
A 64-year-old patient with dilated cardiomyopathy (DCM) and chronic heart failure with reduced ejection fraction (HFrEF), with an implanted cardioverter-defibrillator, was admitted to the cardiology unit due to consecutive acute heart failure (HF) decompensation. Regardless of potent optimal pharmacotherapy, at admission, the patient was in NYHA class 4.
Transthoracic echocardiography (TTE) revealed severe dilatation with significantly reduced left ventricle (LV) systolic function (EF LV – 10%). A combined aortic valve (AV) disease in the form of moderate stenosis and regurgitation was revealed. Morphologically aortic leaflets were calcified, peak velocity in continuous wave (CW) was V max. 1.8 m/s, in colour Doppler (CD) the width of the valve insufficiency – jet 8 mm, the width of the left ventricular outflow tract (LVOT) – 19 mm, pressure half time (PHT) 380 ms. Transesophageal echocardiography (TEE) confirmed the presence of a complex AV defect (AVA planimetric – 1.5 cm2, AR – jet 8 mm, LVOT – 18 mm, EDV in descending aorta – 20 cm/s) (Figure 1). The evaluation of AV morphology revealed a bicuspid AV (BAV): fusion of the right coronary cusp (RCC) and the left coronary cusp (LCC) – fusion flap: still and calcified.
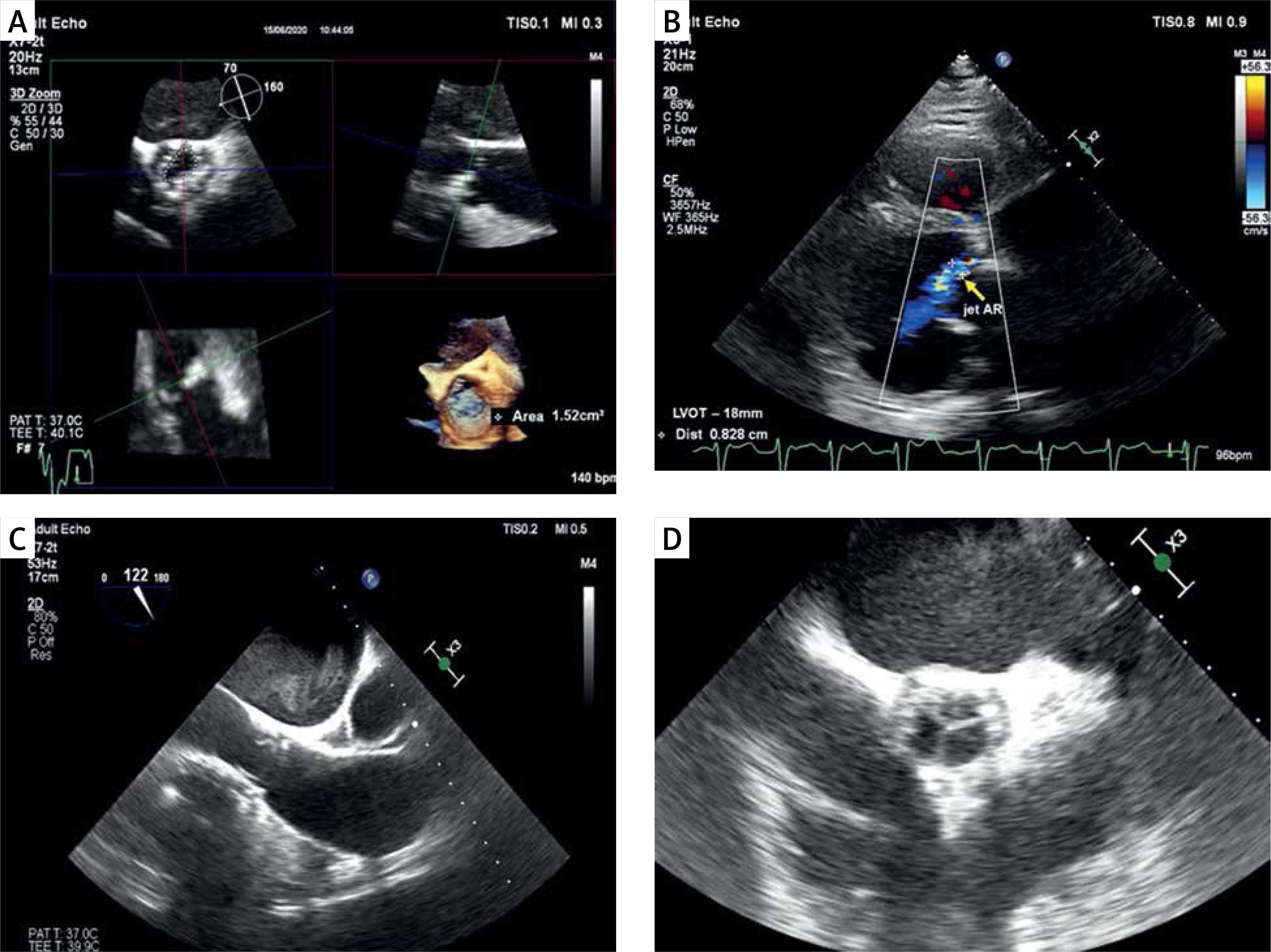
Figure 1
Transesophageal echocardiography: A – AVA planimetric in 3D reconstruction (AVA – 1.52 cm2), B – aortic regurgitation in TEE (jet AR – 8 mm, LVOT – 18 mm), C, D – valve prosthesis Edwards-Sapien 3 Ultra (29) – after procedure TAVI in TEE (long axis view – C), (short axis view – D)
Due to the worsening of clinical status and signs of LV low output, the pharmacotherapy was intensified. To qualify the patient for heart transplantation (HTX)/biventricular support, right heart catheterization (RHC) was performed. Based on RHC results (mPAP – 48 mm Hg, PVR – 6.85 Wood units, CO – 2.48 l/min, CI – 1.1 l/min/m2) precapillary pulmonary hypertension (PH) was diagnosed. It was a reason for the patient’s disqualification from HTX.
Considering the coexisting complex BAV pathology, the patient was consulted by the Heart Team – due to the significant risk of death (EUROSCORE II – 8.2%), he was disqualified from the classical aortic valve replacement and was qualified for transcatheter aortic valve implantation (TAVI) as a life-saving procedure.
The procedure was performed under local anaesthesia by the multidisciplinary TAVI team. A balloon-expandable valve prosthesis Edwards-Sapien 3 Ultra (29) (Edwards Lifesciences Corp., Irvine, CA, USA) was implanted. The result was satisfactory (implantation depth correct, no occlusion of coronary arteries, no tamponade and no paravalvular leak).
After the TAVI, the patient was significantly improved, which allowed the intravenous treatment to be stopped and the HF standard pharmacotherapy to be optimized. TTE showed normal aortic prosthesis function, regression of LV volume (EDV from 341 ml to 290 ml) with persistently reduced LV systolic function (LVEF 17%). Laboratory tests showed a significant decrease in NT-pro BNP, and normalization of hepatic and renal parameters. The follow-up RHC confirmed significant regression of PH indices (mPAP – 35 mm Hg, PVR – 4.0 Wood units, CO – 3.83 l/min, CI 1.82 l/min/m2), and finally, he was qualified for HTX. Currently, he is in a stable state, waiting for further proceedings.
Currently, the indications for TAVI are increasing (AHA 2020); however, standard TAVI procedures are indicated for high-risk patients with severe symptomatic aortic stenosis.
We present successful, nonstandard use of this method in end-stage HF in the case of DCM and moderate BAV disease. Normalization of AV function due to the TAVI procedure allowed for PH regression and constituted a bridge to HTX [1–3].







