
Introduction
Colorectal cancer is the third most common malignancy in Poland, after breast and lung cancer in women and lung and prostate cancer in men. According to National Cancer Registry data from 2013, this type of cancer accounted for a total of 12.2% of malignancies in men and 10.1% in women. It is worth mentioning that during the last four decades an increasing trend in morbidity and mortality due to this cancer has been observed. In 2014 a total of 18,000 new cases of colorectal cancer were diagnosed, and it was the cause of more than 11,000 deaths, nationwide. In comparison with 1980, the morbidity rate is more than four times higher in men and it is three times higher in women [1, 2].
The mortality rate for colorectal cancer in Poland is much higher than in Northern and Western Europe [3]. In Europe considered as a whole, higher mortality rates for colorectal cancer are only found in the Czech Republic and Hungary. Even if this data is devastating due to constantly high mortality rates, colorectal cancer is characterised by the highest survival among all cancers of the digestive system [4].
Aim
The aim of the study was to assess the occurrence of metastases to regional and distant lymph nodes in patients diagnosed and treated surgically due to colorectal cancer in the nearest geographical region. The results were analysed based on individual factors like age, sex, and body mass index (BMI), comparing to clinical and pathological examinations. Correlations between lymph node metastases and physical symptoms as well as between them and CA19-9 and CEA marker levels were then assessed and subjected to statistical analysis.
Material and methods
The study involved 100 patients treated surgically for colorectal cancer in the 2nd Department of General and Gastroenterological Surgery of the Medical University in Bialystok in the years 2009–2010. There were 56 men and 44 women in the study group. The mean age of the study group was 67.09 years, and the median was 69 years. The youngest patient in this group was 26 years old, while the oldest was 89.
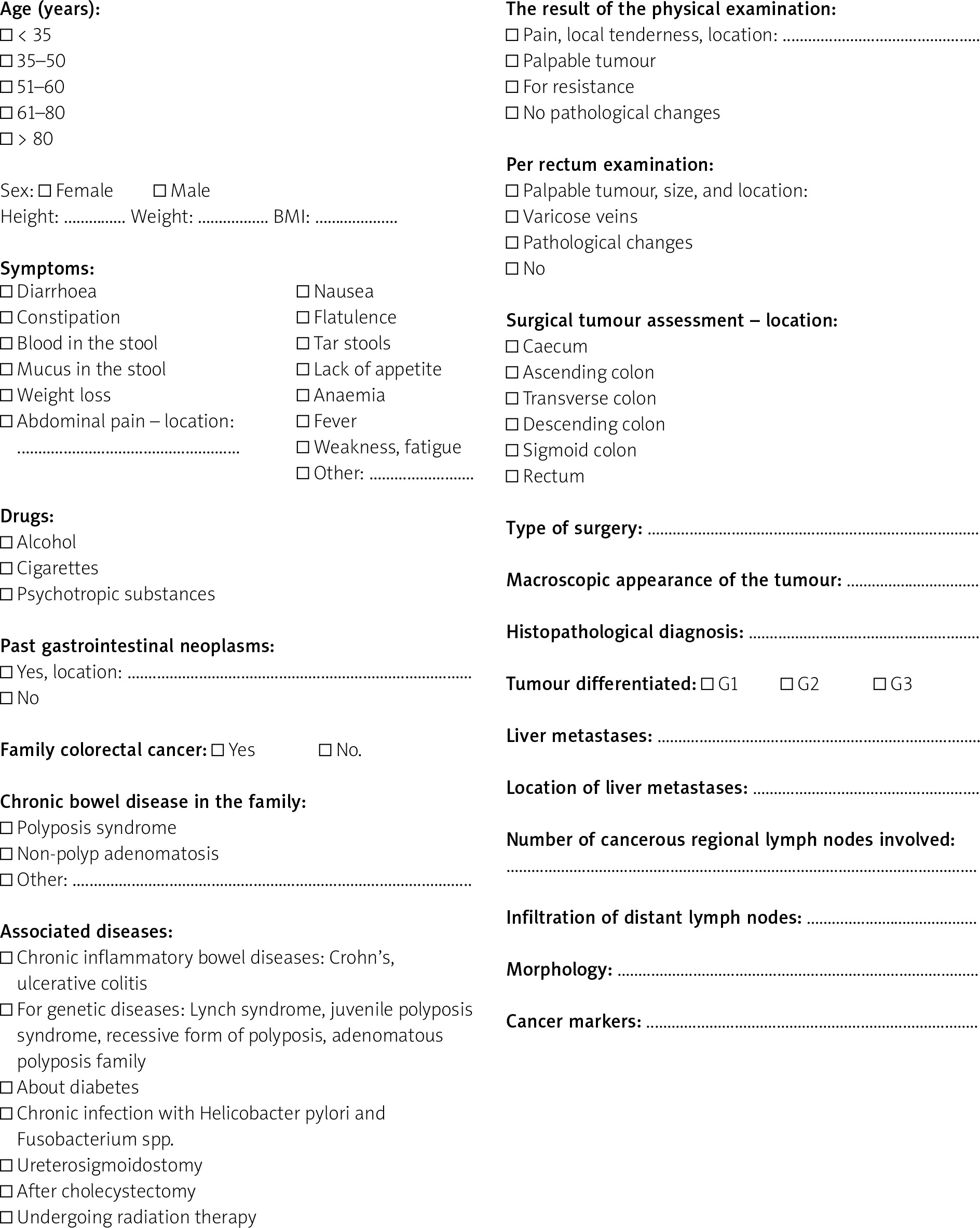
The study was carried out on the basis of medical records (medical history and results of laboratory tests). The research tool was a data collection Questionnaire, which was developed specifically for the purpose of this study.
Results
Metastasis in regional lymph nodes was found in 42% of patients from the study group. Distant metastases occurred in 16% of those cases. Hepatic metastases were diagnosed in 20% (35% of changes in the left lobe, 30% in the right lobe, 30% in both lobes, and 5% between lobes); no statistically significant relationship was found (p > 0.05). The largest group among patients with metastases to regional lymph nodes were patients aged 61–80 years (59.52%). In the group of patients without metastases to regional nodes, the percentage in particular age groups was similar. There were no statistically significant relationships between age, number, and location of metastases (p > 0.05).
Histopathological examination of the primary tumour showed that among the study group there were 94% of adenocarcinomas, 3% of low-differentiated cancers, 2% of adenocellular carcinomas, and 1% of spindle-cell carcinomas. In terms of grading, moderately differentiated or G2 cancers were found most frequently (93%). Poorly differentiated cancer affected 6% of patients, whereas well differentiated lesions were found only in 1% of the study group.
Further pathological evaluation of the primary tumour (pT feature in TNM, according to the 7th TNM staging manual edition) allowed us to find out that 77% of primary tumours were classified as stage T3, 14% as T2, 5% as T4a, 2% as T1 with infiltration limited to the submucosal tissue, and 2% were described as T4b. Primary tumour assessment did not show a statistically significant relationship with the presence of metastases to regional lymph nodes (p > 0.05).
The largest group were patients with cancer located in the sigmoid colon (30 cases), rectum (29 cases), and caecum (16 cases). In addition, in 3 patients bilocation of primary tumour was diagnosed (caecum and ascending colon – 1 patient; caecum and sigmoid – 2 patients). In 2 cases the tumour was located in the descending colon, and in the next two it lay within the splenic fold. There was no statistically significant correlation between tumour localisation and lymph node metastases (p > 0.05).
The mean BMI body mass index in the study group was 26.06 kg/m2. The lowest BMI was 13.14 kg/m2, and the highest was 37.8 kg/m2. Most of the patients in the study group had normal BMI (18.5–24.9 kg/m2, 42%), and only 3% presented body mass deficit. There were no statistically significant correlations in BMI among metastatic and non-metastatic patients (p > 0.05).
Only 2% of respondents reported a congenital character of cancer, including 1% of rectal cancer in the mother and 1% of stomach cancer in the father.
The coexisting diseases among the patients were: arterial hypertension (40%), chronic heart disease (19%), diabetes (11%), ulcerative colitis (2%), and Crohn’s disease (1%).
The most common clinical symptoms were abdominal pain (58%) and weight loss (> 5% loss of body mass within 6 months), seen in in 54% of respondents.
Stool blood was found in 34% of patients, diarrhoea occurred in 28%, and constipation in 27%. In addition, some patients reported pain during defecation (4%) and a feeling of incomplete bowel movement (6%). There was no statistically significant relationship between the group with metastases and without lymph node metastasis (p > 0.05) when these symptoms were considered.
In 31% of the patients, the tumour narrowed the lumen of the intestine, while in 11% it caused bowel obstruction. The average tumour size in patients was 4.84 ±2.54 cm. No statistically significant relationship was found (p > 0.05).
Among the patients with regional lymph node metastases, less than 26% had liver metastases: in both lobes (11.9%), in the right lobe (7.14%), in the left lobe (4.76%), and between the lobes (2.01%). There was no statistically significant relationship (p > 0.05).
Metastases to distant lymph nodes were found in 25% of patients with two regional lymph nodes affected by metastases; in 33% of those with three regional nodes involved; in 50% with 13 regional nodes involved, and in 100% with 7, 10, 18, 20, and 26 regional nodes affected by metastatic cancer. Patients with regional metastases to 10 and 26 regional lymph nodes had multiple distant nodular metastases. There was no statistically significant relationship (p > 0.05).
The highest CA 19-9 value was observed in a patient with regional metastases to seven lymph nodes collected during surgery (3573 U/ml), and the lowest was found in patients with two regional nodes affected by cancer (1.6 U/ml).
In total 26.19% of patients with regional lymph node metastases were found to have CA 19-9 above 37 U/ml. There was no statistically significant relationship (p > 0.05).
The highest CEA was observed in a patient with nine regional lymph node metastases (612.46 ng/ml) and the lowest in one with metastases to two regional nodes (0.2 U/ml). CEA value above 5 ng/ml was found in 35.74% of patients with regional lymph node metastases. A statistically significant relationship was reported (p < 0.05).
Among the patients with distant lymph node metastases, the most common primary tumour location was rectum (36.36%) and ascending colon (27.27%). In patients without metastases to distant lymph nodes, the most common cancer locations were the sigmoid colon (32.58%) and rectum (22.47%). Statistical analysis showed a significant relationship between the occurrence of distant lymph node metastasis and the location of the primary tumour (χ2 test = 38.98). However, there was no statistically significant relation between tumour size, BMI of patients, occurrence of physical symptoms, and involvement of distant lymph nodes (p > 0.05).
Questionnaire
Can factors that influence nodal dissemination in patients with colorectal cancer be identified? Own experience
Discussion
Regional lymph node metastases in CRC tell about the advancement of the disease and are a marker for 5-year survival prediction. Along with their occurrence, the risk of metastasis to distant lymph and peritoneal nodes increases [5]. The results of our own research seem to confirm this thesis. The presence of distant metastases was found only in patients with regional lymph node involvement.
Metastases to regional lymph nodes were found in 42% of the patients, of whom 26.19% had metastases to distant lymph nodes simultaneously. In the available literature, the average percentage of lymph node metastases in colorectal cancer is estimated to be around 35% [6]. In the study of Fujii et al. this percentage was 16.2%, of whom 16.2% had metastases to distant regional lymph nodes (N2) [7]. In the study of Zhou et al., metastases to regional nodes were found in 24.6% of patients, of which 10.4% were N2 metastases [8]. In order to accurately assess the stage and select the most effective treatment, intraoperative collection and pathological examination of at least 12 lymph nodes is recommended. According to the literature, this condition is met in only 20% of surgeries [9]. In our own study, all patients met the above condition.
Women slightly more often had metastases in regional (57.14%) and distant lymph nodes (63.64%). This difference was not statistically significant. In a study performed by Fujii et al. based on 228 patient cases of colorectal cancer, 66.66% of regional lymph node (N2) metastases occurred in women [7]. The increased participation of women in the development of colorectal cancer with nodal involvement is a consequence of hormonal disorders, especially in postmenopausal age [7, 10].
Colorectal cancer in obese women in premenopausal age may be a result of obesity-induced insulin resistance and the effects of leptin released from adipose tissue [10]. Adamowicz et al. proved that obesity is a significant risk factor for colorectal cancer. Obese men suffer from CRC more often than obese women [11].
The location of cancer in the distal part of the large intestine seems to be correlated with lymph node metastasis. Most metastases to regional lymph nodes occurred when the primary tumour location was in the rectum (23.8%) and sigmoid colon (21.43%), but without a statistically significant relationship [12].
The most common primary tumour location when metastases to distant lymph nodes were found was the rectum (36.36%) and ascending colon (27.27%). These results are consistent with those presented by Wang et al. They prove a higher risk of rectal cancer giving metastases to lymph nodes compared to colon cancer [13]. Different conclusions were presented by Fujii et al. and Rössler et al., showing a greater frequency of lymph node metastasis in colon tumours vs. rectum (83% vs. 17%). The 5-year survival rate is similar in both cancer locations with the co-occurrence of lymph node metastases [14].
The size of the tumour does not comply to tumour dissemination in the lymphatic system. The average tumour size among patients with involved regional lymph nodes was 4.84 ±2.54 cm and in patients with distant metastases it was 5.47 ±3.31 cm. Among N-negative patients the average tumour size was 4.72 ±2.13 cm. This does not differ significantly from the data presented by Rössler et al. and Fujii et al. [7, 14].
The histological type of cancer is important in lymph node dissemination of colorectal cancer. 85.71% of patients with regional lymph node metastases had a primary G3 tumour and 7.14% had a G4. Patients with distant lymph node metastases had 100% cancer assessed histologically as G3.
In the study of Fujii et al., 100% of patients with distant regional lymph node (N2) metastasis had a G3/G4 cancer type [7]. In the studies of Rössler et al., the primary tumour of patients with lymph node metastases was classified as G2 in 3.28%, G3 in 47.54%, and G4 in 49.18% [9, 14, 15].
In our own study, 30.95% of patients with metastatic regional nodes and 45.45% of patients with distant lymph node metastases had metastases in other tissues or organs. Naxerova's team proved that about 35% of distant metastases are derived from lymph node metastases [16]. A different hypothesis was formulated by Knijin et al., according to which metastases in the regional lymphatic system predispose mainly to metastases in the peritoneum and distant lymph nodes. On the other hand, metastatic lesions in other organs are usually unaffected by the lymphatic system dissemination, which seems to be confirmed by a comparable frequency of liver and lung metastases [5].
Undeniable confirmation of the origin of metastases in other organs would require further molecular studies. On average, liver metastases occur in 50% of colorectal cancers, and their incidence increases with the advancement of cancer as classified according to TNM. In 70–80% of patients with liver metastases there are metastases in other tissues and organs [17]. In our study, liver metastases were found in 20% of patients, 21.43% of them with regional lymph node metastases and 27.27% with distant lymph node metastases.
The presence of some symptoms of colorectal cancer suggests that there is a greater likelihood of lymph node metastasis. Weight loss was also significantly greater among patients with regional node metastases (64.28%) than in those without metastases (46.53%). A slight difference in the declared weight loss was also observed among patients with distant lymph node metastases (72.13%) as compared to those without metastases (51.68%). Weight loss is a relative predictor of cancer. N-positive patients with > 10% weight loss have a 3.3-fold increased risk of death [18].
Ca 19-9 and CEA tumour markers seem to be an important predictor of the severity of cancer, whereas their values were significantly higher in patients with regional and distant lymph node metastases. The frequency of elevated CEA values (above 5 ng/ml) was detected among patients with distant lymph node metastases (90.9%). In the Fujii et al. study, a CEA result above normal was obtained in 33% of patients with N2 metastases [7].
The CEA marker test is a simple and cost-effective method to identify patients who require intensive oncological surveillance and postoperative adjuvant therapy [19].
Conclusions
The location of the primary tumour, and its pathological stage and size does not seem to have a direct correlation with the occurrence of regional lymph node metastases. Metastasis to distant lymph nodes seems to be a consequence of metastases in regional nodes. Elevated CEA tumour marker values are significantly related to metastases in the regional lymph nodes. The elevation of CA 19-9 and CEA tumour markers significantly correlates with the presence of metastasis to distant lymph nodes. The location of the primary tumour determines the formation of metastases in distant lymph nodes.











