
Introduction
Chronic pelvic pain affects about 26% of the world’s female population [1] . It is defined as pain originating from the pelvis, typically lasting more than 6 months related to conditions such as gynaecological disorders, interstitial cystitis or painful bladder syndrome, irritable bowel syndrome, vulvodynia, and pelvic floor muscle tension [2, 3]. Pain could also be linked to the structure of myofascial tissues in the abdominal and pelvic areas, but the mechanisms are often unclear [4]. The most common debilitating conditions are dysmenorrhea, related to menstruation and dyspareunia, related vulvodynia, chronic pelvic pain, including low back pain (LBP) during pregnancy. These pathologies impact not only physical health, but also quality of life, sexual function, mental well-being, and the ability to participate in daily activities [5, 6]. These conditions often overlap with nonpelvic pain disorders (e.g., fibromyalgia, migraines) and other comorbidities (e.g., sleep, mood, cognitive impairment) to contribute to pain severity and disability [1].
Various treatments could be used to reduce pain and improve health. These patients often have pelvic floor muscle dysfunction, which can be improved through physiotherapy focused on relaxation techniques and pelvic floor re-education [7].
Transcutaneous electrical nerve stimulation (TENS) is a widely used physical therapy modality for pain management and relief. Transcutaneous electrical nerve stimulation involves the application of low-voltage electrical currents through the skin to stimulate peripheral nerves. Its analgesic effects are primarily attributed to mechanisms such as activation of large-diameter Aβ fibres, which inhibit pain transmission according to the gate control theory, and stimulation of endo genous opioid release, including b-endorphins [9] ( Figure 1 ).
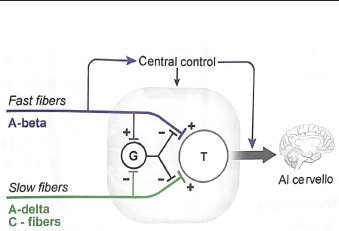
Furthermore, it is supported by the physiological evidence showing inhibition of central nociceptive neurons regardless of diagnosis [10, 11]. Transcutaneous electrical nerve stimulation devices are typically inexpensive and readily available without the need for a prescription. Furthermore, they can be safely self-administered. Despite recent research, uncertainty about TENS efficacy and effectiveness persists nowadays. According to the National Institute for Health and Care Excellence Guidelines (2021), the use of TENS is not supported for chronic primary pain, intrapartum care, and non-specific LBP [12, 13].
It is most frequently used in rehabilitative programs regarding musculoskeletal diseases, like osteoarthritis and rheumatoid arthritis [14, 15].
Recently, TENS has shown promising results in alleviating pelvic pain and improving sexual function, particularly in cases of dysmenorrhea and vulvodynia.Primary dysmenorrhea (PD) is one of the most prevalent causes of pelvic pain in reproductive-age women; it is characterized by the association not only with menstrual cramping but also with alterations in pelvic floor sensitivity and myofascial trigger points. These features suggest a multifactorial pain aetiology [16, 17].
Vestibulodynia, instead, is characterized by localized provoked pain at the vulvar vestibule, often accompanied by dyspareunia, pelvic floor dysfunction, and low sexual quality of life [18].
Both dysmenorrhea and vestibulodynia underline the complex interplay of nociceptive, myofascial, and central sensitization mechanisms contributing to persistent pelvic pain in women. Transcutaneous electrical nerve stimulation could be a non-pharmacological neuromodulation strategy that could improve treatment of these conditions. Previous systematic reviews and randomised controlled trials (RCT) report that TENS may modestly reduce pain intensity in PD and chronic pelvic pain, and specific TENS protocols have demonstrated beneficial effects on burning pain and dyspareunia in women with provoked vestibulodynia [19, 20].
It is important to underline that pelvic pain encompasses heterogeneous conditions with distinct but overlapping mechanisms. This complexity supports the need for multimodal therapies which may address both nociceptive and neuromuscular components of pelvic pain.
This review aims to provide an updated synthesis of RCTs on the use of TENS for managing pelvic pain in women, with a focus on secondary functional and rehabilitative outcomes.
Material and methods
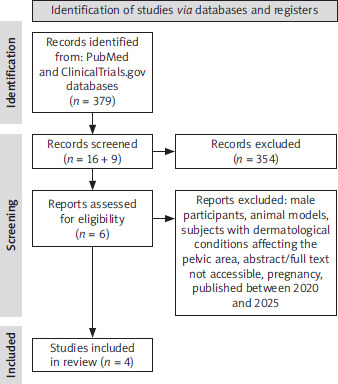
A bibliographic search was performed using the PubMed and ClinicalTrials.gov databases. The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords. The following search string was used: ((“Transcutaneous Electric Nerve Stimulation”[Mesh] OR TENS OR “electrical nerve stimulation” OR “transcutaneous electrical stimulation”) AND ((“Dysmenorrhea”[Mesh] OR “primary dysmenorrhea” OR “menstrual pain”) OR (“Vulvodynia”[Mesh] OR “vulvar pain” OR “vestibulodynia” OR “vulvar vestibulitis”))) AND (“Randomized Controlled Trial”[Publication Type] OR randomized[Title/Abstract] OR sham[Title/Abstract] OR placebo[Title/Abstract]).
Filters were applied to restrict the results to studies involving humans, female participants, and articles published in English. We selected papers from January 2020 to December 2025. Additional filters included article type (RCT) and age categories (adolescent and adult populations). The reference lists of the included studies were manually screened to identify any additional relevant publications.
In accordance with the PICO model [21], we considered eligible RCTs satisfying the following criteria:
P (population): adult women (aged > 18 years) diagnosed with pelvic pain. Male participants, animal models, individuals with dermatological conditions affecting the pelvic area, pregnant women were excluded,
I (intervention): TENS,
C (comparison or control(s): no specific comparators were considered in this review,
O (outcome): pain reduction.
All articles underwent independent evaluation by two reviewers (RC and PEF). Disagreements between the two independent reviewers were resolved through discussion and mutual consensus. In cases of divergent opinions, final decisions were made based on the overall methodological consistency of the review. No conflicts of interest were reported by any of the reviewers.
Evidence acquisition registration
We used the PRISMA reporting guidelines when writing this report [22]. This review was prospectively registered in the PROSPERO database before commencing the literature search and it is available at https://www.crd.york.ac.uk/prospero; ID number 1151312. The methodological quality of the included studies was assessed using the Cochrane risk of bias tool through the RevMan software (https://revman.cochrane.org/info). This software provided the evaluation of seven key domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential sources of bias. Each domain was judged as having a low, unclear, or high risk of bias, and results were visually summarized using a colour-coded system: green for low risk, yellow for unclear risk, and red for high risk (Figure 2).
Results
The included RCTs, published between 2021 and 2024, involved a total of 281 participants (154 in the intervention groups and 127 in the control groups). All studies enrolled female populations, with mean ages ranging from 17 to 31 years. The most frequently investigated condition was PD, addressed in three trials [23–25], while only one study focused on vestibulodynia [20]. Although all studies used TENS as the main intervention, substantial heterogeneity was observed in terms of devices, stimulation parameters, administration modalities, and treatment duration. Murina et al. [20] adopted an intravaginal, self-administered home-based protocol combining high- and low-frequency stimulation for 30 minutes, three times per week, over a 120-et al. day period. In contrast, the PD trials exclusively employed transcutaneous approaches: Guy et al. [23] used adhesive patches with variable frequencies (60–100 Hz), McLagan et al. [24] applied a commercial wearable device delivering stimulation (50–100 Hz), and Manisha and Anuradha [25] administered high-frequency stimulation (100 Hz) for 20 minutes on the first day of menstruation. All included studies reported a significant reduction in pain in study groups. Murina et al. [20] observed significant improvements in burning pain and dyspareunia, but no statistically significant changes in secondary outcomes (female sexual functioning index – FSFI, vulvar pain functional questionnaire, pelvic floor muscle strength), suggesting a predominantly analgesic effect of moderate clinical relevance. In the PD trials, Guy et al. [23] reported a mean pain reduction of 53%, associated with a rapid onset of action and a marked decrease in analgesic consumption, indicating a large and clinically meaningful effect. Similarly, McLagan et al. [24] demonstrated a significant reduction in pain across all cycles and a lower use of non-steroidal anti-inflammatory drugs (NSAID), suggesting at least a moderate treatment effect. Manisha and Anuradha [25] found significant intra- and intergroup differences for all assessed outcomes, consistent with a robust analgesic response. Only two studies documented a significant reduction in analgesic consumption [23, 24], whereas Murina et al. [20] did not observe significant improvements in sexual function or muscle performance.
The methodological quality of the included studies was assessed using the Cochrane risk of bias tool available through the RevMan software (https://revman.cochrane.org/info) (Figure 3).
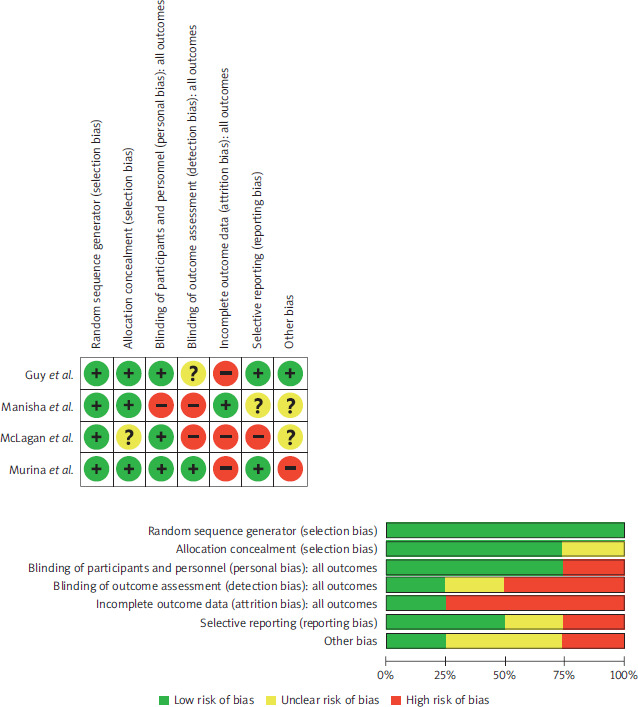
The risk of bias assessment revealed substantial concerns in several domains, particularly regarding detection bias, incomplete outcome data, and selective reporting. Only one study [20] was judged to be at low risk of detection bias, while two [24, 25] were rated as high risk. Small sample sizes, heterogeneous follow-up durations (ranging from immediate post-treatment assessments to 120 days), and non-standardized protocols further reduce the robustness of the findings.
Consequently, although the available evidence suggests a potentially clinically meaningful benefit of TENS in the management of pelvic pain, the heterogeneity of protocols, the lack of standardized effect size reporting, and the overall methodological limitations prevent definitive conclusions. Larger, well-designed RCTs with standardized protocols and complete outcome reporting are required to enable a precise quantification of treatment effects and to improve the comparability of future findings (Table 1).
Table 1
Characteristics of the study
| Author [year] | Study design | Pathology | Study group | Control group 1 | Outcome measure | Follow-up | Results |
|---|---|---|---|---|---|---|---|
| Murina et al. [20] | RCT | VBD | TENS (EVA; Sirval) Vaginal probe (Periprobe VAG2ST; Sirval) self-administered domiciliary protocol 15 min of 100 Hz frequency, a pulse width of 50 μs, and time on : off 20 : 10 s (first program) followed by 15 min of 5 Hz frequency, a pulse width of 100 μs, and time on : off 20 : 10 s (second program) 3/week No. of patients = 40 → 39F Mean age 27.0 | TENS 15 min of 60 Hz frequency, a pulse width of 50 μs, and time on : off 20 : 10 s (first program) followed by 15 min of 5 Hz frequency, a pulse width of 200 μs, and time on : off 20 : 10 s (second program) 3/week No. of patients = 40 → 39F Mean age 27.7 | VAS (burning/pain + dyspareunia score); V-Q FSFI PFM activity at rest PFM peak activity PFM strength | T0: baseline T1: day 60 T2: day 120 | At T2 in the study group, improvement: burning/ pain (p = 0.003) and dyspareunia (p = 0.01) VAS scores Improvement not statistically significant: FSFI, V-Q, and muscle-strength measures |
| Guy et al. [23] | RCT | PD | TENS (menstrual cycle 1) → Sham (menstrual cycle 2) (Patch d’électrothérapie URGO) Program 1: continuous high frequency (100 Hz) Program 2: different frequencies (60 Hz, 80 Hz and 100 Hz) in continuous and discontinuous mode 15 intensity levels 30 min treatment max 6 times/day No. of patients = 20 → 19F Mean age 29.2 ±6.1 | Sham (menstrual cycle 1) TENS (menstrual cycle 2) No. of patients = 20 → 18F Mean age 29.7 ±7.1 | VAS Speed of action Persistence of the effect Therapeutic savings Satisfaction | T0: baseline T1: + 5 days after the end of menses of cycle 1 T2: + 5 days after the end of menses of cycle 2 | In favour of TENS: • significant decrease in the pain of 53% (p < 0.0001), • rapid relief, less than 20 minutes in 74%, • difference in analgesic consumption of –93% (p < 0.01) |
| McLagan et al. [24] | RCT | PD | TENS (Therabody PowerDot®) Uno (single unit)/duo (dual unit)/control (NSAID) in randomised order Continuous HF (50–100 Hz) with a phase duration of 100 μs from 30 to 90 min treatment No. of patients = 34 → 26F Mean age 24.6 ±3.4 | NRS | T0: pre use T1: post use | Significant reduction in pain during the Control (–3.52 ±1.9), Uno (–2.10 ±1.6), and Duo (–2.19 ±1.7) cycles (p < 0.001) Difference in the doses of NSAID during the Control cycle (3.5 ±2.6), compared with that of Uno (1.5 ±3.0), or Duo (1.1 ±2.6) (p = 0.004) | |
| Manisha et al. [25] | RCT | PD | TENS (Stim Tec4) root level L3–L5 Frequency 100 Hz, pulse duration 80 μs, intensity up to the tolerated level 20 min on the first day of menstruation No. of patients = 70F Mean age 17.21 ±1.178 | No. of patients = 70F Mean age 17.50 ±1.327 | NRS pain (lower abdomen Referred lower back Referred bilateral thigh) Systolic blood pressure | T0: pre use T1: post use | Significant difference in intragroup and intergroup comparison of all the outcome variables |
Discussion
The present review provides an updated synthesis of RCTs published in 2020–2025 on the use of TENS for the management of pelvic pain in women. The review focuses on secondary functional and rehabilitative outcomes in addition to pain reduction, in comparison with previous systematic reviews, including the recent one by Han et al. [26].
The collective evidence from these four studies suggests potential efficacy of TENS in reducing pelvic pain in women, particularly in conditions such as PD and vestibulodynia, with benefits primarily observed in analgesic outcomes, as pain intensity was the main endpoint assessed across all included trials.
These findings are consistent with those reported in previous systematic reviews. For instance, the analysis conducted by Igwea et al. [27], published in 2016, demonstrated significant reductions in dysmenorrheic pain following TENS application. Similarly, Proctor et al. [28] reported that high-frequency TENS was superior to both placebo and low-frequency TENS in alleviating pain in women with primary dysmenorrhea.
The analgesic efficacy of TENS is further supported by the findings of Fernández-Pérez et al. [29], whose systematic review, focusing on women with dyspareunia, reported similar outcomes. However, it should be noted that the studies included in their analysis predate the present review period and exhibit substantial methodological heterogeneity.
Furthermore, there is evidence to suggest that the use of TENS has been associated with a decreased use of medications, particularly NSAID, as shown by McLagan et al. [24]. However, a comprehensive systematic review by Johnson et al. [30], which encompassed 381 studies across a wide range of clinical conditions, reported only low-certainty evidence that lends support to the conclusion that TENS is superior to pharmacological analgesia.
In contrast to the relatively consistent evidence supporting the analgesic effects of TENS, findings related to functional and rehabilitative outcomes remain limited and less conclusive. Outcomes, such as sexual function, pelvic muscle strength, and overall functional performance were assessed in only a small number of studies and were not consistently included as primary endpoints, thereby limiting the strength of the conclusion that can be drawn regarding the rehabilitative effects of TENS.
While evidence from other clinical populations suggests potential benefits of TENS on quality of life and functional capacity, such findings cannot be directly extrapolated to women with pelvic pain and should be interpreted with caution.
For instance, Katirci Kirmaci et al. [31] examined the impact of different electrical stimulation modalities on pain, functional capacity, and quality of life in patients with multiple sclerosis, employing the multiple sclerosis international quality of life scale. While both interferential current therapy and TENS demonstrated significant improvements in pain and functional capacity, TENS was found to be more efficacious in enhancing quality of life. The findings are derived from a non-pelvic pain population and therefore provide only indirect support for potential functional benefits of TENS in pelvic pain conditions.
With regard to the specific issue of pelvic pain, Mira et al. [32] provided relevant evidence by comparing hormonal therapy and TENS in patients with endometriosis. Their results demonstrated significant improvements in sexual function, particularly in the lubrication and pain domains of the FSFI, in the group receiving TENS. However, these findings are limited to a specific clinical population and treatment context, and therefore offer supportive but not generalizable evidence regarding the potential functional benefits of TENS in women with pelvic pain.
Despite the paucity of research investigating the cost-benefit profile of TENS in the context of pelvic pain and pelvic floor dysfunctions, it may represent a potentially cost-effective option. This is attributable to its non-invasive nature, low risk profile, and ease of administration. Supporting evidence from other clinical areas, such as the review by Woods et al. [33], which compared the cost-effectiveness of various non-pharmacological treatments for knee osteoarthritis, indicated that TENS represents a cost-efficient therapeutic option when all available trials are taken into consideration.
The findings of the present review can be interpreted in terms of their clinical implications. It is suggested that TENS may be considered as an adjunctive, non-pharmacological option for the management of pelvic pain in women, primarily due to its analgesic effects, particularly in the specific clinical conditions for which evidence is currently available. Additionally, TENS may have the potential to reduce reliance on pharmacological treatments; however, this effect has been directly assessed in only a limited number of studies and should therefore be interpreted with caution. While preliminary evidence suggests the possibility of benefits on secondary outcomes, including sexual function and functional performance, the current evidence supporting these rehabilitative effects remains limited and insufficient to draw firm conclusions.
Consequently, TENS should be regarded primarily as a symptomatic intervention rather than a comprehensive rehabilitative approach for addressing broader functional impairments.
This review has limitations that should be acknowledged when interpreting the findings. Firstly, the number of eligible studies included is limited, which restricts the overall strength and generalizability of the evidence.
Substantial heterogeneity was observed among the studies in terms of TENS application protocols, including electrode placement, stimulation parameters and follow-up periods. This variability complicated direct comparison of results and limited the possibility of defining standardized treatment parameters for clinical practice.
The control conditions differed across studies, ranging from sham stimulation to alternative TENS settings or no treatment. Such methodological differences have the potential to introduce bias in the interpretation of comparative outcomes and may influence effect sizes.
While pain reduction was consistently assessed as the primary outcome, secondary outcomes such as sexual function, pelvic floor muscle strength, and overall functional performance have been less frequently and less rigorously investigated. The limited attention paid to these parameters prevents a comprehensive evaluation of TENS as a rehabilitative tool beyond its analgesic effects.
The duration of the follow-up periods was generally limited, with only one study extending to 120 days. This limits the understanding of the long-term efficacy and sustainability of TENS-induced improvements, as well as its potential role in chronic pain management and relapse prevention.
Additionally, the studies reviewed did not systematically evaluate cost-effectiveness, patient adherence, or satisfaction, factors that are crucial for translating clinical efficacy into practical implementation.
Finally, publication bias cannot be excluded. Studies reporting positive outcomes are more likely to be published, which may overestimate the apparent effectiveness of TENS in the treatment of pelvic pain. In addition, potential conflicts of interest in the included studies may further influence the reported outcomes and should be taken into consideration when interpreting the findings.
It is therefore evident that future research should address the aforementioned limitations through more systematic and methodologically robust investigations. There is a need for large-scale, multicentre RCTs with harmonization of the parameters used, in order to facilitate the development of clinical guidelines. Moreover, future studies should adopt a multidimensional approach, assessing not only pain intensity but also functional outcomes and overall quality of life. Finally, long-term follow-up assessments are essential to evaluate the sustainability of the beneficial effects of TENS.
Conclusions
The present review indicates that TENS may be effective in reducing pelvic pain in women, particularly in conditions such as dysmenorrhea and vestibulodynia, with consistent evidence for analgesic effects. Evidence regarding secondary functional and rehabilitative outcomes, including sexual function and pelvic muscle performance, remains limited and inconclusive.
Transcutaneous electrical nerve stimulation may be considered as an adjunctive, non-pharmacological option for pain management, potentially reducing reliance on medications. However, given the small number of studies, heterogeneity of protocols and limited long-term follow-up, it should be regarded primarily as a symptomatic intervention rather than a comprehensive rehabilitative approach.
Future research should focus on large-scale, multicentre RCTs with standardized protocols, multidimensional outcome assessment, and long-term follow-up to clarify both analgesic and functional benefits and guide clinical practice.








