
An 88-year-old patient with a history of coronary artery bypass grafting was referred for transfemoral transcatheter aortic valve implantation (TAVI) because of severe, symptomatic (NYHA III) aortic stenosis with coexisting renal failure and other comorbidities. In echocardiogram, a severely calcified 3-cuspid aortic valve with an aortic valve area of 0.6 cm2 was noted (aortic maximal pressure gradient of 90 mm Hg and mean gradient of 46 mm Hg). The left ventricle (LV) had a small cavity and was concentrically hypertrophied (LVEDD 42 mm, IVSd 15 mm, LVEF 60%). The mitral annulus was moderately calcified. There was mild mitral regurgitation without significant stenosis (mean gradient 3.2 mm Hg, MVA 2.5 cm2). In computed tomography the aortic annulus area was 5.6 cm2. Revascularization was not required.
Because of the high risk of surgery, the patient was scheduled for transfemoral TAVI (Euroscore II 6.1%, logistic Euroscore 35.7%, STS 5.8%).
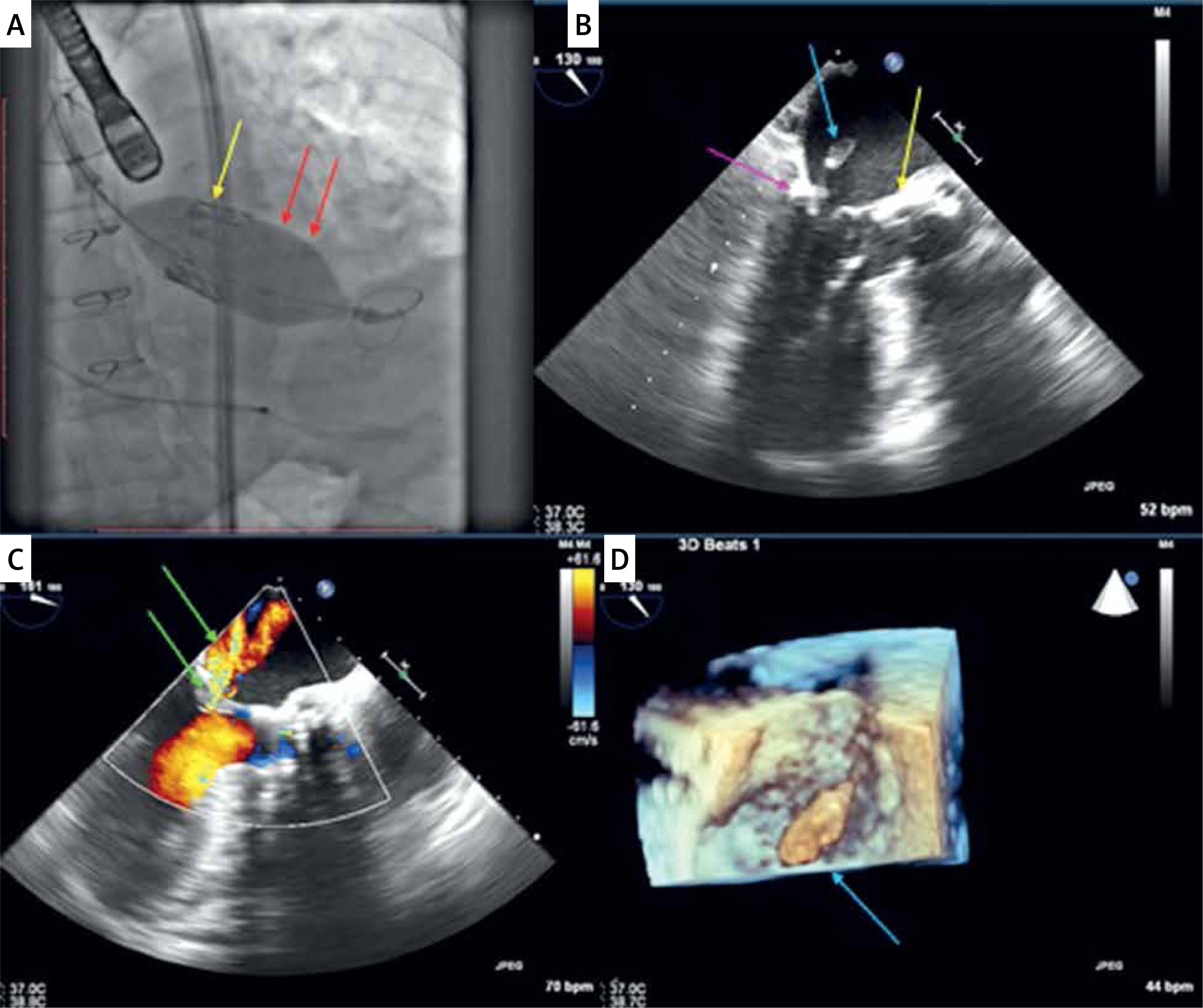
During the procedure, the wire was properly inserted into the LV apex. Successful balloon aortic valvuloplasty was performed. However, during the implantation of an Edwards Sapien XT 29 mm valve, sudden migration of the balloon towards the LV was observed (Figure 1 A). Due to the underexpansion of the valve, postdilatation was necessary. However, during the inflation, the balloon moved slightly towards the LV again. It was immediately deflated, repositioned, and finally the valve was expanded at a low position. Post-procedural routine transoesophageal echocardiography showed good valve function with a mild perivalvular leak. However, a rupture of the papillary muscle was found (Figure 1 B). The papillary muscle was freely swinging between LV and LA and was attached to the chordae tendineae of the A3 mitral segment. Unexpectedly, only moderate mitral regurgitation (Figure 1 C) was observed (VC 3 mm, EROA 0.15 cm2, RV 20 ml). A conservative approach was chosen because the patient was at high risk of surgery and remained stable during 30 min of observation. No other complications were observed. Control echocardiography did not show aggravation of mitral regurgitation (Figure 1 D). The patient was discharged home on the 4th day. Three and 12 months later, echocardiographic and clinical status did not worsen (NYHA III class). Only LV cavity enlargement was observed (LVEDd from 42 mm to 52 mm). Deterioration of the symptoms (NYHA III/IV and dementia) was observed 2 years after TAVI (phone visit). It was the last contact with the patient.
Figure 1
A Fluoroscopy: implantation of TAVI valve (yellow arrow): views of the balloon displaced into the LV (red arrow) and under-expanded valve. B – TEE: ruptured papillary muscle visible in systole in the left atrium (blue arrow - head of the ruptured papillary muscle, violet arrow – calcification of the mitral annulus, yellow arrow – TAVI valve). C – TEE: colour Doppler showing moderate (narrow vena contracta) mitral regurgitation (green arrow – colour Doppler of mitral regurgitation). D – 3D TEE: ruptured papillary muscle visible in systole in the left atrium (blue arrow – head of the ruptured papillary muscle)
Papillary muscle rupture is a very rarely reported but potentially catastrophic complication of TAVI. Migration of the large balloon to the small hypertrophic LV can damage the mitral apparatus.
Such a complication could have 2 mechanisms. The first may occur when the guidewire crosses between the chords of the mitral apparatus and the rapid balloon’s inflation pulls the papillary muscle. However, in this situation, the passage of the guidewire through the mitral subvalvular apparatus increases mitral regurgitation, which was not observed. The second is mechanical damage of the muscle by the balloon nosecone moved into the LV. It may occur especially in a small, hypertrophic cavity, like in our patient.
Papillary muscle rupture usually causes severe consequences, but because of the narrow, calcified mitral annulus and only partial muscle rupture, the mitral regurgitation may be moderate and in selected patients treated conservatively [1–4].







