
The prevalence of coronary artery disease (CAD) is rising, even among younger individuals. As coronary computed tomography angiography (CCTA) becomes increasingly common in CAD diagnostics for coronary artery calcification (CAC), it allows for a comprehensive assessment of coronary arteries after contrast administration, including the visualization of atherosclerotic plaques with significant lesions or pericoronary fat thickness, which is associated with the presence and severity of CAD [1, 2].
A 48-year-old patient with dyslipidemia and hypertension, with a history of non-ST-elevation myocardial infarction (NSTEMI) treated with percutaneous coronary angioplasty of the marginal branch, and radiotherapy for non-Hodgkin’s lymphoma, was admitted for CCTA. The exertional test, performed a month before admission, was electrocardiographically positive. CCTA, assessed jointly by a radiologist and a cardiologist, revealed severe stenosis in the right coronary artery (RCA) with a high-risk lipidic plaque (Figure 1 A).
Figure 1
A – computed angiography tomography of the right coronary artery (RCA) (arrow: coronary artery calcification (CAC)). B1 – coronary angiography of RCA, before percutaneous coronary intervention (PCI) (arrow: CAC). B2 – coronary angiography of the left coronary artery (LCA), before PCI. C1 – optical coherence tomography of RCA, before PCI (arrow: lipid core). C2 – optical coherence tomography of RCA, before PCI, arrow: site of rupture). D1 – angiographic image of RCA, just after PCI. D2 – optical coherence tomography of RCA, just after PCI
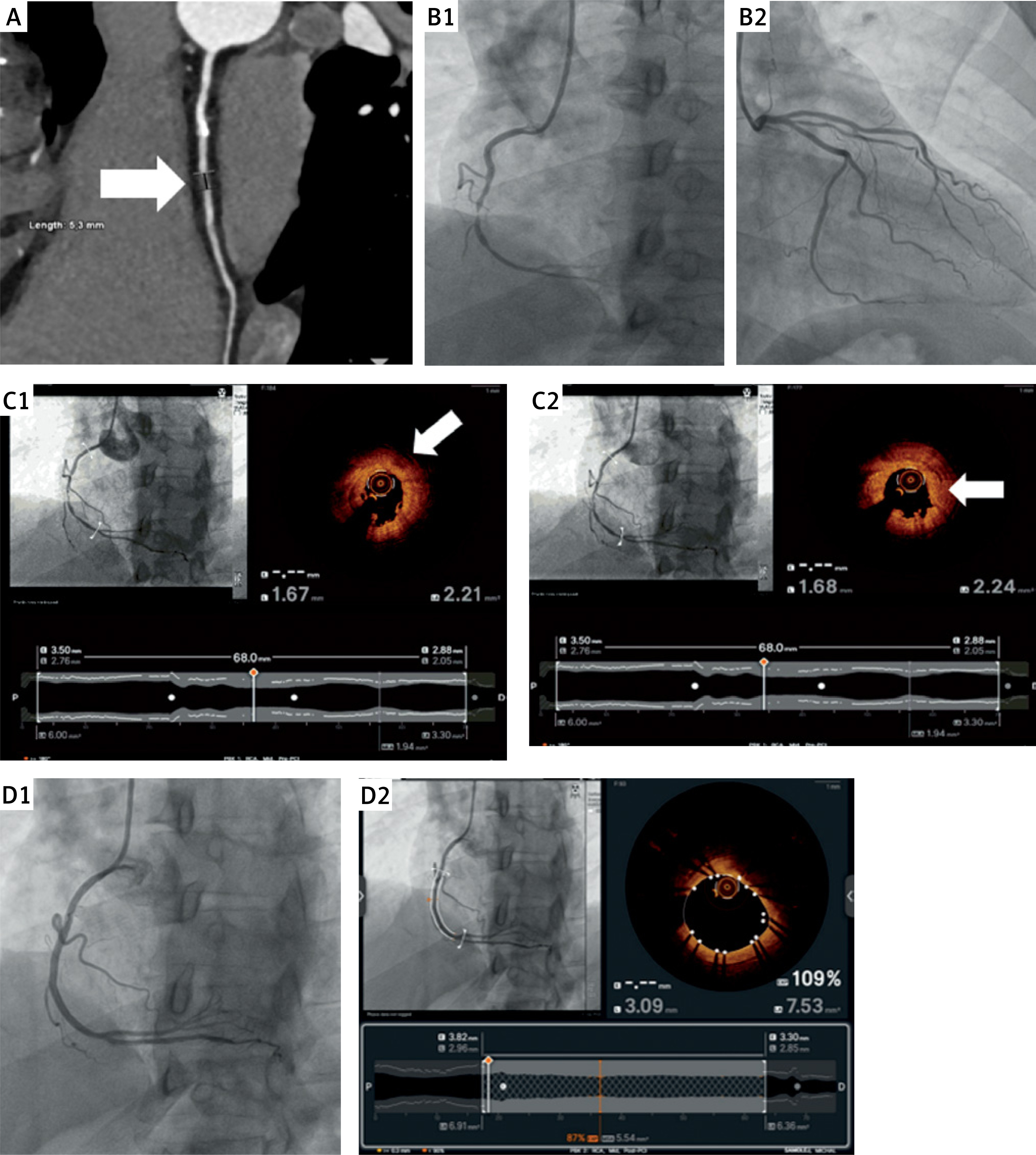
The patient was scheduled for urgent coronary angiography and admitted on the next day. While being transported to the catheterization laboratory on foot, the patient reported chest pain. The electrocardiography (ECG) performed in the catheterization laboratory showed ST segment elevation in leads II, III, and aVF. Coronary angiography revealed a critical stenosis of 99% in the middle segment of the RCA (Figure 1 B1) and only minor plaques in the left coronary artery (LCA) (Figure 1 B2). Optical coherence tomography (OCT) confirmed the presence of thin-cap fibroatheroma with lipid core (Figure 1 C1) and ruptured atherosclerotic plaque with a thrombus (Figure 1 C2), and the patient was deemed eligible for immediate coronary angioplasty. Drug-eluting stent implantation (Ultimaster 2.75 × 44 mm, 20 atm) was performed under optical coherence tomography (OCT) guidance.
The result of the procedure was optimal (Figure 1 D1). It was confirmed in OCT, which showed a minimal stent area of 5.5 mm2 and good apposition of the stent (Figure 1 D2). A day later, the patient was discharged home in good condition.
Patients with a history of major cardiovascular events (MACE), who underwent atherosclerotic plaque assessment via CCTA, showed a 3-fold increase in the rate of atherosclerosis progression compared to those without prior MACE events [3]. The use of more precise CCTA diagnostics helps identify individuals at risk of MACE more effectively. This translates into a lower long-term mortality risk and reduces the number of unnecessary coronary angiographies, supporting the implementation of a modern approach to treating such patients [4] and thereby improving their long-term outcomes.
Thanks to the cooperation between the cardiologist and the radiologist, we can more accurately determine the urgency of hospital admission for patients with CAC. Moreover, using CCTA allows us to assess anatomical variations comprehensively and select stent size appropriately, thereby performing preprocedural planning more accurately, which is part of a multidisciplinary approach for such patients.







