
An 82-year-old woman with a history of hypertension, type 2 diabetes mellitus, myocardial infarction, ischaemic stroke and amputation of both lower extremities was admitted with the symptoms of evolving anterior wall myocardial infarction (STEMI). Coronary angiography performed with a right radial approach revealed critical stenosis in the mid-portion of the left descending coronary artery (LAD) and 75% lesion in the right coronary artery (RCA). The attempt of crossing the culprit lesion in the LAD was unsuccessful due to the calcified and tortuous anatomy of the vessel. In the next hours the chest pain subsided and ST segment elevation in ECG resolved. Two days later the second attempt of crossing the LAD lesion was made. The patient had been diagnosed with Leriche syndrome, so the procedure was performed by right brachial access – a right radial approach was rejected because of haematoma and a small tumour found at the site of previous puncture of that artery. Using the Fielder XT-R wire, microcatheter and rotational atherectomy, successful treatment of LAD/D1 with one drug-eluting stent (DES) implantation was done. The next day after the procedure Doppler ultrasonography of the forearm was carried out and revealed pseudoaneurysm of the radial artery. It was atypical and had unusual anatomy – it consisted of three connected cavities. The first one, 17.7 × 10.2 mm, was located exactly in the site of the artery puncture and was communicated by a narrow, 5 mm long “neck” with the artery and at the opposite side to the next chamber, 13.7 × 24.2 mm, located more proximately in the forearm. The third in the chain, 28 × 9 mm, beam-shaped chamber was connected to the second one and showed no flow. The two “last” chambers were partially occluded by the organizing clot. The peripheral blood flow in the radial artery was not disturbed and the vessel remained patent. Moderate haematoma of the forearm was present and it seemed to increase over the days. Apart from the tumour, a murmur in the area of artery puncture was heard. Because of favourable anatomy (tight “neck” between the cavity and artery) we injected in local anaesthesia 400 IU of thrombin into the first chamber of the pseudoaneurysm. This resulted in effective flow stop in the whole chain of cavities. The embolization procedure was monitored with Doppler technique and did not cause any ischaemic complications in the hand. Follow-up examinations repeated in the following days showed normal flow in all arteries of the extremity and complete exclusion of multichambered pseudoaneurysm (Figures 1–5).
Figure 1
Three successive chambers of the pseudoaneurysm with their dimensions
A – first chamber, B – second chamber, C – third chamber, RA – radial artery.
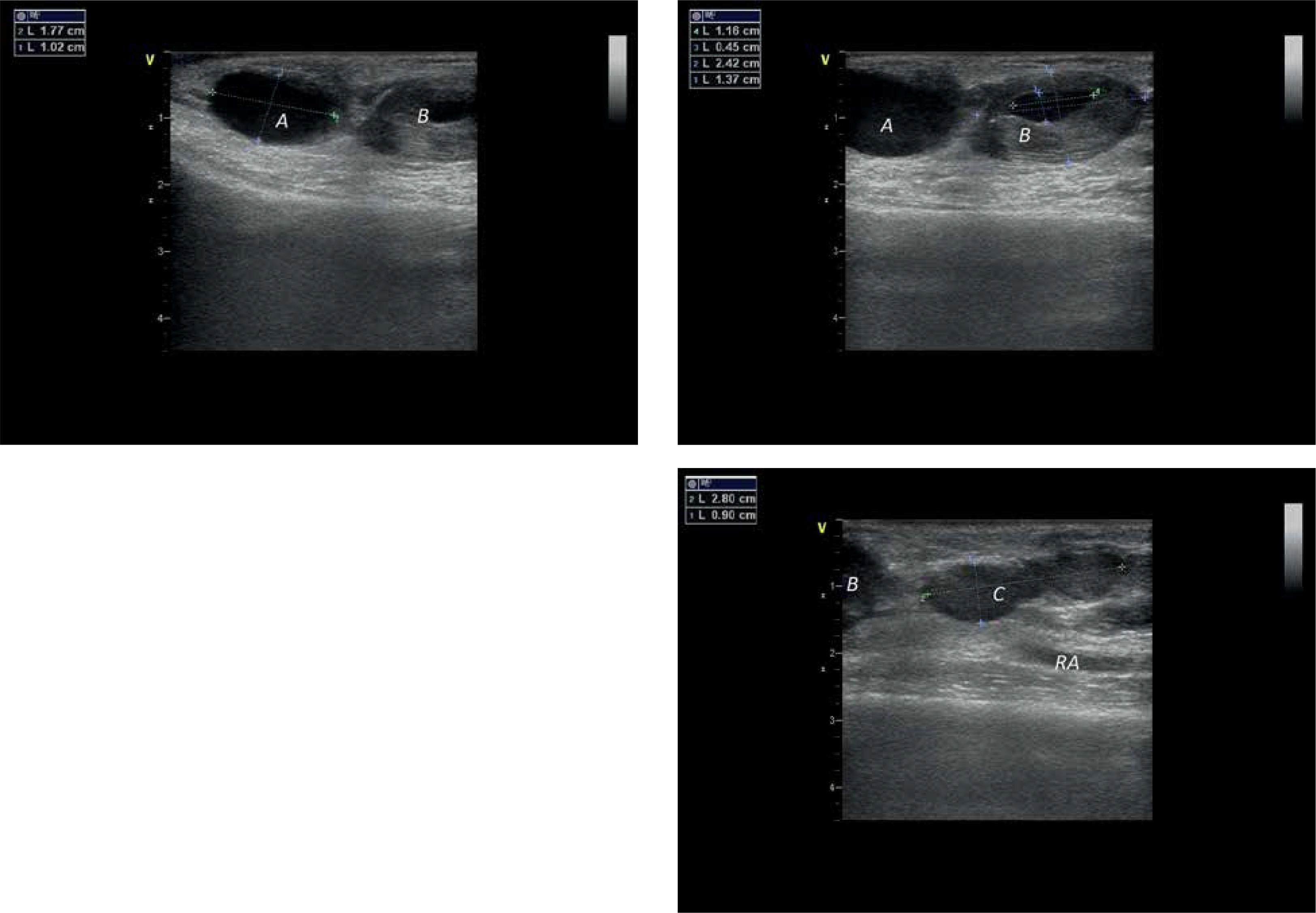
Figure 2
Pseudoaneurysm entry with blood outflow from the radial artery and patent distal part of a vessel
A – first chamber, B – second chamber, RA – radial artery.

Figure 3
Communication between the first and second chamber
A – first chamber, B – second chamber, RA – radial artery.
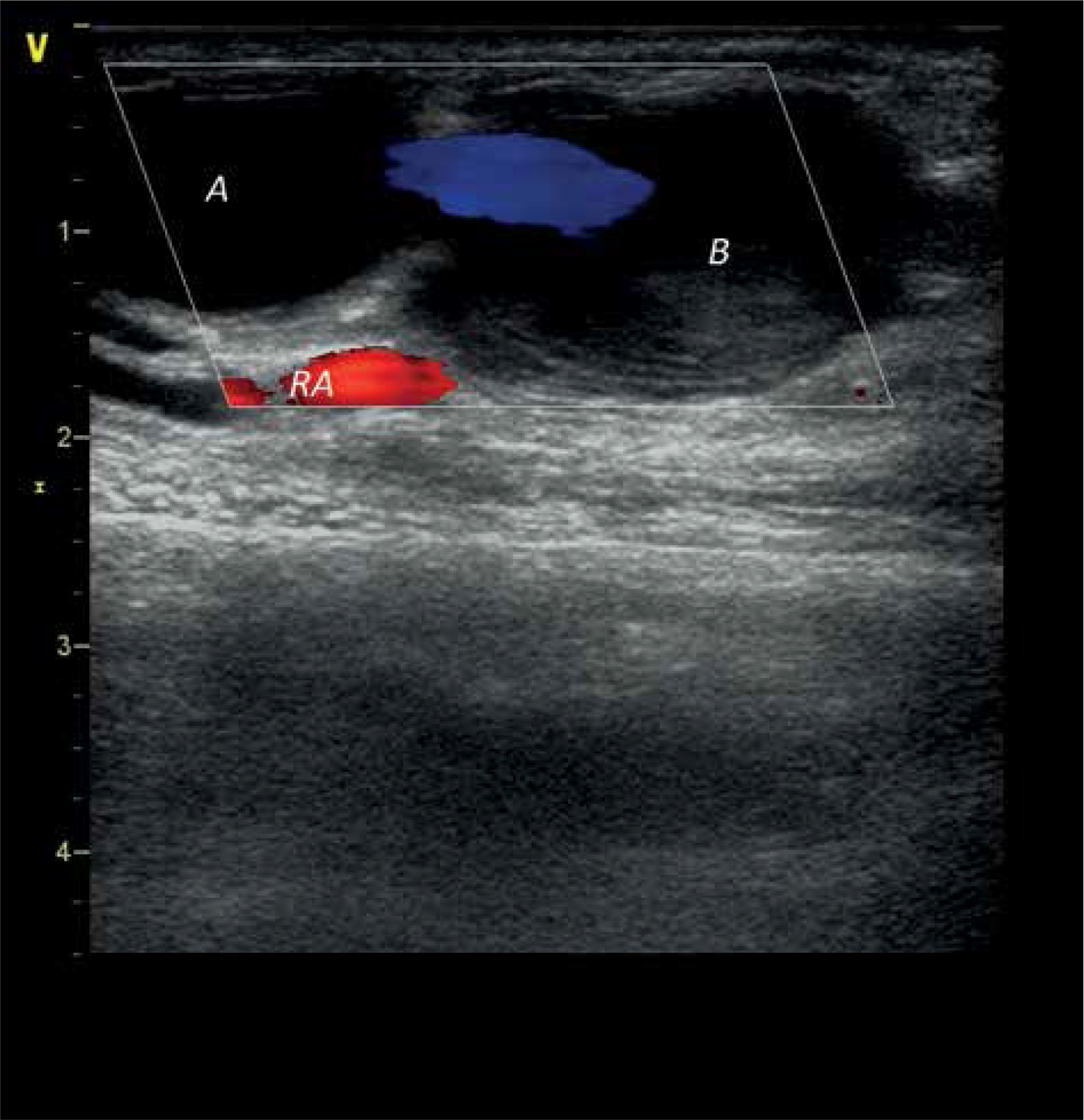
Figure 4
Communication between the first and second chamber with a flow characteristics
A – first chamber, B – second chamber.
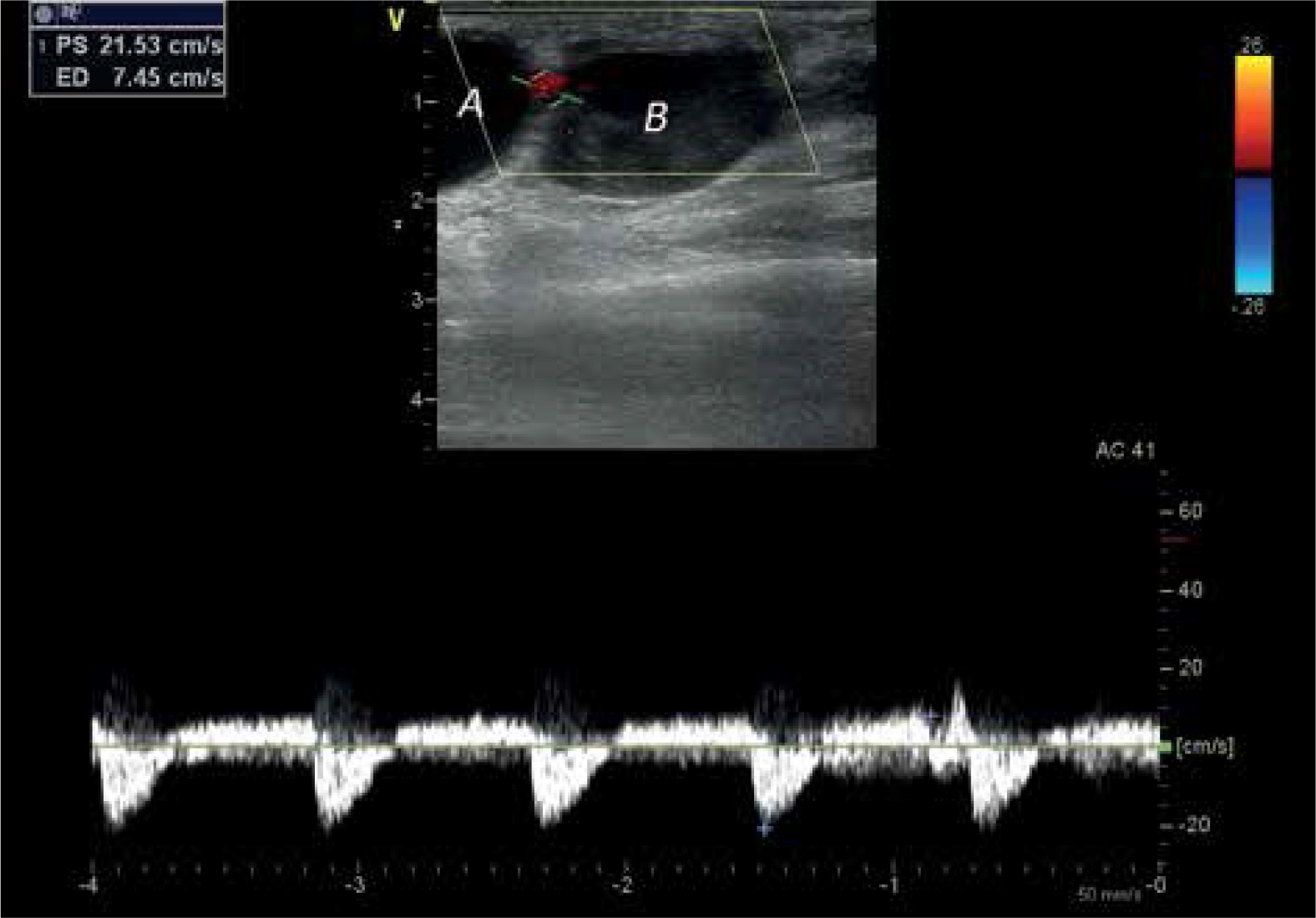
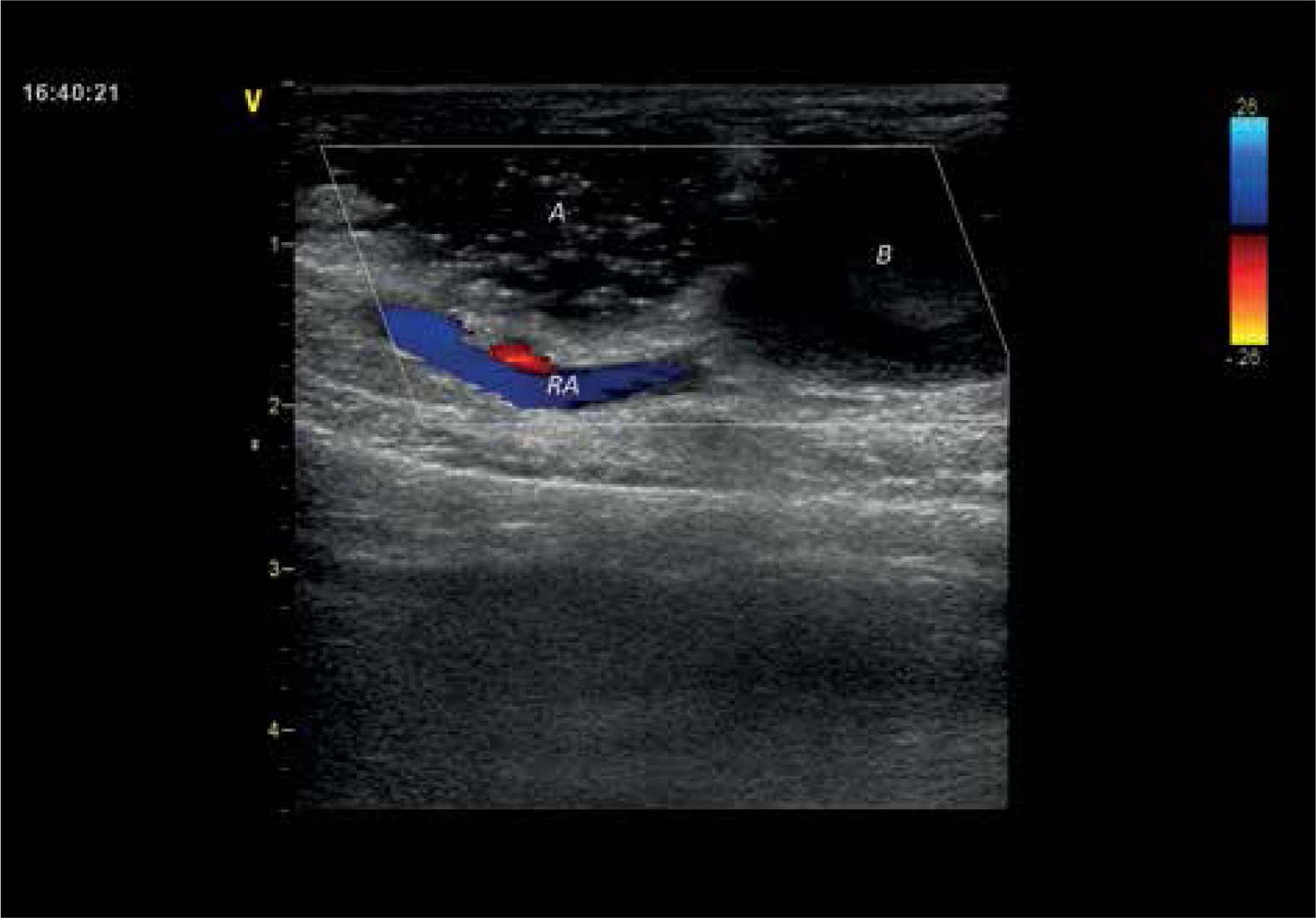
Figure 5
Effect of thrombin injection resulting in complete flow stop by clot filling first of the chambers
A – first chamber, B – second chamber, RA – radial artery.
Pseudoaneurysm is a rare complication occurring with incidence ranging between < 0.1% and 1% of radial procedures. In most cases it does not have an impact on hand function, does not result in more serious complications and may be treated conservatively [1–3]. Possible treatment methods include ultrasonography-guided compression, embolization and surgery. In our case the first of these techniques was relatively contraindicated, because of haematoma of the forearm which potentially could increase during compression. Surgery, although more invasive, would be an alternative option.







