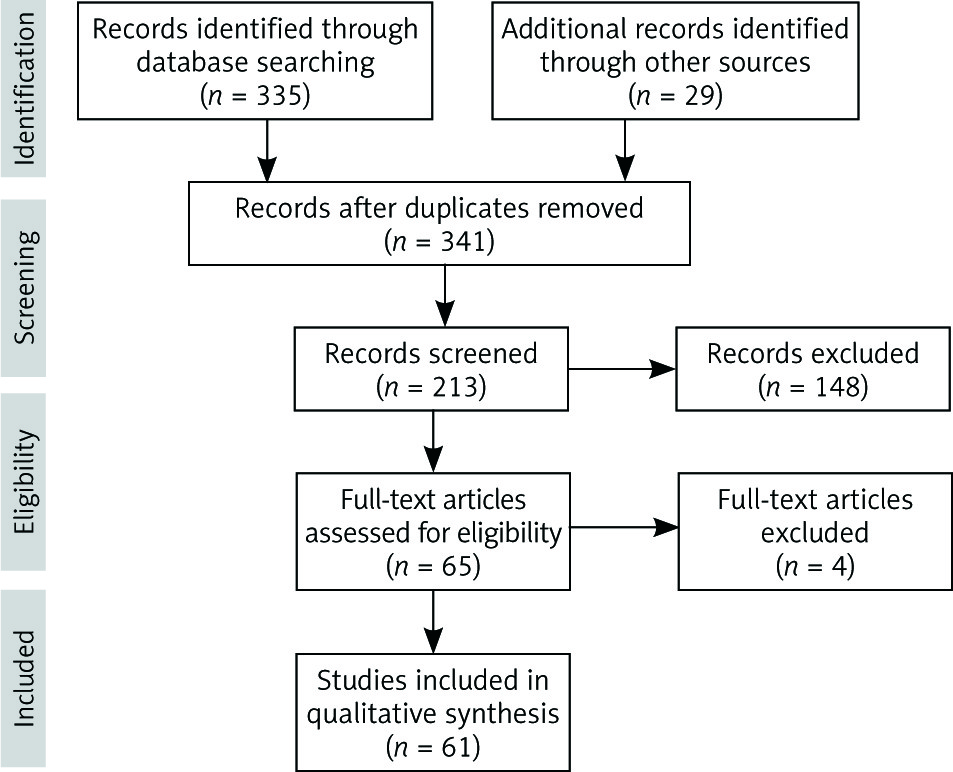
A literature search according to PRISMA guidelines within the Medline database was conducted in December 2018 for papers presenting the technical developments of TURB, without setting time limits, using the terms “bladder cancer” in conjunction with TURB, monopolar, bipolar, plasmakinetic, laser, and en bloc. Boolean operators (NOT, AND, OR) were also used in succession to narrow and broaden the search (Fig. 1). AutoAlerts in Medline were also run, as well as reference lists of original articles and review articles for further eligible data. Additionally, resource centres from the largest urological conferences were searched. The search was limited to English, Polish, German, and Spanish literature. Articles that did not address the topics were excluded, and the full text of the remaining articles was subsequently reviewed.
Fig. 1
The flow of information through the different phases of the systematic review (adopted from www.prisma-statement.org)
Discussion
Conventional resection
The procedure of transurethral tumour resection was first performed and described by Edwin Beer in 1910 [2]. From that moment, despite the technological advancement in the subsequent 100 years, the main idea of TURB remained the same. According to European Association of Urology (EAU) guidelines, the goal of TURB in Ta and T1 BC is to make the correct diagnosis and completely remove all tumours with appropriate muscular layer sampling. In muscle-invasive disease radical excision is often impossible, and therefore the most important objective is an accurate diagnosis based on the analysis of muscle invasion.
The gold standard for transurethral resection of bladder tumours is conventional TURB (cTURB), classically performed with monopolar current (mTURB). The cTURB is widely used, and therefore tremendous experience in this procedure been accumulated over the years. The procedure is performed in the lithotomy position, mainly under spinal anaesthesia. However, because of lack of muscular relaxation, and the fact that during monopolar electrocautery the electric current runs from the resection loop through the patient’s body to the grounding pad placed on the patient’s skin, there is a high risk of obturator nerve stimulation (obturator reflex). Due to abrupt adductor muscle contraction, accidental perforation of the bladder wall with thermal damage of adjacent tissue may occur. Additionally, when monopolar energy is applied, the electrical resistance generates a high temperature (up to 300–400°C) with significant collateral and penetrative tissue injury, which might hamper deeper resection and result in a significant charring of the specimen tissues leading to cancer mis-staging or mis-grading [3]. Finally, mTURB is performed in a nonconductive irrigative solution (water, glycine, sorbitol, or mannitol). The excessive absorption of this fluid into the opened vessels and subsequent fluid and electrolyte abnormalities may cause the life-threatening TUR syndrome.
To overcome those shortcomings, bipolar current was introduced in BC resections (bTURB). In this setting, isotonic saline is used as the irrigant, and the electric current runs between two electrodes incorporated in the resectoscope. Highly ionised particles (plasma field) created around the resection loop disrupt the organic molecular bonds between tissues, generating much lower temperatures (40–70°C) when compared to monopolar energy [4, 5]. Because of those facts, the resection with bipolar energy is more precise with better haemostatic and less charring effect on both the resection bed and histopathological samples. Additionally, bTURB is a safer option for patients with implanted pacemakers or pregnant women [6].
To date, various authors have tried to compare monopolar resection with newer, bipolar resection, but with conflicting results. In the paper by Del Rosso et al. 132 patients were randomised to undergo mono- or bipolar resection of primary NMIBC. The authors demonstrated that bTURB represents a safe and effective procedure in the management of NMIBC; however, the study does not present any advantage between study groups apart from hospitalisation and catheterisation times [7]. Another randomised study included 147 patients and showed statistical differences in the incidence of obturator reflex and lower incidence of severe cautery artefacts in the bipolar arm. Nevertheless, there were no significant differences in other analysed variables [8]. In the study analysing quality of bladder detrusor muscle sampling by Teoh et al., the authors randomised 160 patients to both procedures and noted that bTURB was significantly associated with better muscle sampling, with an odds ratio (OR) of 2.23. Additionally, fewer patients in the bTURB group required postoperative irrigation when compared to patients in the monopolar arm [9]. In another prospective, randomised analysis, 130 patients underwent mono- or bipolar TURB. The authors did not find any statistical differences in tumour resection completeness, muscle sampling, or thermal specimen damage rates. However, obturator reflex was experienced in 21.5% of the patients in the monopolar TURB group and in 4.6% of the patients in bTURB group. Additionally, the number of bladder perforations was significantly higher in mTURB (21.5% vs. 6.1%) [10]. These observations were confirmed in a large retrospective analysis of perioperative outcomes of 8188 mono-bipolar pairs. Sugihara et al. showed that bTURB was associated with a substantially lower incidence of perioperative complications, including severe bladder injury [11]. On the other hand, another retrospective TURB complication analysis on 586 procedures by Avallone et al. did not show any statistically significant differences between investigated procedures. The authors emphasised that obturator reflex and significant adductor contraction can also occur during bTURB. Similarly, a post-hoc analysis from a randomised trial of various visualisation methods during TURB did not find any statistically significant differences between the two methods. The authors stated that bTURB seems to have no evident advantages over mTURB with respect to operation time, perioperative and postoperative complication rates, and recurrence rates at 12 months [12].
Finally, in a meta-analysis including almost 1000 patients from eight trials, bTURB was associated with shorter operative time, shorter hospital stay, less blood loss, and shorter catheterisation time. What is more, there were fewer complications such as obturator reflex and bladder perforation in the bTURB group. Also, the recurrence rates up to two years after the procedure were slightly more favourable for bTURB [6]. Nevertheless, another meta-analysis did not corroborate those findings; Cui et al. found that there were no statistically significant differences between bTURB and mTURB in terms of obturator reflex, bladder perforation, and transfusion rates. Also, the grade of tissue sample cautery artefacts and recurrence rate did not differ significantly [13].
In conclusion, despite extensive experience and an abundance of reports, available studies do not provided solid evidence that bipolar resection is superior to monopolar resection in terms of surgical outcome, complication risk, or tumour recurrence rate.
En bloc transurethral resection of bladder tumour
The main disadvantage of cutting wire-loop resection is the necessity to use the “incise and scatter”, piece-by-piece technique. As is widely known, scattering the neoplastic tissue runs against the basic principles of oncological surgery, leading to exfoliation of numerous cancer cells. Theoretically, it may cause out-of-field recurrences by implementation of circulating cells [14]. Because the residual tumour rates after TURB concern up to 35% of cases and recurrence of up to 75% of patients, at least some of those clinical events may be caused by implementation of released cancer cells [15]. The other major problem of cTURB is the difficulty in accurately pathologically evaluating fragmented, disoriented, and heavily damaged samples. This often leads to inaccurate invasion depth and malignancy grade determination [16]. It is widely known that the presence of lamina muscularis of the bladder in the histopathological specimen is considered a surrogate criterion of the operation quality. As shown in the literature, the absence of muscle in the specimen is associated with a significant risk of residual disease, tumour misstating, and early recurrence [17].
For those reasons, the en bloc resection concept was developed. It comprises resection of the whole tumour in one piece – the exophytic papillary tumour together with the base and bladder wall fragment. When the lesion is resected in that manner, the normal histological relations of the specimen are preserved, rates of lamina muscularis presence go beyond 95%, and the cells’ dispersal is (theoretically) diminished [18, 19]. What is more, excellent bleeding control is possible [16].
The en bloc technique differs slightly between various studies; however, the main principles include: 1) creating a circular incision up to the depth of the muscle layer at some distance from the tumour; 2) progressive dissection of the lesion within the muscular layer using both blunt dissection and some form of energy, mainly in a “flash-firing” fashion; 3) final detachment of the tumour; and 4) tumour retrieval through the resectoscope [20]. For smaller tumours one-swing loop resection or the “grasp and bite technique” can also be used [21]. Finally, thermal/laser ablation in local anaesthesia of small lesions with strong low-grade conviction may be employed, especially in an outpatient follow-up setting [22]. Nonetheless, being therapeutic enough in selected cases, fulguration cannot be classified as en bloc resection.
The major drawback of the en bloc technique is the tumour size limit, which must finally fit and be pulled in one piece through the working channel of the endoscope. Depending on the tumour morphology, cohesion, and amount of resected bladder wall, a diameter of 3 cm is generally considered the upper limit of tumour size that can be extracted in one piece [18].
In the available literature various retrieval methods have been described. The easiest ones comprise simple washing with or without pressure evacuators and usage of cystoscopy graspers or a thick vaporisation loop. Some authors advocate wedging the specimen in front of a resectoscope beak and subsequently removing the whole instrument through the urethra [23]. Naselli et al. describe usage of laparoscopic forceps for the retrieval of tumours as large as 4.5 cm [24]. Similarly, Hurle et al. used a nephroscopy sheath and a laparoscopic grasper [25]. In a paper by Maurice et al., the authors described usage of a nylon mesh retrieval net to retrieve tumours larger than 5 cm [26]. Other authors reported retrieval of tumours with standard endo-bags commonly used in gastroenterology [27]. Finally, some authors propose the extraction of non-compliant lesions by cutting the specimen into a few pieces [16]. However, in cases when the tumour is retrieved in front of the whole instrument, it subjectively seems that theoretical urethral seeding has to be considered so as not to compromise oncological principles.
Some other en bloc problems may be related to lesion location, with the most difficult resection in the bladder dome, anterior wall, and bladder neck. However, it has to be remembered that the cTURB also yields some risks in those locations, and as the growing experience shows – it is not smaller when compared to en bloc.
En bloc resections can be performed by means of various energy sources including electric energy and lasers.
En bloc with electric energy
The first reports of en bloc resection were delivered in the late 1990s [28, 29]. To perform the procedure, Ukai et al. used a modified J-shaped monopolar loop. The electrode was created from a traditional right-angle loop electrode with the left half of the loop cut off, and the right half trimmed to 2 mm and then bent inward. Later, the knife electrode was presented by Saito et al., flat loop by Lodde et al., and Collins loop by Hurle et al. [25, 30, 31]. In the literature we can also find reports about en bloc resection with classic wire loop, as well as bipolar loop or bipolar “button” [32–35].
To date, several studies comparing electric en bloc resection and classical resection were published. Sureka et al. showed in a prospective non-randomised study on 45 patients that there was a significant reduction in the recurrence rate and time to recurrence with en bloc when compared with mTURB. However, the progression rate did not differ significantly [34]. In the next study on 90 patients by Zhang et al., the authors did not show statistically significant differences in operative time, surgical complications, and recurrence rates between the groups. However, the detrusor muscle could be identified in 100% of en bloc specimens but only in 70% of cTURB samples [35]. In other study, 90 patients were prospectively randomised to undergo bipolar button en bloc or mTURB. Reduced obturator reflex rate, mean operation time, haemoglobin level drop, catheterisation period, and hospital stay were observed in the en bloc arm. Additionally, a lower recurrence rate was found in the en bloc group with decreased rate of heterotopic recurrent lesions [33]. Finally, in a meta-analysis of 886 patients (438 en bloc, 448 cTURB) Wu et al. proved that hospitalisation and catheterisation time were shorter in the en bloc group with no significant difference in operation time. Also, there was a significant difference in recurrence and complication rates in favour of en bloc resection [36].
En bloc using water dissection
One of the difficulties in en bloc resection is finding and following the right, deep plane of dissection, without perorating the bladder. This is particularly important in tumourslocalised in the bladder dome or posterior wall and in patients with atrophic or severe obstructive bladder.
In such cases, the well-known gastroenterological tool, a water-jet dissector, may be helpful. The main idea of the device is to create a fluid cushion underneath the tumour by injecting saline, elevate the lesion, and therefore facilitate precise and safe resection.
In the available literature only a few case series of hydrodissection usage in NMIBC are available. In those, the authors present their experience with tumours up to 7.5 cm in diameter [27, 37, 38]. What is worth mentioning, good quality data regarding this method are presented at international conferences. In the 2017 Société Internationaled’Urologie (SIU) conference, Hu presented single-centre, randomised, controlled trial results from 86 patients receiving either en bloc transurethral water jet resection or cTURBT. The authors proved that hydrodissection is safe and feasible; however, according to Kaplan-Meier survival curves, there was no statistical difference in the rate of recurrence at 12 months [39]. In the 2017 EAU congress, Gakis et al. presented results of a randomised, controlled trial including 115 patients. Detrusor muscle presence, complication rate, and catheterisation and hospitalisation times were not significantly different between both groups. Despite the fact that the operation time was higher in the en bloc group, the procedure was associated with significantly higher histopathologically confirmed complete resection status (pR0) [40].
En bloc using a holmium laser
The holmium laser is one of the most versatile lasers in urology. This pulsed wave laser with a wavelength of 2100 nm (absorbed by water) may be used for tissue ablation, cutting, coagulation, as well as lithotripsy [41]. Because of its shallow penetration depth and lack of obturator reflex, it allows for very precise tumour resection.
One of the first reports about holmium laser usage in bladder tumour resections was published by SolerMartínez et al. In the study on 36 patients operated under local anaesthesia and sedation the authors presented “photocoagulation” of the papillary bladder tumours. They observed no serious complications, and the recurrence rate was similar when compared to cTURB [42]. In next study, Zhu et al. presented the results of 101 holmium laser resections of bladder tumours (HoLRBT) and 111 cTURBs on 212 patients with primary NMIBC. The complication rates, and irrigation and catheterisation times were lower in the HoLRBT group; however, the cTURB group had shorter operation times. It is worth mentioning that there were no differences in the recurrence-free rates between the study groups [43]. In the study by Xishuang et al. the authors retrospectively evaluated data of 51 patients who underwent mTURB, 58 patients who underwent bTURB, and 64 patients after HoLRBT. They proved that both bTURB and HoLRBT were associated with fewer intraoperative and postoperative complications, as well as less bleeding and shorter postoperative bladder irritation, catheterisation, and hospitalisation times. Once again, there were no significant differences in recurrence rates between groups [44]. In the next study on 27 patients after mTURB and 23 patients after HoLRBT, the authors showed that there were no significant differences in operation time and recurrence rates between the two groups. The HoLRBT group had lower intraoperative and postoperative complication rates, but there were no significant differences in the transfusion rates and occurrence of urethral strictures [45].
En bloc using a thulium laser
The thulium continuous wave laser was introduced in the early 2000s [46]. With a water-absorbed wavelength of 2013 nm (close to the peak absorption of water) and 0.25 mm of penetration depth, the thulium laser allows for very precise and accurate resection [47].
The first reports about thulium laser resection of bladder tumours (ThuLRBT) were presented by Yang et al. and published in a series of articles. The authors stated that resection with thulium is a safe, efficient, and effective method [48–54]. Zong et al. presented a study on 95 patients comparing thulium, holmium, and conventional resection. The authors observed a lower haemoglobin decrease after the thulium procedure, but no differences in recurrence-free survival were observed [55]. Liu et al. published the results of a prospective, randomised trial comparing ThuLRBT and cTURB. The study comprised 120 patients (56 cTURB and 64 ThuLRBT), and no significant differences in recurrence rates were shown between the groups. On the other hand, intra- and postoperative complications were less frequently observed in the laser group [56]. In another paper, Chen et al. prospectively compared 142 patients undergoing ThuLRBT and cTURB in a randomised manner. The operation times were longer when using laser, but the complication rates were lower. No differences in recurrence-free survival were noted [57]. In the randomised prospective comparison of 143 patients after cTURB and 149 after thulium vaporesection, Zhang et al. showed that operation times were shorter and complication rates higher with cTURB, and there were no differences in recurrence-free and progression-free survival [58]. Migliari et al. compared a prospective group of 58 patients who underwent ThuLRBT with a historical cohort of 61 patients after mTURB. The authors reported lower complication rates and higher rates of lamina muscularis in the specimens from the laser group [59]. In the retrospective study on 256 patients by Li et al., comparing ThuLRBT and bTURB, the authors showed that operation and hospitalisation times, and postoperative irrigation and catheterisation durations were significantly shorter in the thulium group. Also, the rate of bladder detrusor muscle identified in pathologic specimens was higher in patients operated by laser. However, no differences in fever, bleeding, and recurrence-free rates were observed [60].
Lately, a second generation of thulium laser has been introduced in the NMIBC setting (1.9 µm Vela laser) [61]. In the study by Xu et al. the authors compared retrospectively data of 26 patients after ThuLRBT and 44 after cTURB. They observed lower complication rates and better quality of histopathological specimens when using laser; however, there were no differences in procedure duration and transfusion and recurrence-free rates [62].
En bloc using a green-light KTP laser
The first report on green-light laser (532 nm) usage in the NMIBC setting was presented by Tao et al. in the late 1990s. The authors published data comparing 74 patients who underwent laser vaporisation and 84 patients after cTURB. No significant differences were observed in operative time and perioperative and postoperative serum sodium and haemoglobin levels. The green laser was associated with fewer complications, and the recurrence-free rates were lower. Yet, the main disadvantage was the lack of sufficient tissue for pathologic examination [63]. Subsequently, He et al. introduced en bloc with a KTP laser using front-firing fibre on 45 patients, showing the feasibility and safety of the procedure [64]. In the prospective, non-randomised study on 158 patients (83 KTP en-bloc and 75 cTURBT) by Chen et al. the authors showed that resection with laser was associated with lower complication rates and had shorter duration. Still, the recurrence-free survival rate did not differ significantly between the two groups after 36 months of follow-up [65].
One feature of green laser should be emphasised. The KTP laser energy is absorbed by haemoglobin, which results in excellent haemostatic abilities. Hence, the green laser procedure may be performed under local anaesthesia in patients who are under oral anticoagulation. Clearly not being an option for every-day practice, it may be helpful in some carefully selected patients.
Conclusions
In recent years, the technological development in urological surgery has been remarkable. The latest advances in the field of endourology are aimed at increasing surgical accuracy and thus reducing the risk of tumour recurrence and progression. However, despite the constant progress in technology and technique, there are still a lack of good quality data showing the superiority of any of the methods. It should be remembered that, regardless of the surgical method, adjuvant treatment should be implemented in accordance with the current EAU guidelines for NMIBC.






