
Introduction
Rosacea is a chronic inflammatory skin condition with a complex aetiology, primarily affecting the facial skin. It is characterized by episodic flares of symptoms, including erythema, telangiectasia, papules, and pustules significantly impacting patients’ quality of life. The studies indicate that rosacea patients experienced significantly higher levels of anxiety, and depression compared to controls, with disease severity being a strong predictor of these outcomes [1]. Although the exact pathogenesis of rosacea remains poorly understood, growing evidence suggests a pivotal role of skin barrier dysfunction, immune dysregulation, and environmental factors in its development [2]. In recent years, scientific interest has increasingly focused on the skin microbiome, a complex ecosystem of microorganisms residing on the skin, as a potential contributor to rosacea. The interplay between host immunity and microbial communities appears to be critical in maintaining skin homeostasis, while dysbiosis of the microbiome may contribute to the onset and progression of rosacea [3]. This paper aims to explore the relationship between the skin microbiome and rosacea, shedding light on potential mechanisms and therapeutic implications.
Aim
The objective of this study is to investigate the relationship between the skin microbiome and the pathogenesis of rosacea. The study aims to analyse the composition and diversity of the skin microbiome in individuals with rosacea compared to healthy controls, identify potential microbial dysbiosis associated with the development and progression of the condition, and explore the role of microbial interactions with the immune system and skin barrier function. Additionally, it seeks to evaluate the potential of microbiome-targeted therapies as a novel approach to managing rosacea. By addressing these goals, the study aspires to enhance understanding of the role of the skin microbiome in rosacea and identify new avenues for therapeutic interventions.
Methods
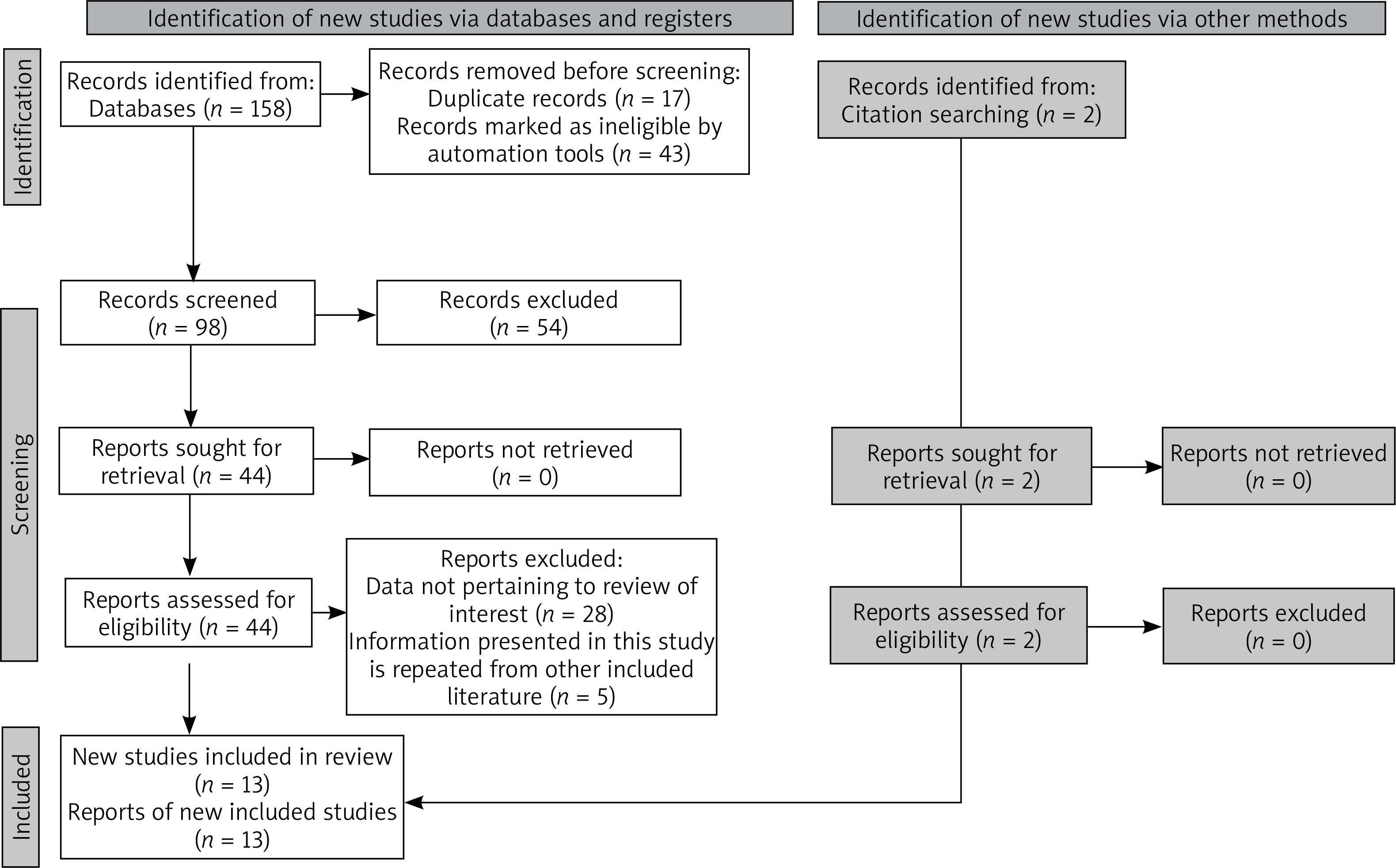
The systematic review was carried out according to the PRISMA guidelines including all types of articles published and included in PubMed and Embase databases from inception to February 2025. The selection process is illustrated by a PRISMA flowchart in Figure 1 [4]. The authors conducted research in PubMed and Embase databases, using MeSH and Emtree terms: “Rosacea” and “Skin microbiome”. After removing duplicates, the articles were manually reviewed to confirm they met the inclusion criteria, with studies lacking a connection to the cutaneous manifestations of the disease being excluded. Only original studies and Mendelian randomisation studies, along with other various research methods, were included in the final analysis.
Results
The results collected are presented in tabular form (Table 1) [3, 5–16], accompanied by detailed descriptions of all studies included in the review.
Table 1
Summary of the literature review on skin microbiota data in patients with rosacea
| No. of study | Year | Authors | Methodology and study population | Key results |
|---|---|---|---|---|
| 1 | 2020 | Wang et al. [5] | Observational, case-control study 58 participants: 22 healthy subjects, 21 patients with erythematotelangiectatic rosacea (ETR), 15 with papulopustular rosacea (PPR) Extraction of DNA from skin samples collected from cheeks of the participants | Both erythematotelangiectatic (ETR) and papulopustular rosacea (PPR) showed a decreased abundance of Cutibacterium (ETR: 27.3%, PPR: 23.3%, controls: 62.6%. Increased Staphylococcus abundance in ETR (23.0% vs. 7.7% in controls). Increased Streptococcus abundance in PPR (9.6% vs. 2.2% in controls). Cutibacterium abundance was significantly reduced in both rosacea subtypes, suggesting a potential protective role against dysbiosis. Increased Shannon diversity (richness and evenness) in the bacterial microbiome of PPR patients compared to controls. |
| 2 | 2020 | Woo et al. [6] | Longitudinal cohort study Patients were prescribed oral doxycycline, 100 mg, twice daily for 6 weeks Samples from skin areas on the cheek and nose 12 Asian subjects with skin phototype 3 (50%), and 4 (50%) on the Fitzpatrick scale. One of the subjects (8.3%) was male and the mean age was 49.2 ±18.6 | Before treatment, the dominant species were Staphylococcus epidermidis (28%) and Cutibacterium acnes (13%). After 6 weeks of doxycycline treatment, the dominant species were S. epidermidis (22%) and Stenotrophomonas rhizophila (8%). In the group aged 60 years and younger, the dominant species were Staphylococcus epidermidis (31%) and Cutibacterium acnes (17%). In the group older than 60 years, the dominant species were Pseudomonas koreensis (33%) and Corynebacterium tuberculostearicum (17%). |
| 3 | 2020 | Caimei et al. [7] | Observational case-control study 28 patients – 14 patients with rosacea (8 with early-stage, 6 with intermediate-stage) 14 healthy controls Microbial samples were collected from the nasal alar and nasolabial folds from all of the participants | The relative abundance of Demodex mites was significantly higher in the rosacea group (1.647 ±0.389%) compared to the healthy group (0.448 ±0.089%). Demodex abundance was higher in intermediate-stage rosacea patients compared to early-stage patients. The relative abundance of Demodex mites was negatively correlated with bacterial abundance and positively correlated with fungal abundance. The relative abundance of Demodex mites was negatively correlated with bacterial abundance and positively correlated with fungal abundance. |
| 4 | 2020 | Rainer et al. [8] | Observational case-control study comparing the skin microbiota of 19 rosacea patients (erythematousangiectatic, papulopustular or both) to 19 matched controls Skin swabs were collected from 2 × 2 area on the nose and bilateral cheeks | PPR showed greater alpha diversity compared to ETR and controls. Depletion of Roseomonas mucosa in ETR. Enrichment of Corynebacterium kroppenstedtii, Campylobacter ureolyticus, and Prevotella intermedia in PPR. The highest relative abundance of C. kroppenstedtii was seen in patients with both ETR and PPR (19.2%) compared to controls (0.19%). |
| 5 | 2020 | Yuan et al. [9] | Pilot study including 25 patients with papulopustular rosacea (PPR), aged 28–60 years Swabs were collected from lesional and non-lesional areas Measurements of transepidermal water loss (TEWL) and skin conductivity were taken from lesional (papules/pustules) and non-lesional areas | Lesional areas in rosacea patients showed higher transepidermal water loss (TEWL) and lower skin conductivity, indicating a compromised skin barrier. Imbalances in Propionibacterium acnes and Staphylococcus epidermidis were linked to altered skin physiology in rosacea. Differences in bacterial communities were observed between lesional and non-lesional areas. |
| 6 | 2021 | Thompson et al. [10] | A cross-sectional, case-control study comparing the skin microbiota of patients with acne, rosacea, and healthy controls Participants: 54 individuals (8 with acne, 19 with rosacea, and age-, sex-, and race-matched controls for each group) Skin microbiota samples were collected from the cheeks and nose using sterile foam-tipped swabs premoistened with Amies medium | Cutibacterium acnes (C. acnes) and Serratia marcescens were significantly enriched in rosacea compared to acne. Actinobacteria was the most abundant phylum in rosacea patients, contrasting with acne patients, where Proteobacteria dominated. Rosacea is associated with a higher density of Demodex folliculorum mites. These mites may either contribute directly to inflammation or act as vectors for bacteria, such as Bacillus oleronius. |
| 7 | 2023 | Xiong et al. [11] | 44 samples of facial microorganisms (17 in the case group and 27 in the control group) The 16S rRNA gene sequences from 44 samples were processed using the UPARSE software | Relative abundance of Cutibacterium acnes was significantly lower than in the control group. In contrast, the mean relative abundance of Staphylococcus epidermidis was higher in patients with rosacea than in the control group. Cutibacterium acnes and Staphylococcus epidermidis may be associated with the pathogenesis of rosacea. |
| 8 | 2023 | Tao et al. [12] | Comparative analysis of the facial microbiome in patients with rosacea, seborrheic dermatitis, and healthy controls Data included 18 rosacea patients, 18 seborrheic dermatitis patients, and 11 healthy individuals Skin samples were taken from the cheeks for DNA extraction and sequencing | The bacterial Shannon diversity index was significantly higher in rosacea patients compared to healthy controls. No significant differences were found in fungal diversity for rosacea patients. Firmicutes abundance was increased, while Actinobacteria abundance was decreased in rosacea patients compared to healthy controls. Cutibacterium: Reduced abundance in rosacea patients (21.7%) compared to controls (63.5%). Streptococcus: Increased abundance in rosacea (23.3%) compared to seborrheic dermatitis (0.6%). |
| 9 | 2024 | Pan et al. [3] | Two-sample Mendelian randomisation (MR) The Skin Microbiome Genome-Wide Association Study (GWAS) Summary Data was derived from 647 participants in two German population-based cohorts, and for the inflammatory skin diseases, they were sourced from the FinnGen consortium 79 bacterial features of the skin microbiota. The study considered bacterial correlations with diverse skin environments (moist, sebaceous, dry) | Specific Staphylococcus species, including uncategorized ones (ASV002 and ASV122), were associated with an increased risk of rosacea. Environmental variability of the microbiota was critical. The same bacterial genus could have different effects depending on its niche (e.g., sebaceous vs. dry skin environments). Some Staphylococcus species from sebaceous environments might protect against certain diseases but increase the risk of others. |
| 10 | 2024 | Ferček et al. [13] | Observational case-control study 35 patients with periocular inflammatory conditions (including 10 with rosacea) 39 healthy controls matched for sex and age Microbial analysis included DNA extraction followed by PCR amplification; analysis included alpha and beta diversity; bacterial taxonomy was assigned (SILVA rRNA database) | The altered skin microbiota in rosacea, particularly increases in Corynebacterium and Bartonella, suggests a potential role of these bacteria in disease pathogenesis. Decreased abundance of Gram-positive anaerobic cocci (Anaerococcus and Finegoldia). |
| 11 | 2024 | Li et al. [14] | Method: Mendelian Randomisation (MR), Weighted Bayesian Analysis (BWMR) Skin microbiome: 1656 samples collected from participants in two German cohorts: KORA FF4 (n = 324), PopGen (n = 273) Summary statistics for rosacea were obtained from the FinnGen genome-wide association study (GWAS). The numbers of cases and controls are as follows: 1,877 cases and 297,544 controls | Finegoldia and Rhodobacteraceae in a moist skin environment were negatively correlated with rosacea. The species ASV023 in a dry skin environment was positively correlated with rosacea. |
| 12 | 2024 | Joura et al. [15] | Oobservational, case-control Molecular microbiology methods (16S rRNA sequencing) Stool, blood and skin samples of 18 rosacea patients in addition to stool, blood and skin samples of 9 healthy individuals | Rosacea patients exhibited significant differences in alpha and beta diversity and in the abundance of specific genera in their skin microbiome compared to healthy individuals. Key genera associated with rosacea skin included Staphylococcus, Cutibacterium, Corynebacterium, and Neisseria. |
| 13 | 2024 | Zhu et al. [16] | A total of 1656 skin samples was acquired from individuals within two German cohorts, KORA FF4 (n = 635) and PopGen (n = 1021) The samples were collected from three skin microenvironments, including moist skin, dry skin, and sebaceous skin Microbial community patterns were obtained through the 16 S rRNA gene | Corynebacterium (ASV004) and the Micrococcaceae family are associated with an increased risk of rosacea (ROS). |
Discussion
The studies reviewed consistently highlight significant alterations in the skin microbiota of patients with rosacea, emphasizing the role of bacterial diversity and specific microbial taxa in disease pathogenesis. Tao et al. reported that the bacterial Shannon diversity index was significantly higher in rosacea patients compared to healthy controls, suggesting an overall increase in microbial richness and evenness. In contrast, fungal diversity did not show significant differences, indicating that bacteria play a more prominent role in rosacea than fungi [12]. Wang et al. similarly observed increased bacterial diversity in rosacea, particularly in the papulopustular subtype (PPR), further supporting the relevance of bacterial imbalance in the condition [5]. Several bacterial genera and species have been identified as key contributors to rosacea. For instance, Staphylococcus species, including Staphylococcus epidermidis, were frequently associated with an increased risk of the condition [5, 6, 11]. Pan et al. demonstrated that specific Staphylococcus species were linked to higher susceptibility to rosacea, especially in sebaceous skin environments, where they might exacerbate inflammation [3]. Similarly, Wang et al. observed an increased abundance of Staphylococcus in erythematotelangiectatic rosacea (ETR) patients compared to healthy controls [5]. Conversely, Cutibacterium acnes, typically dominant in healthy skin, was significantly depleted in rosacea patients across multiple studies, such as those by Tao et al. and Li et al., suggesting a potential protective role against the condition. The loss of this beneficial bacterium might contribute to microbial dysbiosis and heightened skin inflammation [12, 14]. Additional taxa, including Corynebacterium and Streptococcus, were also implicated in the disease. Ferček et al. found increased levels of Corynebacterium in rosacea patients, while Streptococcus abundance was notably higher in the PPR subtype compared to controls and other inflammatory conditions like seborrheic dermatitis [13]. These findings indicate that specific bacterial profiles may not only influence the onset of rosacea but also differentiate its subtypes.
Environmental factors and niche-specific variations also appear to shape the skin microbiota in rosacea. Pan et al. highlighted that the same bacterial genus might exert contrasting effects depending on its location (e.g., sebaceous vs. dry skin environments), underscoring the importance of local skin conditions in modulating bacterial activity [3]. Moreover, studies like that by Yuan et al. demonstrated differences in microbial composition between lesional and non-lesional skin, suggesting that localized microbial shifts contribute to disease severity and progression [9].
The most frequently mentioned pathogens influencing rosacea include Staphylococcus species, particularly Staphylococcus epidermidis, which were consistently found in higher abundance in rosacea patients and are associated with increased inflammation, especially in sebaceous skin environments [3, 9, 11, 15]. Another key bacterium, Cutibacterium acnes, typically dominant in healthy individuals, showed significant depletion in rosacea patients across multiple studies, suggesting that its reduction may disrupt skin homeostasis and promote dysbiosis [6, 10–12, 15]. Additionally, Corynebacterium species were reported at elevated levels in rosacea patients, indicating a potential role in the disease’s pathogenesis [6, 8, 13, 15, 16].
The presence of Demodex mites has been identified as a contributing factor in the development of rosacea. It has been postulated that these mites may function as vectors for bacteria such as Bacillus oleronius [7, 10]. An increased density of Demodex mites has been observed to be a contributing factor in the onset and exacerbation of papulopustular rosacea [17].
These findings emphasise the intricate relationship between microbial diversity, specific bacterial taxa, and environmental factors in the pathogenesis of rosacea. In addition to compositional changes, several studies suggest that the skin microbiome may influence the immune response. Pro-inflammatory microbes, such as Staphylococcus epidermidis, have been observed to activate Toll-like receptor 2 (TLR2), a receptor that is overexpressed in rosacea skin. This activation increases the production of inflammatory mediators, including cathelicidins such as LL-37 [18, 19], thereby contributing to the chronic inflammation observed in rosacea patients [20].
Dysbiosis may also negatively impact the integrity of the skin barrier. Loss of beneficial species such as Cutibacterium acnes may reduce the production of short-chain fatty acids and other metabolites important for barrier function and microbial competition [21, 22]. In parallel, increased colonisation by Corynebacterium and Streptococcus, as observed in various rosacea subtypes, has been linked to skin irritation and altered lipid metabolism [23]. These changes may exacerbate transepidermal water loss and facilitate pathogen access to deeper skin layers, further amplifying inflammatory responses.
With regard to therapeutic implications, most of the reviewed studies did not include interventional data. While some authors have proposed potential benefits of microbiome-targeted approaches – such as topical probiotics or selective antimicrobials (e.g., ivermectin or metronidazole) – there is currently a lack of robust clinical evidence to support their efficacy in rosacea management [24, 25]. Moreover, the long-term effects of such interventions on microbial homeostasis and skin physiology remain uncertain.
Taken together, current evidence underscores the complex interplay between microbial composition, immune activation, and barrier function in rosacea. However, the precise mechanisms underlying these relationships are still insufficiently understood. Future studies should prioritise clarifying how dysbiosis drives immune dysregulation and barrier impairment, and should provide high-quality clinical trials to assess the safety and efficacy of microbiome-targeted therapies.
Conclusions
This systematic review highlights the important role of the skin microbiome in the pathogenesis of rosacea, with bacterial diversity and specific taxa emerging as key contributors to the disease. Patients with rosacea consistently exhibit microbial dysbiosis, characterized by increased bacterial diversity and the enrichment of pro-inflammatory taxa such as Staphylococcus epidermidis, Corynebacterium, and Streptococcus. In contrast, the depletion of protective species such as Cutibacterium acnes suggests a disruption of skin homeostasis and enhanced inflammatory potential. Local environmental factors and niche-specific variations further shape the microbiome’s impact, as lesional skin demonstrates distinct microbial profiles compared to non-lesional areas.
These findings indicate that microbial interactions with the immune system and skin barrier may play a role in rosacea development and progression, although current evidence remains limited. While emerging data suggest that microbiota-targeted strategies – such as probiotics, prebiotics, or selective antimicrobial approaches – could be promising for rosacea management, robust clinical studies are needed. Future research should prioritize clarifying the mechanisms linking microbial dysbiosis with immune dysregulation and generating stronger evidence to guide the development of effective microbiome-based therapies.







