
Introduction
The prevalence of metabolic syndrome has been increasing worldwide, especially in the developing world compared to its western counterpart [1]. It is thought to be more common in women than in men [2, 3], particularly in the Middle East [4]. Metabolic syndrome is a significant health issue that comprises a collection of cardiovascular metabolic abnormalities including abdominal obesity, raised serum triglyceride levels, hypertension, reduced high-density lipoprotein (HDL), and raised fasting blood glucose levels [5]. Metabolic syndrome has frequently been associated with cardiovascular disease, type 2 diabetes, and all-cause mortality [5]. It has also recently been linked to increased susceptibility to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and increased severity of COVID-19 complications [6, 7]. This highlights the need for prompt management of patients with metabolic syndrome using multimodal interventions to help prevent complications associated with the condition. Conventional and recent recommendations support lifestyle interventions based on dietary caloric restriction and exercise as first-line interventions for the management of metabolic syndrome [8].
High-intensity interval training (HIIT) comprises bouts of exercise at high intensity interspersed by periods of active/passive recovery. In the last decade, a considerable number of studies have investigated the effectiveness of HIIT in metabolic syndrome [9–19]. These studies have shown that HIIT is an effective exercise strategy in metabolic syndrome management yielding significant improvements in waist circumference (WC) [9–18], serum triglycerides (TG) [10, 19], systolic blood pressure (SBP) and diastolic blood pressure (DBP) [9–18], high-density lipoproteins (HDL) [9, 19], blood glucose (BG) [10, 11, 15], and body weight and/or body mass index (BMI) [11, 13, 16, 17]. Also, HIIT combined with dietary restriction has resulted in positive changes in the cardiometabolic profile in metabolic syndrome [20, 21]. The aforementioned studies have either examined the effect of HIIT in isolation [9–19] or in combination with diet [20, 21]; however, no previous study has investigated the effectiveness of HIIT in combination with diet and carboxytherapy in the management of metabolic syndrome. Carboxytherapy or carbon dioxide (CO2) therapy has been defined as the transcutaneous administration of CO2 for remedial purposes and has been effective in the localized reduction of subcutaneous fat and waist/central adiposity [22–25]. Thus, in light of these effects, we hypothesized that carboxytherapy could be beneficial in reducing abdominal obesity and related cardiometabolic risks when combined with diet, and that the addition of HIIT to these interventions could have additional benefits in metabolic syndrome features.
Aim
Based on the above, the present study aimed to assess the effects of HIIT combined with a low-fat diet and carboxytherapy versus a low-fat diet and carboxytherapy alone on the metabolic cardiovascular risk indicators (i.e. WC, TG, SBP, DBP, HDL, and FBG) in women with metabolic syndrome. The results of this study could aid efforts directed to the prevention and/or the management of metabolic syndrome, and they may guide other researchers interested in cardiovascular disease research.
Material and methods
Ethical considerations
This study was approved by the Ethics Committee of Scientific Research of the main author’s institution (Approval No.: P.T.REC/012/002526), and it followed the tenets of the Declaration of Helsinki. Informed consent was obtained from patients before the study.
Sample size calculation
The sample size was calculated, based on previously published data [25], for the primary outcome measure (i.e. waist circumference). The power of this study was set at 80%, and the level of significance was set at a p-value of < 0.05. Sample size was calculated as follows: Sample size (n) = 2 SD2 (Zα/2 + Zβ)2/d2 [26], where: Zα/2 = 1.96 for 2-tailed results at p < 0.05; Zβ = 0.84 for a power of 80%; SD = standard deviation (estimated SD of the WC) = 5.6 (cm), [25]; d = expected effect size = absolute mean change (i.e. in the WC) = –4.5 (cm) [25]. Accordingly, n = 2 (5.6)2 × (1.96 + 0.84)2 ÷ (–4.5)2 = 24. Thus, the estimated minimum sample size was 24 patients per group. However, we aimed to recruit a total of 30 patients per group to account for a 20% drop-out rate.
Subjects
Sixty women aged from 50 to 60 years, presenting with metabolic syndrome, were enrolled in this study by referral from a physician. Inclusion criteria were metabolic syndrome diagnosed according to the National Cholesterol Education Program (NCEP) Adult Treatment Panel III [27], abdominal obesity with a waist circumference > 88 cm, body mass index 30–34.9 kg/m2, serum TG 150–200 mg/dl, blood pressure 135/85–149/89 mm Hg, serum HDL < 50 mg/dl, and FBG 100–125 mg/dl. Exclusion criteria were uncontrolled hypertension, diabetes mellitus, coronary artery or cardiac disease, chest disease, smoking, contraindications to carboxytherapy (i.e. renal failure, chronic liver insufficiency, congestive heart failure, severe respiratory insufficiency, acute infectious disease, and anti-coagulation therapy), and contraindications/limitations to exercise testing or training (i.e. cardiopulmonary, neurological, or musculoskeletal). Eligible participants were assigned equally through consecutive sampling to an experimental group that received HIIT alongside a low-fat diet and carboxytherapy, and an active control group that received a low-fat diet plus carboxytherapy only.
History taking and clinical examination
For proper patient selection, thorough medical history taking and clinical examination were performed by a physician.
Anthropometric measurements
Patients’ height, weight, waist circumference (WC), and body mass index (BMI) were recorded at baseline and after 4 weeks of the interventions. The WC was measured at the level of the umbilicus using a tape measure [28], which was kept in a horizontal plane around the waist, fitting closely to the skin without compressing it [29]. The number on the tape was recorded immediately after the patient’s exhalation [29], and each measurement was repeated 3 times and the average measurement was recorded. The body mass index (BMI) was calculated as body weight in kilograms divided by the height in metres squared [30].
Blood biochemical analysis
Twelve-hour fasting serum triglycerides (TG), 12-hour fasting high-density lipoproteins (HDL), and 6–8-hour fasting blood glucose (FBG) were measured at baseline and after 4 weeks. These were run in an automated chemistry analyser (Erba Mannheim, Model: Chem-7, SR. NO.: 9155, Germany).
Blood pressure measurements
Blood pressure was measured by a mercury sphygmomanometer with the arm supported at heart level while the patient was at complete rest. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were reported at baseline and after 4 weeks.
Symptom-limited maximal exercise test
Patients in the experimental group were eligible for exercise testing and underwent a symptom-limited maximal treadmill exercise test according to the modified Bruce protocol at baseline to record their peak heart rate (HRpeak) necessary to determine the target heart rate/exercise intensity on an individual basis [31]. The modified Bruce protocol has seven 3-min stages and starts with a zero inclination at a speed of 1.7 miles/hour (stage 0) and is then graded to 5% (stage 0.5) and 10% (stage 1) inclinations at the same speed [31]. From then on, the treadmill speed and inclination should be increased until the last stage, as described by Noonan and Dean [31]. During the test, the individual’s heart rate was continuously monitored using fingertip pulse oximetry (Yuwell, YX300, SR. no. 190800170, China). Patients were monitored for any symptoms or signs that warranted exercise test termination (e.g. chest pain/discomfort, severe breathlessness, severe leg pain/fatigue, confusion, dizziness, presyncope, pallor, staggering, or diaphoresis). Patients underwent the test safely and stopped because of volitional exhaustion. Immediately after the test, the peak heart rate (HRpeak) of each patient was recorded.
Interventions
Patients in both groups received a low-fat diet and carboxytherapy for 4 weeks, while only patients in the experimental group received HIIT in addition to this combination over the same timeframe. No pharmaceutical treatment was administered to patients in the 2 groups throughout the course of the study.
Low-fat diet
A low-calorie (1000–1200 calories/day), low-fat diet was prescribed for patients in both groups for a 4-week period, as recommended by Castro-Barquero et al. [32], and was composed of (a) less than 30% of daily calories fats including around 20% monounsaturated and polyunsaturated fatty acids and less than 10% saturated fatty acids, (b) 15–20% of daily calories in proteins, and (c) 50–55% of daily calories in carbohydrates. The diet plan emphasized foods with reduced total fat content (e.g. foods prepared without the addition of butter, low-fat dairy products, and lean protein sources), whole grains, fruits, vegetables, herbs and spices, and foods low in sodium. The patient’s compliance with the diet regimen was checked every week throughout the study.
Carboxytherapy
Patients in both groups received carboxytherapy for 4 consecutive weeks using a carboxytherapy unit (Carbo-5000, Daeyang Co., SN2012009, Korea). After disinfection of the areas, subcutaneous injection of carbon dioxide (CO2) was applied to the abdomen bilaterally in the paraumbilical area, with a total gas dose of 150 ml per session, twice a week [22]. The abdominal region was divided into lines parallel to the umbilicus, and each line consisted of points 5 cm apart. The CO2 was injected vertically 1–2 cm deep, with a dose of 5 ml per point using a 30-gauge syringe at an infusion velocity of 100 ml/min [33]. Apart from the pain from the needle, the unpleasant burning sensation felt in the treated sites lasting for < 1 min, and/or the occasional capillary bleeding in some injection areas, no serious adverse effects of carboxytherapy were reported throughout the study.
High-intensity interval training (HITT)
HIIT was prescribed only in the experimental group, according to Tjønna et al. [9], for 4 consecutive weeks, using the “FITT” principle of exercise prescription laid down by the American College of Sports Medicine [34], as follows: Frequency: 3 days/week on alternate days. Intensity: 4 working bouts were set at a target heart rate of 85–90% of peak heart rate (HRpeak), and 3 active recovery bouts were set at 60–70% of HRpeak. Treadmill speed and inclination were adjusted between the working and recovery bouts to achieve the target heart rate. To ensure that the patients were exercising at their individually prescribed target heart rate, a fingertip pulse oximeter (Yuwell, YX300, SR. No.:190800170, China) was used for heart rate monitoring. Low-intensity walking was used for the warm-up and cooling-down. Time (Duration): each session lasted about 33 min: 5-min warm-up, 16-min working bouts (4 min each), 9-minute recovery bouts (3 min each), and 3-minute cool-down. Type/mode: interval exercise training: 4 high-intensity intervals interspersed with 3 active recovery intervals. Modality: An electrical treadmill (LSG, SN321125, 2014, Taiwan) was used with adjustable speed (from 1 to 18 km/h) and inclination (from 0 to 15%).
Statistical analysis
The normal distribution of data was checked by the Kolmogorov-Smirnov test. Square root transformation was needed for some data (i.e. SBP data) to achieve the normal distribution. The homogeneity of variances between groups was checked by Levene’s test. Then, the unpaired t-test was used to compare the means between the 2 groups at baseline and post-intervention, and the paired t-test was used to compare the means of the paired measurements within each group. Welch’s t-test was used for normally distributed data with unequal variance between groups (i.e. TG data) to analyse the difference in the means between the 2 groups. Non-parametric statistics were used for the data with an abnormal distribution that failed the normality test after data transformation (i.e. DBP data). Wilcoxon Signed-Rank test was used to analyse the changes within each group, and the Mann-Whitney U test was used to assess the difference between the 2 groups. The absolute mean change from baseline (Δ) of each variable was considered an independent outcome and was statistically analysed between groups by the unpaired t-test or the Welch’s t-test. Mean differences (MD) between groups and 95% confidence intervals (CI) were determined. P-values < 0.05 were considered statistically significant. Social Science Statistics and GraphPad Prism software were used for statistical analysis.
Results
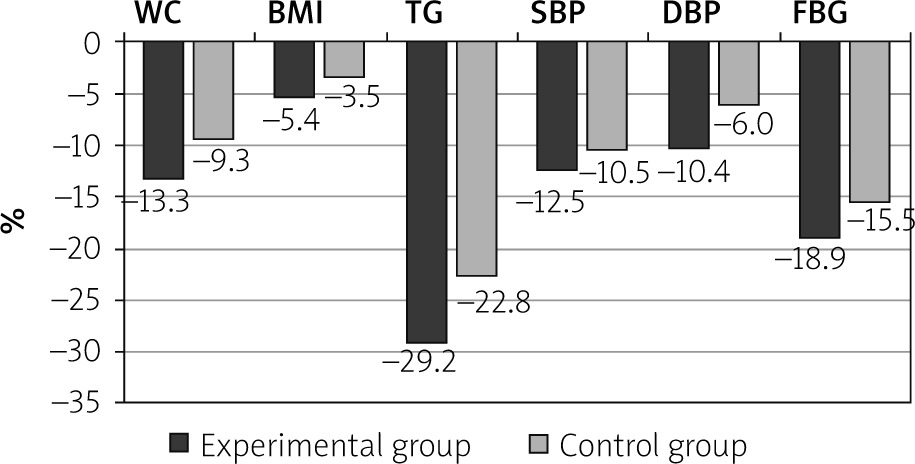
At baseline, there were no significant differences between groups in patients’ age and anthropometric characteristics (Table I) or in the outcome measures except for the DBP (Table II). After the treatment, there were significant differences in waist circumference, BMI, triglycerides, systolic blood pressure, diastolic blood pressure, high-density lipoproteins, and fasting blood glucose (p < 0.001) in both groups compared to the baseline (Table II). The experimental group demonstrated significantly greater improvements in mean values of waist circumference (p < 0.001), BMI (p = 0.031), triglycerides (p < 0.001), systolic blood pressure (p = 0.026), diastolic blood pressure (p = 0.001), and fasting blood glucose (p = 0.003) compared to the control group (Table II). There was an observed difference in the mean value of HDL between the 2 groups in favour of the experimental group, which tended towards significance (p = 0.075), as shown in Table II. The absolute mean change from baseline (Δ) was significantly different between the 2 groups in favour of the experimental group for ΔWC (p < 0.001), ΔBMI (p < 0.001), ΔTG (p < 0.001), ΔSBP (p = 0.014), ΔDBP (p < 0.001), ΔHDL (p = 0.008), and ΔFBG (p < 0.001), as shown in Table II. Percentage reductions of the outcome measures post-intervention for the 2 groups are presented in Figure 1.
Table I
Age and baseline anthropometric characteristics of patients in the 2 groups
Table II
Results for outcome measures in the 2 groups pre- and post-intervention
[i] Data are presented as mean ± SD and as mean differences (MD) and 95% confidence intervals (CI). HIIT – high-intensity interval training. Δ absolute change from baseline. *Significant p-value (< 0.05) based on the paired t-test, **significant p-value (< 0.05) based on the unpaired t-test, ‡significant p-value (< 0.05) based on Welch’s t-test, $significant p-value (< 0.05) based on the Wilcoxon Signed-Rank test, #significant p-value (< 0.05) based on the Mann-Whitney U test.
Discussion
Our study is the first study to investigate the addition of HIIT to a low-fat diet and carboxytherapy in metabolic syndrome. In agreement with our hypothesis, we have demonstrated that the addition of HIIT to a low-fat diet and carboxytherapy elicited significantly better improvements in waist circumference, BMI, triglycerides, systolic blood pressure, diastolic blood pressure, high-density lipoproteins, and fasting blood glucose compared to the low-fat diet and carboxytherapy alone. The present study also showed that both multimodal interventions resulted in significant improvements in the aforementioned variables compared to baseline.
We can partly attribute our results in the 2 groups to the low-calorie, low-fat diet implemented in the present study. Calorie-restricted dietary plans proved effective for inducing improvements in metabolic cardiovascular disturbances in metabolic syndrome in terms of reducing waist circumference, BMI, systolic and diastolic blood pressure, and triglycerides and increasing HDL levels [34]. A low-fat diet was found to reduce the risk of metabolic syndrome, minimize the use of anti-hypertensive and blood lipid-lowering medications [35], and reduce premature all-cause mortality in obese adults [36]. Recently, a low-fat diet was found to be more effective for weight loss, blood pressure control (↓ SBP, ↓ DBP), and blood lipid control (↑ HDL, ↓ LDL levels) compared to a normal diet [37, 38].
Our findings in the 2 groups can also partly be attributed to carboxytherapy. Several studies have shown that carboxytherapy is effective in adipocyte destruction and reduction of abdominal adiposity and/or waist circumference [22–25]. The mechanism underlying the lipolytic effect of carboxytherapy can be explained by the appearance of thin fracture lines in the plasma membrane of adipocytes following carboxytherapy without damaging the connective tissues comprising the vascular and nervous structures, with a subsequent release of triglycerides in the intercellular spaces [22]. In addition, the diameter of adipocytes was significantly minimized following CO2 injection compared to air injection in rat models [39].
The major finding in the present study was the significantly greater improvement in the metabolic cardiovascular risk factors reported in the experimental group compared to the control group. This finding can be solely attributed to the HIIT, and it can be explained by several physiological adaptations/responses, as described by Serrablo-Torrejon et al. [40], as follows: (a) HIIT-mediated reduction in waist circumference, an effect that was reported in metabolic syndrome by many studies [9–18]. The HIIT-induced decrease in WC can be related to reduced visceral or abdominal fatness owing to excess post-exercise oxygen consumption (EPOC) and increases in fat oxidation during recovery periods of HIIT [41]. These responses occur to replenish muscle oxygen and energy stores that were depleted during the work periods of training. EPOC has been positively correlated with exercise intensity, and so HIIT has a greater effect than other exercise forms of a lower intensity [42]. To add, ATP is re-synthesized during recovery intervals of HIIT by aerobic metabolism utilizing free fatty acids transported from triglyceride stores in adipose tissue, which is correlated with the fat loss [43]. (b) HIIT-induced weight loss/BMI reduction [11, 13, 16, 17]. This could be explained by the aforementioned physiological responses and by the effect of HIIT on appetite control [44]. HIIT has been found to suppress appetite (↓ hunger and ↑ satiety) by reducing ghrelin hormone and increasing glucagon-like peptide 1 (GLP-1) hormone in blood circulation [44]. Reduced appetite has shown a significant correlation with weight loss in overweight/obese subjects [45]. (c) HIIT-mediated decrease in plasma TG, a response that has been previously reported in patients with metabolic syndrome [10] and dyslipidaemia [19], and can be predominantly caused by the reduction in very low-density lipoprotein-triglyceride (VLDL-TG) concentration following training, as found by Tsekouras et al. [46]. (d) HIIT-induced reductions of SBP and DBP, which were found to be greater than other modes of training [47]. Numerous studies have demonstrated that HIIT can induce significant decreases in SBP and DBP in patients with metabolic syndrome [9–18]. Possible explanations include decreases in circulating catecholamines and peripheral resistance, as well as improved baroreflex control of the sympathetic nervous system [48]. (e) HIIT-mediated increase in HDL, an effect that was found in patients with metabolic disorders [9, 19], and/or obese women [49]. A higher expression of ATP-binding cassette transporter A1 mRNA, a key player in plasma HDL biogenesis, as well as increased activity of lecithin–cholesterol acyltransferase, a key enzyme for transferring free cholesterol into cholesteryl ester and HDL formation, may be involved in the HIIT-mediated increase in HDL levels [50]. (f) HIIT-induced reduction in FBG, an adaptation that is due to increases in skeletal muscle mass, insulin receptors/sensitivity, blood flow, and skeletal muscle GLUT-4 expression with a consequently increased blood glucose disposal into the skeletal muscle [51]. Several studies have shown that HIIT induced significant reductions in blood glucose in metabolic syndrome [10, 11, 15]. HIIT also induced a significant decrease in average blood glucose levels compared to the non-exercising group in type 2 diabetes [52].
It is worth noting that HIIT plus dietary intervention has shown significant improvements in BMI, FBG, HDL, and TG compared to diet alone in metabolic syndrome [20]. More recently, HIIT in combination with diet restriction has shown significant changes in BMI, WC, SBP, and DBP compared to baseline values in metabolic syndrome [21]. Furthermore, interval training in combination with a low-calorie diet has induced positive changes in body weight and serum TG levels in patients with metabolic syndrome [53]. Although we did not examine the effect of HIIT plus diet alone, these studies [20, 21, 53] did, and their results revealed favourable therapeutic benefits of this combination.
Finally, our findings should be viewed considering some limitations. The major limitation of this study is the lack of randomization with a possibility of a selection bias which may limit the generalization of the results. Other limitations of this study include the lack of determination of the isolated effect of carboxytherapy in patients with metabolic syndrome. Also, only female patients were enrolled. Nevertheless, our study has several strengths. This is the first study to investigate the combined effect of low-fat diet and carboxytherapy with and without HIIT in metabolic syndrome. Also, the sample size was calculated to improve the determination of clinically relevant treatment effects.
Conclusions
The findings of the present study suggest that the use of a 4-week HIIT, as an addition to a low-fat diet plus carboxytherapy, could lead to more reductions of metabolic cardiovascular risk factors in women with metabolic syndrome (i.e. ↓ WC, ↓ TG, ↓ SBP, ↓ DBP, ↑ HDL, and ↓ FBG) than the use of a low-fat diet and carboxytherapy alone. Nevertheless, a low-fat diet plus carboxytherapy without HIIT could help reduce the risk factors related to metabolic syndrome in women. Further research could produce more conclusive evidence.











