
Introduction
Menopause is experienced by approximately 1.5 mil-- lion women each year [1], and according to a meta- analysis covering studies with data from 6 continents, the average natural age of menopause in the world is between 46 and 52 years old [2] – more specifically in Latin America with an average of 46.5 ±5.8 years [3]. This process involves somatic-vegetative, psychological, and urogenital symptoms [4], and although symptoms related to the urogenital aspect are not frequently reported, they have a negative and significant impact on women’s health and quality of life, with 83% showing vaginal dryness, 30% urinary incontinence, and 42% pain during sexual intercourse [5–7].
The transition from menopause, characterized by hormonal, physiological, and social changes, is often associated with sexual dysfunction, and the physiological mechanism that affects sexual health involves declining gonadal steroid hormone levels, which have an impact on vaginal elasticity and secretion, resulting in vaginal atrophy and pain during sexual intercourse [8, 9]. In addition, these hormonal changes also make it difficult to fill the blood vessels around the vagina, which are crucial for proper lubrication and excitation, triggered by reduced blood flow to the sexual organs [10, 11]. Therefore, discomfort caused mainly by pain during sexual intercourse is reported, resulting in a decrease in sexual practice at this stage [12].
The decrease in sexual practice in this phase has its negative effects, because it generates discomfort and changes the psychological aspect of women, causing mental and emotional disorders and interpersonal suffering, compromising quality of life and inducing a decline in general health [13, 14]. Thus, considering the lack of studies involving this theme, it is believed that it is important to identify aspects related to the absence or presence of sexual practice in menopause, so that health professionals can guide interventions that contribute to better coping with this phase of life. Furthermore, it is considered relevant to direct actions of assistance to the population because sexual activity is considered an important marker for well-being [14]. Thus, the aim of this study was to analyse a possible association between menopausal symptoms (somatic- vegetative, psychological, and urogenital) and sexual function with the maintenance of sexual activity for women in menopause.
Material and methods
Study type and participants
This cross-sectional study followed the recommendations of STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) [15]. Women were included who obtained a positive score on the menopause rating scale (MRS) questionnaire [16], in early post menopause (up to 6 years in amenorrhoea [17]), and serum follicle stimulating hormone (FSH) levels ≥ 25 IU/ml [17]. Those who used stabilization therapy were excluded from the study, as well as woman who were in late post-menopause (after 7 years in amenorrhoea), comprising a total of 96 menopausal women aged 40 to 59 (52.88 ±4.05) years living in the region of Florianópolis (SC) in southern Brazil.
Procedures
The recruitment of participants took place from October 2019 to February 2020, in which participants were recruited through advertisements in print and electronic media, subsequently filling out the MRS questionnaire online through Google Docs. Those with a positive score for symptomatological menopausal women were invited for blood collection in order to check FSH levels, performed by a biochemical professional in February 2020 at a higher education institution.
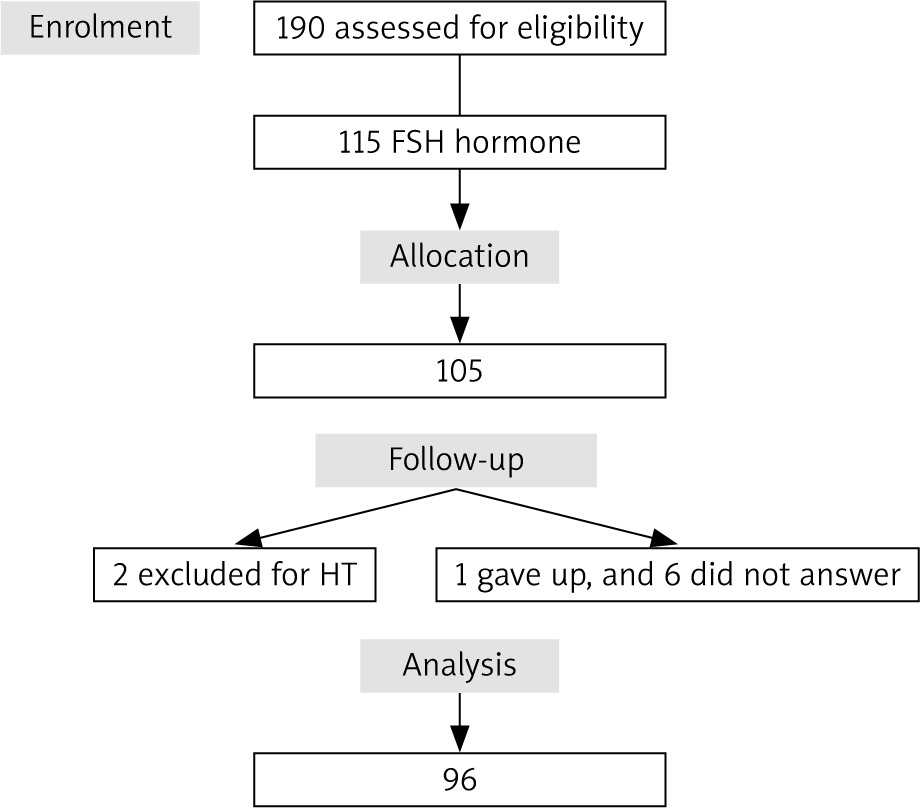
All women filled out a Free and Informed Consent Form. The study followed the recommendations and guidelines of the Declaration of Helsinki and was approved by the UDESC Ethics Committee on Human Research (CEPSH) (Protocol 3.672.933). A total of 190 wo- men were recruited by the media, and of these all had a positive score for symptoms by MRS. In the next stage, which was blood collection, only 115 women with symptoms were available and interested in participating. Of these, 105 had FSH levels ≥ 25 IU/ml. Two women were excluded for using hormone replacement therapy, and one withdrew from the study. After recruitment, data collection was performed by Google Docs, in which the researchers responsible for the Research Laboratory for Leisure and Physical Activity – LAPLAF/CNPq, sent the questionnaire links via email and/or WhatsApp to the participants, according to the preference of each one. The menopause rating scale took around 5 minutes to complete, and the clinical questionnaire took approximately 15 minutes.
Finally, in the collection of the study questionnaire, 6 women did not answer, totalling 96 participants, as shown in Figure 1.
Instruments
Individual online survey using Google Docs:
sociodemographic aspects: economic level, verified through the criterion of the Brazilian Institute of Geography and Statistics, which classifies the population into 5 economic strata by means of monthly family income, adopting the 2019 minimum wage as a base in the value of R$ 998.00; marital status (living together – married/in a stable relationship; living separately – widow/divorced/single); education (up to higher level). The economic level and education were categorized in 3 strata for analysis in the tests, being for the economic level: a) up to 4 minimum wages, b) 5–20 minimum wages, c) more than 20 minimum wages. For education: a) basic education, b) high school, c) higher education;
clinical aspects: sexual activity (yes/no); presence of diseases (yes/no); contraceptive use (yes/no), tobacco use (yes/no); type of menopause (natural or surgical), menarche age (years), age of menopause (years) and practice of physical activity (yes/no).
Menopause symptoms were investigated using the MRS [16], composed of 11 questions, developed in Germany, and validated in Brazil [4], which scores in one scale from 0 (absence of symptoms) to 4 (most severe) and divided into 3 domains: somatic-vegetative, urogenital, and psychological symptoms. The variation in the total score was zero (asymptomatic) and 44 (the highest degree of complaints); the higher the total score in the questionnaire, the greater the severity of symptoms.
Sexual function was investigated using the female sexual function index (FSFI) questionnaire to assess the FSFI in Brazilian women by Rosen et al. [18], translated, validated, and culturally adapted for Brazil by Thiel et al. [19]. The female sexual function index is a 19-question questionnaire that assesses 6 domains: sexual desire, arousal, vaginal lubrication, orgasm, satisfaction, and pain. Each domain indicates scores, and the answer options are classified 0–5 in an increasing way regarding the occurrence of the questioned function. In the pain domain the score is inverted. When adding the scores for each domain, each must be multiplied by a factor that homogenizes the influence of each domain, reaching the total score. The total score varies from 2 to 36, and the higher the final score, the better the sexual function. Menopause symptoms were investigated using the MRS [16], composed of 11 questions, developed in Germany, and validated in Brazil [4], which scores on a scale from 0 (no symptoms) to 4 (most severe) and divided into 3 domains: somatic-vegetative, urogenital, and psychological symptoms. The variation in the total score is 0 (asymptomatic) and 44 (the highest degree of complaints); the higher the total score on the questionnaire, the greater the severity of symptoms.
For statistical purposes, women were analysed according to whether or not they practiced sexual activity (yes/no).
Statistical treatment
The data were analysed using descriptive and inferential statistics. In the descriptive analysis, measures of central tendency (median), dispersion (interquartile ranges), and absolute and relative frequencies (%) were verified. For comparison between groups (sexual activity), the independent χ2 test was used to analyse clinical aspects. The normality of the data was verified using the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to compare the medians of the overall score, and the domains of menopausal symptoms and sexual function with the practice of sexual activity. A multiple linear regression model was also applied to verify the association between the practice of sexual activity and the general score of menopausal symptoms, considering the type of menopause as a variable for control of the analysis. The software used was SPSS version 20.0, and the level of significance adopted was 5%.
Results
The sociodemographic aspects of the study participants were homogeneous, with no difference between groups (sexual activity [yes/no]), i.e. similar groups, in which the average age of menarche was 12.6 years (1.61), and the average age of menopause was 48.03 years (4.5). In addition, as participants who practiced sexual activity, they earned 1–4 rewards (56.5%), studied up to higher education (62.3%), lived together with a partner (81.2%), and were not net (95.7%). Regarding previous physical activity, most had already practiced (97.1%), for more than 10 years (34.8%), at some point in their practical life (76.8%), and some only during school (24.6%) (data not required).
The average overall score of women in the MRS questionnaire was 22.65 (7.53) points, with the participants who maintained sexual activity gaining 21.1 (7.3) points, and 26.5 (6.7) for those who did not engage in sexual activity, i.e. for women had severe symptoms in the MRS score.
Table 1 shows that the participants were homogeneous regarding clinical characteristics, with no differences between the variables, but it is interesting to note that 96.3% of those who did not engage in sexual activity had severe symptoms.
Table 1
Clinical characteristics of the participants according to the practice of sexual activity (n = 96)
When comparing the medians of the domains of menopausal symptoms with the practice of sexual activity, it was observed that those who reported the maintenance of sexual activity had lower medians in the somatic-vegetative (p < 0.001) and psychological (p = 0.006) symptoms, as well as in the general score (p = 0.001), as shown in Table 2.
Table 2
Comparison of medians of domain scores with menopausal symptoms with sexual activity (n = 96)
Furthermore, when the medians of the domains of the FSFI questionnaire, which analyses the sexual function of menopausal women, were compared, those who reported practicing sexual activity had better sexual function in 4 domains (p < 0.005): excitement, lubrication, orgasm, and pain, and in the total score to the questionnaire (p < 0.005). Women who did not engage in sexual activity scored higher in the desire domain compared to those who did (p = 0.001). An increase in sexual desire is perceived here due to the absence of its practice among the participants (Table 3).
Table 3
Comparison of medians of the scores of the Female Sexual Function Index questionnaire domains with sexual activity (N = 96)
When performing the multiple linear regression analysis by the general score of menopause symptoms, with the practice of sexual activity and the type of menopause as controls of the analysis, it was found that, regardless of the type of menopause (surgical or natural), women who reported not engaging in sexual activity had a score of 5.651 (p = 0.004) more points in the MRS questionnaire compared to those who engaged in sexual activity. This shows that the maintenance of sexual life in this period predicts the variation in the MRS score by 10.4%, as shown in Table 4.
Discussion
The aim of this study was to analyse the possible relationship between menopausal symptoms (somatic-vegetative, psychological, and urogenital) and sexual function with the maintenance of the practice of sexual activity in menopausal women. A positive relationship was observed in the practice of sexual activity in the reduction of menopausal symptoms, highlighting somatic- vegetative, psychological, and sexual function, compared to those who did not engage in sexual activity. The association found here in other published scientific reports is unknown.
When analysing sexual function, the cut-off point for the total score of the FSFI questionnaire is 26 points [20], with values equal to or below this point indicating sexual dysfunction. In general, the study participants had good sexual function with a median of 26.8 points. And those who did not engage in sexual activity had a much lower score (15.2 points). For comparison with another study using this questionnaire with middle aged women in Latin America [21], the score was 27.2, being similar to the current study. In a Spanish study, the median score was lower, at 24.7 points [22]. This study with Spanish women did not investigate whether or not women practiced sexual activity; however, the sample was well distributed regarding marital status, comprising 55.7% of married women, and 44.3% for single women, unlike the study of Mezones-Holguin et al. [21] and the current study, where a large part of the sample comprised married women, enabling a more active sex life and consequently a higher score on the FSFI questionnaire.
Corroborating a Brazilian cross-sectional study carried out with a sample of 370 middle-aged women [23], in which it sought to assess the influence of climacteric symptoms on the sexual function of the participants, 67% of the women were at risk of sexual dysfunction – a higher percentage when compared to the present study, in which 56.3% of the participants were at risk of sexual dysfunction. It is noteworthy that the present study sought to analyse the sexual activity of the participants, where a large part of the sample practiced sexual activity (71.9%), which may justify a lower percentage of participants at risk of sexual dysfunction.
Because the sample comprised 71.9% of sexually active women, sexual function was statistically significant in the areas of arousal, lubrication, orgasm, and pain, in addition to the total score on the FSFI questionnaire (p < 0.005), i.e. those who practiced sexual activity showed a better sexual function in these 4 domains and in the total score compared to those who did not practice. Only the desire domain was statistically greater in those who did not engage in sexual activity (p = 0.001), with no statistically significant difference between groups in the satisfaction domain alone. In addition, in the analysis of multiple linear regression, those who did not practice sexual activity had a score almost 6 points higher on the MRS, i.e. practicing sexual activity in this period predicts a reduction in symptoms better than the type of menopause (natural or surgical).
These data show the relevance of maintaining the practice of sexual activity in reducing the symptoms of menopause, although in climacteric due to oestrogen deficiency there is a loss of elasticity, reduced lubrication, vaginal dryness, and consequently, pains caused by the urogenital symptom [24–26]. Thus, it is necessary that health professionals assist women with their doubts about the physical changes that will occur during menopause, and most importantly, how to deal with them. Therefore, it is extremely important to look for integrative ways to prevent, reduce, and treat sexual dysfunctions resulting from this phase of life, aiming at maintaining the sexual life of these patients [27, 28].
The literature shows that menopausal symptoms are less intense in those who exercise regularly [29]; in addition, kinesiotherapy helps strengthen pelvic floor muscles, contributing to the improvement of dysfunctions [30], and information on sexual physiology and anatomy, with Kegel exercises and vaginal dilation, proved to be effective for sexual dysfunctions [31]. All this evidence could make up a specific clinical intervention protocol to help women overcome menopausal difficulties.
However, it is important to note that the study had a small sample size (only 96 postmenopausal women), which introduces certain limitations to the study, and it is important to consider this potential bias when interpreting the findings. It becomes more challenging to control for confounding factors adequately, there is a possibility of selection bias as the study participants may not be fully representative of the broader population of menopausal women, and small sample sizes can reduce the statistical power of the study, potentially leading to an increased risk of type II errors. Finally, there may be additional factors influencing the relationship between menopausal symptoms, sexual function, and sexual activity that were not accounted for in this study.
Potential clinical value
Given the lack of previous studies on the practice of sexual activity in relation to the deleterious effects of menopause in middle-aged women, future and longitudinal research should investigate its relationship with menopausal symptoms and with sexual function to produce more definitive and generalizable conclusions.
These results have positive implications for the emergence of strategies and new protocols to be developed by professionals in the field that encourage the maintenance of the sexual life of these women in the treatment of menopausal symptoms, which should aim to reduce somatic-vegetative, psychological, and urogenital symptoms in middle-aged women. Such strategies and/or protocols can be effective in increasing sexual function and reducing the deleterious symptoms of menopause.
Finally, while this study appears to confirm that sexual function and somatic-vegetative and psychological symptoms can be improved by maintaining sexual life among middle-aged women, this was only a cross-sectional study. Research with more representative samples and research with longitudinal study designs are recommended to confirm the results found here and justify the creation of a specific protocol to stimulate the maintenance of sexual life for patients in these conditions.
Conclusions
Menopausal women who keep their sex lives active had a lower score on the menopause symptoms score, specifically in somatic-vegetative, psychological, and total MRS scores, and better sexual function in 4 domains: arousal, lubrication, orgasm, and pain, and also in the total score of the FSFI questionnaire in relation to those who did not practice sexual activity; hence, practicing sexual activity seems to have positive implications for the symptoms and function of sex among menopausal women.
In addition, maintaining sexual activity seems to have a greater impact on reducing menopausal symptoms than the type of menopause (natural or surgical), where participants who reported not engaging in sexual activity had a score that was 5.651 points higher on the MRS questionnaire compared to those who engaged in sexual activity. This shows that the maintenance of the practice of sexual activity predicts the variation in the MRS score by 10.4%. Specific sexological clinical protocols that can stimulate the maintenance of sexual practice among these women during this period are necessary.
However, we emphasize the need for future studies with more diverse and larger populations to confirm the observed relationships; our study has a limited generalizability of the findings due to the small sample size.








