
Introduction
Spontaneous bacterial peritonitis (SBP) is one of the most frequent and life-threatening infectious complications in patients with decompensated cirrhosis and ascites, occurring in approximately 10-30% of hospitalized individuals and remaining associated with substantial short-term mortality despite advances in antimicrobial therapy [1-3]. Its pathophysiology is multifactorial, involving bacterial translocation, cirrhosis-related immune dysfunction, portal hypertension, and systemic inflammation [4-6]. Clinically, SBP often precipitates acute decompensation or acute-on-chronic liver failure and is an independent predictor of early mortality [7-9].
Current clinical practice guidelines strongly recommend early diagnostic paracentesis for all hospitalized patients with cirrhosis and ascites [8, 10]. Nevertheless, delays remain common in routine care, often due to concerns regarding coagulopathy or hemodynamic instability, logistical constraints in busy clinical settings, and the frequently subtle or nonspecific presentation of SBP [2, 10]. As delayed diagnosis and treatment are consistently associated with worse outcomes, improved strategies for early risk recognition at the time of hospital admission are needed [5, 9].
Several non-invasive approaches have recently been proposed to aid SBP risk stratification, ranging from simple bedside scores to models incorporating novel biomarkers or machine-learning techniques [11-15]. Earlier tools, such as the Wehmeyer and Mansoura scores, emphasized systemic inflammation using routinely available laboratory parameters [11, 12]. While more recent models report improved predictive performance, many rely on non-routine biomarkers, complex computational methods, or limited sample sizes, and lack broad validation or real-world clinical applicability [16-18]. Concurrent epidemiological trends – including rising antimicrobial resistance and evolving phenotypes of cirrhosis – further underscore the need for practical, updated, and widely applicable risk-stratification tools [19-23].
Against this background, we conducted a single-center cohort study to develop and internally validate a pragmatic bedside prediction score based exclusively on objective, routinely available admission variables. Our primary aim was to derive a simple four-component, point-based risk classification system – the SCAN score (serum sodium, C-reactive protein [CRP], age, and neutrophil-to-lymphocyte ratio [NLR]) – reflecting key pathophysiological domains relevant to SBP. The SCAN score is intended to complement, not replace, guideline-recommended diagnostic paracentesis by facilitating early risk stratification and helping prioritize patients at higher risk at initial presentation, particularly when clinical suspicion is low. This study reports the development, internal validation, and comparative performance of the SCAN score in accordance with the TRIPOD and STROBE reporting guidelines.
Material and methods
Study design and participants
This retrospective observational cohort study included consecutive adults (≥ 18 years) with cirrhosis and ascites admitted to a tertiary care center between January 2020 and January 2025. Cirrhosis was diagnosed according to established clinical, biochemical, radiologic, and/or histologic criteria [4]. Of 1,312 screened admissions, 1,000 unique patients fulfilled all eligibility criteria: 1) confirmed cirrhosis with ascites, 2) index hospitalization during the study period, 3) availability of baseline clinical and laboratory data, and 4) diagnostic paracentesis performed within 24 hours of admission.
Patients were excluded if they had secondary peritonitis with a surgically treatable source, recent abdominal surgery (< 4 weeks), intra-abdominal malignancy with peritoneal carcinomatosis, systemic antibiotic therapy for non-SBP indications at admission, or incomplete medical records. To avoid intra-individual clustering, only the first eligible hospitalization per patient was included. The study population was randomly divided into a derivation cohort (n = 700) and an internal validation cohort (n = 300).
The study protocol was approved by the Kayseri City Hospital Non-Interventional Clinical Research Ethics Committee (Approval No. 287, January 7, 2025). The requirement for informed consent was waived due to the retrospective and de-identified nature of the data. The study was conducted in accordance with the Declaration of Helsinki.
Definitions and outcomes
Spontaneous bacterial peritonitis was defined as an ascitic polymorphonuclear leukocyte count ≥ 250 cells/mm3, with or without a positive culture result, in the absence of a surgically treatable intra-abdominal source [2, 8, 10]. Culture-negative neutrocytic ascites was classified as SBP. Infections diagnosed more than 48 hours after hospital admission were considered nosocomial and were excluded from the primary analysis but included in prespecified sensitivity analyses. A total of 15 nosocomial SBP cases were identified and excluded from the primary model. The primary outcome was SBP present at the time of index admission.
Data collection and candidate predictors
Clinical and laboratory variables obtained at admission or within six hours of diagnostic paracentesis were extracted from electronic medical records. Collected data included demographic characteristics, cirrhosis etiology, selected clinical parameters (fever, hepatic encephalopathy, mean arterial pressure, recent gastrointestinal bleeding), laboratory tests (complete blood count, NLR, CRP, serum sodium, renal and hepatic function tests, and international normalized ratio), and ascitic fluid analyses.
Disease severity was assessed using Child-Pugh, MELD, and MELD-Na scores; these composite indices were not entered into multivariable models to avoid collinearity. Therapeutic exposures, including albumin administration, vasoconstrictor therapy, proton pump inhibitor use, and long-term antibiotic prophylaxis, were evaluated as candidate predictors. Long-term antibiotic prophylaxis (norfloxacin 400 mg/day or rifaximin 550 mg twice daily) was used in 22.1% of patients overall, with no significant difference between the non-SBP (18.9%) and SBP (25.4%) groups (p = 0.08).
Handling of missing data and cut-off selection
Variables with ≥ 20% missing values were excluded a priori. Remaining missing data were handled using multiple imputation by chained equations (10 imputations), assuming data were missing at random. Continuous predictors were evaluated for nonlinearity. Clinically established thresholds were applied for serum sodium (< 130 mmol/l) and age (> 60 years).
Optimal cut-off values for CRP (> 50 mg/l) and NLR (> 4) were determined within the derivation cohort. These thresholds were selected based on established literature linking them to significant systemic inflammation and bacterial infection in cirrhosis [11, 12, 24], and they provided the most favorable balance between discrimination and clinical interpretability in our cohort. Alternative cut-off values were explored but did not result in meaningful improvements in model performance. Multicollinearity was assessed using variance inflation factors, with values < 5 considered acceptable.
Model development (SCAN score)
Model development was performed in the derivation cohort in accordance with TRIPOD recommendations. Candidate variables identified in univariable analyses (p < 0.10) were entered into a multivariable logistic regression model. Four independent predictors were retained: CRP > 50 mg/l, NLR > 4, serum sodium < 130 mmol/l, and age > 60 years. The full regression equation with unrounded coefficients is provided in Supplementary Table 1.
Regression coefficients were scaled and rounded to derive a simple additive bedside score (SCAN), ranging from 0 to 6 points. Two points were assigned for CRP > 50 mg/l and NLR > 4, and one point each for serum sodium < 130 mmol/l and age > 60 years. Risk categories were defined a priori as low (0-2 points), intermediate (3-4 points), and high (5-6 points).
Model performance and validation
Model discrimination was assessed using the area under the receiver operating characteristic curve (AUROC) with 95% confidence intervals. Calibration was evaluated using the calibration slope, Brier score, and calibration plots. Internal validation was conducted using bootstrap resampling (1,000 iterations) to estimate optimism and assess potential overfitting. Final performance measures were reported in the validation cohort.
Comparative performance and sensitivity analyses
The SCAN score was compared with the Wehmeyer [11] and Mansoura [12] scores using identical predictor definitions and outcome criteria. Prespecified sensitivity analyses included: 1) exclusion of nosocomial SBP cases, 2) restriction to culture-positive SBP, 3) exclusion of patients receiving long-term antibiotic prophylaxis, and 4) refitting the model using continuous predictors.
Statistical analysis
Continuous variables are presented as mean ± standard deviation or median (interquartile range), and categorical variables as number (percentage). Statistical analyses were performed using R software (version 4.3.1) and IBM SPSS Statistics for Windows (version 27.0). Reporting followed the STROBE and TRIPOD reporting guidelines.
Results
Patient characteristics
The study included 1,000 adults with cirrhosis and ascites (Fig. 1), randomly allocated to a derivation cohort (n = 700) and an internal validation cohort (n = 300). The cohort was predominantly male (68.3%), with a mean age of 58.2 ±11.5 years. The main etiologies of cirrhosis were viral hepatitis (52.4%), alcohol-related liver disease (30.0%), metabolic-associated steatotic liver disease (MASLD/MASH) (14.7%), and cryptogenic causes (2.9%).
Fig. 1
Study flow diagram showing patient selection, exclusion criteria, and allocation into derivation and internal validation cohorts
Nosocomial infections diagnosed > 48 h after admission (n = 15) were excluded from the primary analysis and included in prespecified sensitivity analyses.
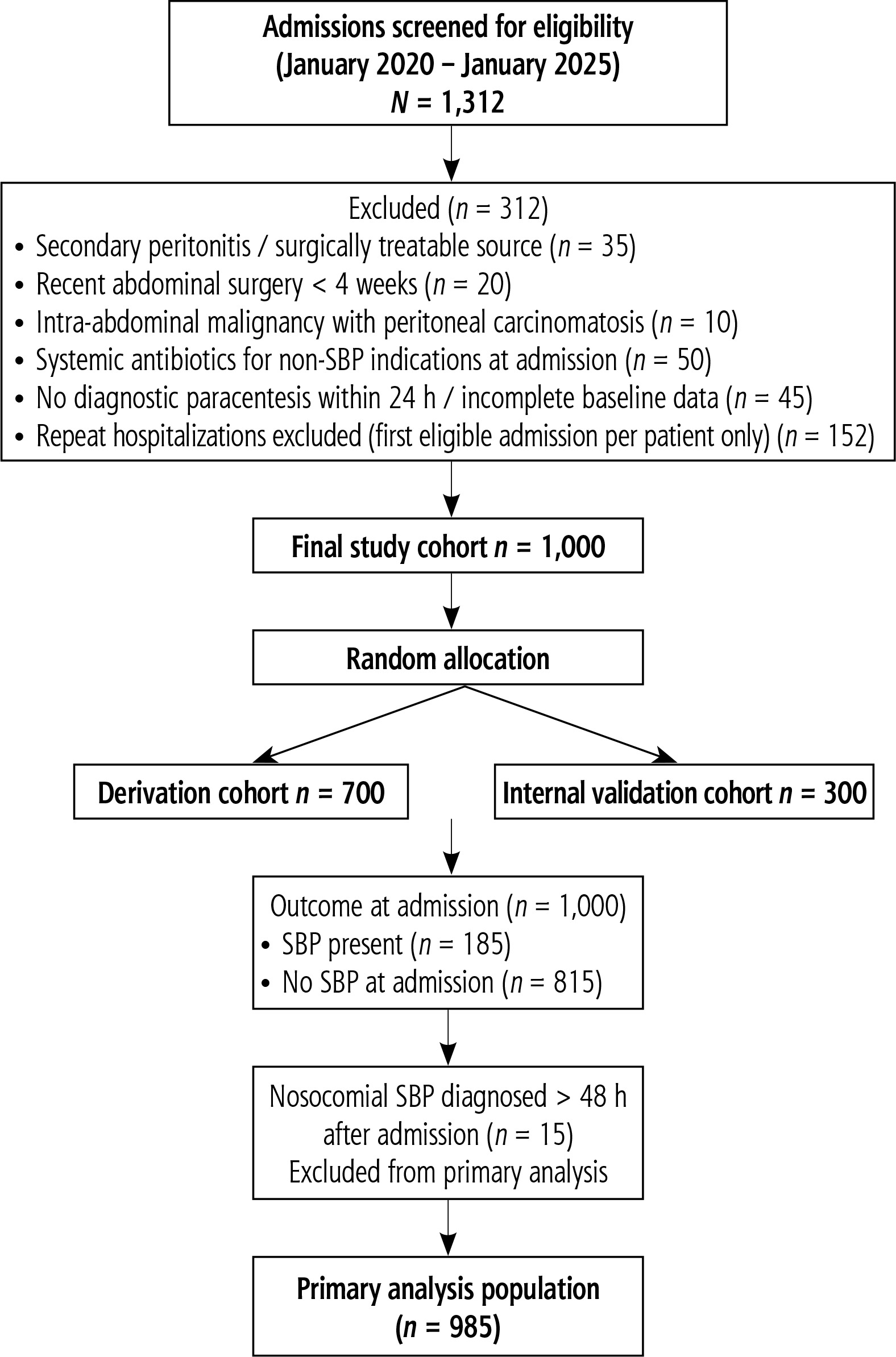
At the time of admission, SBP was diagnosed in 185 patients (18.5%). Compared with patients without SBP, those with SBP had more advanced liver disease, as reflected by higher Child-Pugh scores (10.8 ±2.1 vs. 7.9 ±1.8) and MELD-Na scores (24.1 ±5.3 vs. 18.3 ±4.6, all p < 0.001). Markers of systemic inflammation were also more pronounced in patients with SBP, including higher NLRs (6.4 ±2.3 vs. 2.9 ±1.1, p < 0.001). Long-term antibiotic prophylaxis was used in 22.1% of patients overall, with no significant difference between the SBP and non-SBP groups (25.4% vs. 18.9%, p = 0.08). Baseline characteristics are summarized in Table 1.
Table 1
Baseline characteristics of patients with cirrhosis and ascites
Predictor selection and SCAN score construction
Multivariable logistic regression analysis identified four variables independently associated with SBP: CRP > 50 mg/l, NLR > 4, serum sodium < 130 mmol/l, and age > 60 years (all p ≤ 0.01). The adjusted regression coefficients of these predictors in their continuous form are presented in Table 2.
Table 2
Continuous multivariable predictors of spontaneous bacterial peritonitis (SBP)
| Variable | Adjusted odds ratio (95% CI) | β coefficient | Variance inflation factor (VIF) | p-value |
|---|---|---|---|---|
| C-reactive protein (per mg/l) | 1.07 (1.04-1.11) | 0.067 | 1.42 | < 0.001 |
| Neutrophil-to-lymphocyte ratio (per unit) | 1.29 (1.15-1.44) | 0.255 | 1.26 | < 0.001 |
| Serum sodium (per mmol/l) | 0.91 (0.87-0.95) | –0.094 | 1.18 | < 0.001 |
| Age (per year)* | 1.03 (1.01-1.05) | 0.030 | 1.12 | 0.002 |
Coefficients represent the continuous forms of predictors in the multivariable model prior to dichotomization for construction of the final SCAN point-based score.
Based on scaled and rounded regression coefficients, a point-based bedside score (SCAN) was constructed. Two points were assigned for CRP > 50 mg/l and NLR > 4, and one point each for serum sodium < 130 mmol/l and age > 60 years, yielding a total score ranging from 0 to 6. For illustrative purposes, a 65-year-old patient with a serum sodium of 128 mmol/l, CRP of 60 mg/l, and a NLR of 5 would receive 1 point for age, 1 point for sodium, 2 points for CRP, and 2 points for NLR, resulting in a total SCAN score of 6 and classification into the high-risk category.
Model performance and internal validation
The SCAN model demonstrated good discriminatory ability, with an area under the receiver operating characteristic curve (AUROC) of 0.92 (95% CI: 0.89-0.95) in the derivation cohort and 0.91 (95% CI: 0.87-0.94) in the validation cohort.
Calibration in the validation cohort was acceptable, with a calibration slope of 0.96, a Brier score of 0.06, and a non-significant Hosmer-Lemeshow goodness-of-fit test (p = 0.55). The calibration plot showed close alignment between predicted and observed SBP probabilities across the full range of risk, indicating good overall model fit (Supplementary Fig. 1). Internal validation using 1,000 bootstrap replications demonstrated minimal optimism (ΔAUROC ≈ 0.01), suggesting a low risk of overfitting. Comparative performance metrics are summarized in Table 3.
Table 3
Performance characteristics of the SCAN score and selected previously reported prediction models
| Model | AUROC (95% CI) | DeLong p-value vs. SCAN | Calibration slope | Brier score |
|---|---|---|---|---|
| SCAN | 0.91 (0.87-0.94) | – | 0.96 | 0.06 |
| Mansoura score [12] | 0.85 (0.80-0.90) | 0.003 | 0.84 | 0.08 |
| Wehmeyer score [11] | 0.68 (0.61-0.75) | < 0.001 | 0.77 | 0.10 |
| Cullaro et al. ascites NGAL model [16] | 0.75 (0.69-0.81) | < 0.001 | 0.81 | 0.09 |
| Hu et al. AI-based model* [14] | 0.88 (0.84-0.92) | 0.042 | 0.88 | 0.07 |
[i] AUROC – area under the receiver operating characteristic curve, NGAL – neutrophil gelatinase-associated lipocalin
[iii] All bedside models were applied using identical predictor definitions and SBP outcome criteria.
[iv] The AI-based model by Hu et al. [14] is included for contextual comparison only; model coefficients are not publicly available, and therefore it could not be implemented as a bedside clinical tool in the present analysis.
Risk stratification and diagnostic performance
The observed prevalence of SBP increased progressively with higher SCAN scores: 2.2% for a score of 0, 3.3% for a score of 1, 5.8% for a score of 2, 16.7% for a score of 3, 41.3% for a score of 4, and 75.0% for scores of 5-6 (p < 0.001 for trend; Table 4).
Table 4
Observed incidence of spontaneous bacterial peritonitis (SBP) according to SCAN total score
Using a prespecified threshold of SCAN ≥ 3 in the validation cohort, sensitivity was 88.1% and specificity was 91.7%. Among patients with a SCAN score of 0, no SBP events were observed in the validation cohort, yielding a negative predictive value of 100% for this subgroup.
Decision curve analysis demonstrated a higher net clinical benefit for the SCAN score compared with treat-all, treat-none, and single-parameter strategies across threshold probabilities between approximately 15% and 40%. Compared with CRP > 50 mg/l alone, the SCAN score provided incremental predictive value, as reflected by significant improvements in net reclassification and discrimination indices (both p < 0.001).
Comparative performance
When applied to the validation cohort, the SCAN score demonstrated superior discriminatory performance compared with the Mansoura score (AUROC 0.85; p = 0.003) and the Wehmeyer score (AUROC 0.68; p < 0.001). The SCAN score also showed numerically higher performance than previously reported biomarker-based and machine learning-based models included for contextual comparison (Table 5).
Table 5
Diagnostic performance of the SCAN score compared with selected prediction models in the validation cohort
| Model | AUROC (95% CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Feasibility† |
|---|---|---|---|---|---|---|
| SCAN | 0.91 (0.87-0.94) | 88.1 | 91.7 | 89.6 | 100* | High |
| Mansoura score [12] | 0.85 (0.80-0.90) | 80.0 | 88.4 | 76.2 | 92.1 | Moderate |
| Wehmeyer score [11] | 0.68 (0.61-0.75) | 70.4 | 75.2 | 62.4 | 85.3 | Moderate |
| Hu et al. AI-based model [14]‡ | 0.88 (0.84-0.92) | 84.7 | 89.1 | 84.3 | 94.7 | Limited |
AUROC – area under the receiver operating characteristic curve, PPV – positive predictive value, NPV – negative predictive value
† Feasibility reflects bedside applicability and routine availability of required variables. Feasibility categories: High, Moderate, Limited.
* An NPV of 100% applies to patients with a SCAN score of 0, among whom no SBP events were observed in the validation cohort.
‡ The AI-based model by Hu et al. [14] is included for contextual comparison only; model coefficients are not publicly available, and therefore it could not be implemented as a bedside clinical tool.
Sensitivity analyses
All prespecified sensitivity analyses yielded consistent results. Model performance remained stable when nosocomial SBP cases (n = 15) were excluded (AUROC 0.90, calibration slope 0.95). Comparable and stable performance was observed when analyses were restricted to culture-positive SBP, when patients receiving long-term antibiotic prophylaxis were excluded, and when continuous predictors were modeled instead of dichotomized cut-offs. Across these analyses, AUROC values ranged from 0.90 to 0.92, and calibration slopes ranged from 0.94 to 1.02.
Discussion
In this study, we developed and internally validated the SCAN score, a pragmatic bedside tool incorporating serum sodium, CRP, age, and NLR for the early identification of SBP in patients with decompensated cirrhosis and ascites. Using exclusively routinely available admission variables, SCAN demonstrated consistent and strong discriminatory performance, with AUROC values of 0.92 and 0.91 in the derivation and validation cohorts, respectively. Given the often subtle clinical presentation of SBP and its strong association with early adverse outcomes, a simple and readily applicable risk-stratification tool may support timely clinical decision-making at hospital presentation [1-3]. Importantly, the SCAN score is designed to complement, not replace, guideline-recommended diagnostic paracentesis by aiding in risk stratification and helping prioritize patients at higher risk, particularly when clinical suspicion is low [8].
From a methodological perspective, the performance of SCAN was supported by favorable discrimination and calibration metrics, as well as by its net clinical benefit across clinically relevant threshold probabilities in decision curve analysis [25]. The combined assessment of discrimination and calibration aligns with contemporary methodological standards for clinical prediction models [26]. The minimal optimism observed during bootstrap internal validation (ΔAUROC ≈ 0.01) suggests a low risk of overfitting, despite the derivation of optimal cut-off values for CRP and NLR within the same cohort. This robustness is further supported by stable performance across multiple prespecified sensitivity analyses.
SCAN builds upon earlier bedside prediction efforts by integrating complementary pathophysiological domains relevant to SBP. Previous scores, such as the Wehmeyer and Mansoura scores, primarily focused on markers of systemic inflammation and demonstrated moderate discriminatory performance [11, 12]. The inclusion of serum sodium in SCAN captures circulatory dysfunction and effective hypovolemia, which are central features of advanced cirrhosis and contribute to immune impairment and increased susceptibility to infection [24]. Age reflects reduced physiological reserve and immunosenescence, which are increasingly recognized as important modifiers of infection risk and outcomes in cirrhosis [27]. The selected cut-off values for CRP (> 50 mg/l) and NLR (> 4) were informed by existing literature linking these thresholds to significant systemic inflammation in cirrhosis and by their favorable performance within our cohort, providing a balance between clinical relevance and predictive accuracy [11, 12, 24]. Together, these variables offer a clinically intuitive framework aligned with the multifactorial pathophysiology of SBP.
From a practical standpoint, SCAN offers straightforward bedside applicability. Unlike models dependent on specialized biomarkers or complex computational methods, it can be calculated at hospital admission using routine laboratory data, facilitating integration into clinical workflows. SBP risk increased progressively across SCAN categories, supporting its use for clinical risk stratification. Patients with SCAN scores ≥ 3 may warrant closer monitoring and prioritized diagnostic evaluation, even in the absence of classic symptoms [4]. Nevertheless, diagnostic paracentesis remains the gold standard and is recommended for all hospitalized patients with cirrhosis and ascites, regardless of risk score classification [8].
The predominance of viral hepatitis as the underlying etiology in our cohort (52.4%) may raise questions regarding generalizability to Western populations, where alcohol-related and metabolic-associated liver diseases are more prevalent. However, the pathophysiological domains captured by SCAN – systemic inflammation, circulatory dysfunction, and immunosenescence – are universal hallmarks of advanced cirrhosis and are largely independent of etiology. External validation in geographically and etiologically diverse populations will therefore be essential to confirm its broader applicability.
Several strengths of this study merit consideration, including the large and well-characterized cohort, standardized data collection, rigorous internal validation using bootstrap resampling, and adherence to TRIPOD and STROBE reporting guidelines. The exclusive use of routinely available variables enhances feasibility and supports potential implementation across diverse clinical settings.
This study also has limitations. Its retrospective, single-center design may limit external generalizability, and residual confounding cannot be excluded. The analysis was restricted to admission variables and did not account for in-hospital management decisions or treatment delays. Although cut-off values for CRP and NLR were optimized within the derivation cohort, which introduces a theoretical risk of overfitting, internal validation and consistent performance across sensitivity analyses suggest that this risk is limited. Furthermore, while therapeutic interventions such as albumin administration are integral to SBP management, their effects were beyond the scope of this prediction-focused analysis [28, 29].
External validation in independent, multicenter, and etiologically diverse cohorts is required before SCAN can be recommended for routine clinical use. Future studies should also evaluate its ability to predict SBP recurrence, short-term clinical outcomes, and its potential impact when integrated into structured clinical care pathways.
Conclusions
The SCAN score is a simple, transparent, and physiologically grounded bedside tool for early risk stratification of spontaneous bacterial peritonitis in patients with cirrhosis and ascites. By combining four routinely available admission variables, it demonstrated reliable discrimination and calibration in a large single-center cohort. SCAN may assist clinicians in prioritizing diagnostic evaluation and supporting timely management decisions in routine clinical practice. Prospective multicenter validation studies are needed to confirm its generalizability, clinical utility, and impact on patient outcomes.





