
Introduction
Betatrophin is a hormonal protein secreted by the liver and adipose tissue and encoded by the gene C19orf80 (chromosome 19 reading frame 80). It is also known by various other names: ANGPTL8 (angiopoietin-like protein 8), RIFL (refeeding induced fat and liver protein), lipasin, and TD26 (hepatocellular associated protein).
In the process of establishing the function of betatrophin, its significance in fat metabolism was first determined. Betatrophin affects lipoprotein lipase: it regulates fasting and postprandial triglyceride concentration by inhibiting lipoprotein lipase. It also affects the distribution of fatty acids in muscle tissue and adipose tissue [1, 2].
It was also found that betatrophin levels are higher in patients with liver cirrhosis, increasing proportionally with the liver disease progression score and with insulin resistance [3-5]. Theoretically, betatrophin also participates in carcinogenesis, possibly influencing the Wnt/β-catenin pathway [6, 7]. An increase in betatrophin was observed in patients with cirrhosis, but there is little research on patients with primary liver cancer.
Betatrophin also shows antiproliferative effects and induces apoptosis in patients with pancreatic tumors [8]. The betatrophin levels in this group of patients are elevated and correlate with the presence of diabetes [9].
Betatrophin is now recognized as a marker of certain disease states, primarily diabetes. Betatrophin is also considered a marker of obesity [10, 11].
Hepatocellular carcinoma (HCC) is classified as the third-to-fifth most frequently diagnosed type of cancer. As the diagnosis is usually established at an advanced stage, it is also the second most common cause of death. The etiological factor of cancer development is liver cirrhosis (secondary to infections with hepatotropic viruses, fatty liver, alcohol, etc.). The incidence of this cancer is increasing every year and will continue to do so in the coming years.
Therefore, this study aimed to assess the significance of betatrophin levels in patients with cirrhosis and HCC, to determine whether betatrophin is a marker of liver fibrosis or neoplasia, and to evaluate whether it could serve as an auxiliary factor in HCC diagnosis. Another aim of our study was to assess betatrophin levels in relation to sex. This aspect has not previously been investigated in patients with cirrhosis or HCC. We sought to determine whether betatrophin concentration demonstrates greater diagnostic sensitivity in either women or men with cirrhosis and/or with HCC.
Material and methods
The study cohort comprised patients supervised and treated for chronic liver disease of various etiologies at the First Department of Jerzy Gromkowski Regional Specialist Hospital. To avoid interference of pharmacotherapy with betatrophin measurements, the study included patients in whom any type of therapy had been completed at least two months prior to histopathological examination.
Patients with liver cirrhosis (diagnosis based on biopsy or endoscopy and/or imaging of the liver) and HCC (diagnosis confirmed by dual CT and MRI imaging with contrast and, in some cases, with tumor biopsy), hospitalized between 2022 and 2024 were enrolled as study participants. The control group consisted of patients with chronic non-advanced liver disease.
Patients were assessed for hepatotropic virus infections, coexisting diabetes, and hypertension. Patients with type 2 diabetes had their glycemic levels controlled (glycated hemoglobin at less than 7%), while those with hypertension were on continuous therapy and their blood pressure stayed under 150/90 mmHg. In the studied group, liver function was assessed using the Child-Turcotte-Pugh (CTP) scale. In the group with cancer, the Barcelona Clinic Liver Cancer (BCLC) staging system was also applied. Patients with chronic pancreatic diseases, proliferative diseases, alcohol use of > 20 g per day, and autoimmune causes of liver diseases were excluded from the study.
The albumin-bilirubin (ALBI) score was included to assess liver function and improve clinical utility. It was calculated based on serum total bilirubin and albumin, according to the following formula: ALBI = 0.66 × log10 (bilirubin) − 0.085 × albumin. ALBI grades 1, 2, and 3 were separately defined as ALBI ≤ −2.60, −2.60 < ALBI ≤ −1.39, and ALBI > −1.39, respectively [12].
The BCLC staging system is currently the most accurate tool for simultaneously assessing disease severity, therapeutic options, and expected survival.
Specifically, it provides a prognostic evaluation based on tumor size, liver function, and the patient’s performance status, incorporating α-fetoprotein (AFP) concentration as well as the ALBI, Child-Pugh, and MELD scores. It further outlines patient characteristics to individualize treatment strategies, estimates survival, and guides clinical decision-making and potential changes in therapy. The BCLC system comprises five stages: very early (0), early (A), intermediate (B), advanced (C), and terminal (D). The BCLC scores were A 13, B 56, C 27.
Statistical methods
The methods used in this article included basic descriptive statistics tools – mean, median, range – which were primarily used to collect information about the study group. Descriptive statistics were also used to verify the results obtained with more advanced statistical methods.
The Mann-Whitney U-test and the Kruskal-Wallis test were nonparametric equivalents of the Student t-test for independent samples.
Analytical methods: betatrophin measurements
Blood samples were collected by venipuncture on the fasting morning on the day of admission to the hospital. The separated serum was aliquoted and frozen at −80°C for future analysis. Biochemical parameters were measured using available clinical methods, and data on their concentration or activity were obtained from the patients’ medical records. Betatrophin concentration was estimated using ELISA (AVISCERA BIOSCIENCE, Santa Clara, California, USA) in line with the manufacturer’s protocol.
ELISA was performed using standard equipment (Multiskan Go microplate reader, Thermo Scientific, Uusimaa, Finland), and quality controls and samples were incubated for two hours in a microwell plate precoated with anti-human betatrophin monoclonal antibodies. After washing the plate of any unbound substances, a biotinylated anti-human total betatrophin monoclonal detection antibody was added and incubated for another two hours at room temperature, also on a microwell plate shaker. After a second wash, streptavidin-HR conjugate was added and incubated for one hour. After a final wash to remove the unbound enzyme, substrate solution (TMB) was added to the wells. Incubation lasted 15 minutes. The reaction was stopped by adding acidic solution. The color in the wells changed from blue to yellow. The intensity of the resulting coloration was directly proportional to the amount of betatrophin bound in standard solutions or samples. A standard curve was established (in the concentration range between 0.781 ng/ml and 50 ng/ml) and used to read the betatrophin concentration values in the assayed samples. Betatrophin concentrations were measured using a high-specificity ELISA assay capable of detecting both the C-terminal fragment of betatrophin (amino acids 100-198) and the 21-198 amino-acid form. The calibration curve was prepared using recombinant mature betatrophin (21-198 aa). According to the manufacturer’s documentation, the intra-assay precision is 2-5%, and the inter-assay precision is 4-8%. All measurements in our study were performed in duplicate, and the intra-assay precision calculated from our dataset was 4.8%, confirming the high reproducibility and reliability of the assay.
Results
The study was approved by the Ethics Committee of the Medical University in Wroclaw and conformed to the ethical guidelines of the Declaration of Helsinki (KNW/0022/KB1/95/13; KB 01/07/2020). Informed consent was obtained for the whole study series. Informed consent was obtained for the whole study series.
The study population consisted of 190 individuals: 96 patients with HCC – group 1; 81 patients with liver cirrhosis – group 2; and 13 patients with non-advanced liver disease – group 3 (control group). All groups were dominated by men: 71 with HCC, 57 with liver cirrhosis, and 7 in the control group. In the female subpopulation, 25 had HCC, 24 had liver cirrhosis, and 6 were in the control group. All patients with HCC had liver cirrhosis. Only those in the control group did not have liver cirrhosis.
Liver function was assessed using the Child-Pugh scale. Additionally, the ALBI score was calculated based on serum total bilirubin and albumin, which represent liver function. The average age of men in the study population was 59 (20-88) years, and the average age of women was also 59 (34-80) years. Patients with HCC had an average age of 61.5 (20-88) years: in men 62 (20-88) years, and in women 61 (41-80) years.
In the HCC group, liver function assessed by CTP score was as follows: in men, CTP A – 39, CTP B – 29, CTP C – 3; in women, CTP A – 13, CTP B – 8, CTP C – 4. The MELD score was 13 in men and 12 in women. BCLC staging was A 13, B 56, C 27. Patients with liver cirrhosis were on average 58.5 years (24-86): in men 56 (24-86) years old, and in women 58 (34-77) years old. Liver function assessed by CTP score was in men: CTP A – 28, CTP B – 26, CTP C – 3, in women: CTP A – 5, CTP B – 16, CTP C – 3, and the median MELD score was 12.5 in men and 9.5 in women.
The mean age of the control group was 46 (38-65) years. The patients in the first group were significantly older than the patients in the control group (p < 0.001). Patients with liver cirrhosis were also order than the control group (p < 0.05).
The results of basic laboratory tests are presented in Table 1. The mean results of individual parameters of patients in the studied groups differed statistically significantly: γ-glutamyltransferase (GGT) in patients in the HCC group was 109 IU/l, while in the cirrhosis group it was 75.5 IU/l, p < 0.05. Alkaline phosphatase activity in the HCC group was 122 IU/l, in the cirrhosis group 95 IU/l, p < 0.01. In our study, betatrophin levels correlated in men with HCC with insulin levels (r = 0.4) and inversely with prothrombin activity (r = –0.4) and albumin (r = –0.5), and in women with liver cirrhosis (r = 0.5) with AST activity (r = 0.5) and inversely with albumin levels (r = –0.8).
Table 1
Clinical and biochemical characteristics of patients
| Parameter | Hepatocellular carcinoma | Cirrhosis | Control group |
|---|---|---|---|
| N | 96 | 81 | 13 |
| Male/female, n (%) | 71/25 (74/26) | 57/24 (70.4/29.6) | 7/6 (53.8/46.2) |
| Age (years) | 61.5 (20.0-88.0)*** | 58.5 (24.0-86.0)^ | 46.0 (38.0-65.0) |
| ALBI scale | (–)1.7 ((–)3.1-(–)3.1*+) | –1.9 ((–)3.2-(–)1.1) | (–)2.4 ((–)3.2-(–)1.7) |
| BCLC score, n (%) | 13/56/27 (13.5/58.3/28.2) | – | – |
| ALT (IU/l) | 57.0 (11.0-327.0) | 77.5 (7.0-422.0) | 48.0 (14.0-131.0) |
| AST (IU/l) | 64.5 (16.9-598.0) | 57.5 (14.0-614.0) | 42.0 (15.0-121) |
| GGT (IU/l) | 109.0 (21.0-5406.0)+ | 75.5 (12.0-965.0) | 63.0 (19.0-190.0) |
| ALP (IU/l) | 122.0 (44.0-1319.0)++ | 95.0 (38.0-363.0) | 96.5 (44.0-177) |
| Glucose (mg/dl) | 106.0 (67-592) | 111.0 (56.7-281.0) | 103.6 (74.6-246.6) |
| Total cholesterol (mg/dl) | 150.0 (49.0-374.0) | 142.3 (50.8-230) | 148.5 (44.9-199.9) |
| Triglycerides (mg/dl) | 104.2 (37.0-183.2) | 83.8 (36.0-676) | 101.6 (71.6-162.7) |
| Leucocytes (× 109/l) | 5.0 (2.9-19.0) | 5.7 (2.5-14.0) | 5.8 (2.64-12.08) |
| HGB (g/dl) | 12.4 (5.7-16.5) | 12.9 (5.8-18) | 13.5 (10.7-16.6) |
| Platelets (× 109/l) | 96.0 (18.0-395) | 99.5 (11.2-436.0) | 190.0 (42.0-256.0) |
| AFP (ng/ml) | 393.0 (0.7-5845)+++ | 4.5 (1.0-2763.0) | 3.6 (1.5-118.6) |
| Betatrophin (ng/ml) | 25.0 (0-139.2)* | 21.9 (0-158.1) | 7.6 (0-63.6) |
Comorbidities
Hepatitis C virus (HCV) infection was found in 59 patients (61.46%) in the HCC group, 20 (33.89%) women and 39 (66.1%) men. A total of 40 (49.38%) patients in the cirrhosis group – 26 (65%) men and 14 (35%) women – and 10 control patients (6 men (60%) and 4 women (40%)) were diagnosed with HCV infection, which accounted for 76.92%. No correlation was found between HCV infection and betatrophin levels in the study groups.
Hepatitis B virus (HBV) infection was confirmed in 15 patients (18.52%) of the cirrhosis group: 3 women (20%) and 12 men (80%). HBV/HCV co-infection occurred in 6 (40%) of them: 3 women (50%) and 3 men (50%). Thirty-two patients (33.3%) in the cancer group had HBV infection: 26 men (81.25%) and 6 women (18.75%). No HBV infection was found in the control group. No significant difference was observed between the presence of HBV infection and betatrophin concentration in the studied patient groups.
Betatrophin
A significant difference between betatrophin levels in the group of patients with hepatocellular carcinoma and the group without advanced liver disease was demonstrated using the Kruskal-Wallis test (p = 0.0349). Additionally, no correlation was found between betatrophin concentration and cirrhosis severity as assessed using the CTP and MELD scoring systems. Also, there were no statistically significant differences between patients with different cancer severity assessed using the BCLC scoring system.
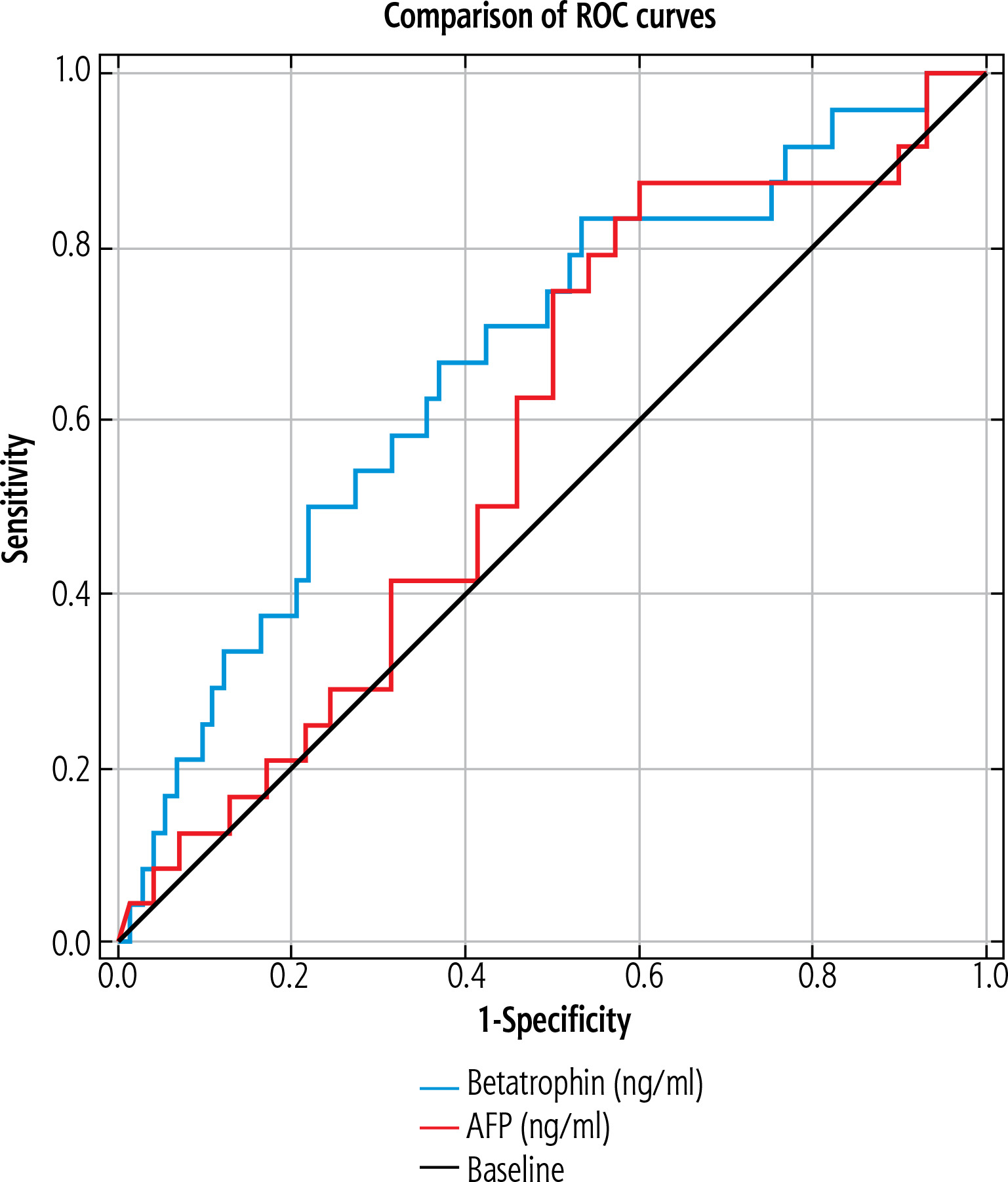
In the group of patients with hepatocellular carcinoma, analyzing betatrophin levels by gender showed higher betatrophin levels in women (41.18 ng/ml) than in the entire HCC cohort (25 ng/ml). Diagnostic accuracy in identifying women with HCC with cirrhosis was assessed using the area under the ROC curves and compared with AFP. These curves were generated by plotting sensitivity vs. 1-specificity. 95% confidence intervals (CIs) were calculated for the area under the curve (AUC). The optimal cutoff point was determined by ROC analysis by selecting the value that maximized the sum of sensitivity and specificity. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were assessed for each optimal cutoff point. Betatrophin was found to be a better marker for detecting HCC in women with cirrhosis with an AUC of 0.642 (Fig. 1). The optimal betatrophin threshold for predicting HCC was 30.23 ng/ml, with a sensitivity of 64.0%, specificity of 62.5%, a PPV of 37.2%, and NPV of 83.3%. ROC curves were assessed using the DeLong method. Betatrophin proved to be a better marker of tumorigenesis: betatrophin (AUC = 0.642) showed significantly better discriminatory performance than AFP (AUC = 0.584) in detecting HCC in women with liver cirrhosis. Diagnostic accuracy was 65.9% for betatrophin and 60.4% for AFP (Table 2).
Table 2
Comparison of diagnostic value of betatrophin and α-fetoprotein (AFP) in women with hepatocellular carcinoma (HCC)
| Parameter | Cut-off | AUC (95% CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | ACC |
|---|---|---|---|---|---|---|---|
| Betatrophin (ng/ml) | 30.23 | 0.642 (0.55-0.77) | 64.0 | 62.5 | 37.2 | 83.3 | 65.9 |
| AFP (ng/ml) | 8.66 | 0.584 (0.45-0.72) | 88.0 | 40.6 | 34.9 | 90.3 | 53.2 |
Discussion
Screening for early diagnosis of HCC in patients with cirrhosis has been recommended for many years by hepatology societies around the world. Such tests typically cover an abdominal ultrasound and, at times, AFP level checks, repeated in patients with cirrhosis every 6 months (according to the European [13] and American [14] Societies) or every 3 months (according to the Japanese Society). Unfortunately, the correct and accurate performance of an abdominal ultrasound is highly dependent on the skill of the performer and the quality of the equipment.
Similarly, AFP levels do not increase in all HCC patients. Some, despite advanced liver cancer, demonstrate normal AFP levels, with a sensitivity of 4-71% and specificity of 29-100% [15]; in the early stages they show a sensitivity of 39-46%, specificity of 76-97%, and a predictive value of 9-32% [16]. AFP is a more sensitive marker for recurrence during oncological treatment.
Adipokines secreted in the liver are natural candidates. In our earlier paper, we highlighted the significance of measuring levels of various adipokines, e.g. chemerin, in the diagnosis of HCC [17]. In this article, we show that the concentration of chemerin increases with tumor progression (i.e. with increasing number of HCC foci), and decreases with the progression of liver disease, assessed using the CTP score.
In another study, we investigated vaspin and visfatin levels in cirrhotic patients with HCC. The concentration of vaspin proved to be a more sensitive marker. Compared to healthy controls, serum vaspin was significantly elevated in HCC patients, independently of cancer etiology. Vaspin upregulation can be a compensatory mechanism against IR in HCC patients, especially in those with HCV infection.
In contrast, serum visfatin and vaspin, although upregulated in this group of patients, seem not to be associated with cancer grade and cirrhosis severity [18].
The decrease in irisin levels in both cirrhotic and HCC patients is correlated with disease progression. Thus, it is a marker of disease and cachexia progression rather than a cancer marker [5].
In our early studies, we measured betatrophin levels in groups of patients with liver disease of various etiologies and different stages of liver fibrosis and a group with HCC. The results were correlated with the progression of fibrosis assessed with the CTP score, but not tumor progression [4, 19]. In this study we observed significantly higher betatrophin levels in the cancer group versus the cirrhotic and control groups. Our results apply to the European population with cirrhosis and HCC and are unique in this regard, as such research has not been conducted on this patient group before.
Other authors have presented data on betatrophin among women in populations without liver diseases. Increased betatrophin in women has also been observed in other studies. Gomez-Ambrozi reported a significant difference in betatrophin concentrations between the sexes: in the Caucasian population, betatrophin levels were higher in women than in men. In addition, there was a stronger negative correlation between BMI and betatrophin levels in the female group. However, the data were for overweight and obese individuals [20]. In the study by Hassan et al., noticeably higher concentrations of betatrophin were observed in women than in men, in both age groups (group 1 – 20-39 years, group 2 – 40-59 years); these concentrations were higher in younger age groups, regardless of gender (a study on an Iraqi population) [21]. However, in our study, betatrophin levels were significantly higher in women with liver cancer than in men with liver cancer.
Ma et al. confirmed that androgens influence the development of HCC. Free testosterone was inversely associated with HCC risk among men, but not in women [22]. In postmenopausal women, 4-androstenedione was inversely associated with HCC risk [23].
On the other hand, Sinclair et al. studied the impact of testosterone on the course of liver cirrhosis and observed that low free testosterone levels in men with liver cirrhosis were associated with mortality and the need for liver transplantation [24].
In line with this, in men with advanced liver disease (i.e. cirrhosis combined with HCC), a decrease in hormone levels, including testosterone, has been observed. This probably causes the decrease in betatrophin production. In contrast, in postmenopausal women, higher levels of cholesterol, sex hormone binding globulin, and free cholesterol were associated with the development of HCC [25], but also with a higher production of betatrophin.
In our study, we did not observe a significant association of betatrophin with type 2 diabetes or hypertension. In contrast to many other papers, Yue et al. performed a meta-analysis of 11 papers and showed a significant correlation between circulating betatrophin levels and T2DM. In T2DM, betatrophin concentrations are higher than in the general population. In another meta-analysis, by Li et al., higher levels of betatrophin were found in the T2DM group than in the population without diabetes, but subgroup analysis showed differences only in the subgroup with T2DM but without obesity [26]. A study of the Yue population found higher circulating betatrophin levels in the group with T2DM than in the general population, and a positive correlation of betatrophin with hypertension [27].
Interestingly, Xie made contrasting observations in a group without diabetes mellitus: higher betatrophin levels were identified in men [28].
In our study, patients with HCC were significantly older than patients in the other groups. In the Teng study, older age, male sex, family history of HCC, and HBV viral load of 2000 helped differentiate patients at risk of developing HCC [29]. Similarly, Sahil Mittal – who analyzed US veterans with HBV – singled out older age and ethnicity (Asian Pacific Islander, African American) as factors associated with higher tumor risk [30]. Additionally, actinic alkaline phosphatase and GGT were found to be significantly different in patients with HCC compared to the cirrhotic and control groups. Similar observations were made by Qin et al., who evaluated basic laboratory tests indicating HCC. In their research, the activity levels of alanine aminotransferase (ALT), aspartate transaminase (AST), alkaline phosphatase (ALP), and GGT were found to be of clear significance [31].
Changes in the WNT/B-catenin pathway are observed in more than 90% of HCC cases [32].
In our previous research, vaspin was the second most sensitive marker, regardless of etiology. Combining these markers with AFP concentration, age, and gender may allow for a better diagnostic algorithm for patients with HCC.
The use of lipid-lowering drugs, such as rosuvastatin (HMG-Co A reductase inhibitor), in patients with diabetes affects pro- and anti-inflammatory action, as well as the WNT/β-catenin pathway, and increases insulin expression. Statin use reduces the risk of developing the HCC. Currently, the role of dapagliflozin in improving cognitive functions via the WNT/β-catenin pathway is also emphasized. We did not take this factor into account in our research [33, 34].
Our study had certain limitations. It was single-center design, with an exclusively white Caucasian population. The size of the control group was small and would need to be increased in further research. Another limitation is the lack of detailed medication data and the resulting risk of residual confounding.
An additional limitation was that we tested only serum betatrophin and did not assess its levels in liver tissue, like other authors did, e.g. Wang et al. [35]. Current standards, according to the European Association for the Study of the Liver (EASL), show no need for performing a biopsy, to confirm either cirrhosis or HCC, and patients, when allowed, choose to forgo this invasive testing. It is reasonable to assume that in future we will obtain specimens for histopathological examination of the liver only in surgical cases.
Conclusions
For the first time in the course of our research, we noted a significant difference in betatrophin levels between male and female patients with HCC. Betatrophin also showed higher sensitivity in diagnosing cancer than the widely used marker AFP. The diagnosis of HCC using laboratory tests remains imperfect, but it is more widely available than imaging, and often less expensive. Therefore, we intend to continue research on this marker in women with liver cirrhosis coupled with HCC risk or established HCC. We would also like to expand our future research with assessments of selected hormones – estrogen, testosterone, and androgen – to confirm the hypothesis presented in this paper, as well as with assessment of betatrophin levels as a marker of response to treatment in patients undergoing HCC therapy.





