
A 64-year-old man with hypertension and type II diabetes presented with an inferior ST-elevation myocardial infarction (STEMI) (Figure 1 A, baseline 12 leads electrocardiogram (ECG)) within 2 h of symptom onset. He was loaded with aspirin and ticagrelor, and 8000 units of unfractionated heparin were administered intravenously (iv). Urgent coronary angiography performed via the right radial artery showed an ostial acute thrombotic occlusion of the infarct-related coronary artery (RCA) (Figure 1 A) with Thrombolysis in Myocardial Infarction (TIMI) grade 0 flow in a left non-dominant unobstructed coronary artery system. After achieving flow with a workhorse guidewire crossing, a severe proximal RCA stenosis with a large thrombus burden (LTB) was revealed (Figure 1 B). To prevent microvascular distal embolization (DE) and the no-reflow (NR) phenomenon [1], up-front iv GpIIb/IIIa tirofiban 25 µg/kg bolus and guide catheter directed intracoronary thrombolysis (ICT) with 10 mg of alteplase were administered without any prior thrombus modification technique such as manual aspiration thrombectomy (MAT) or ballooning. We felt that in the absence of coronary-specific power aspiration catheters, conventional MAT would be ineffective in such an LTB vessel and would probably provoke thrombus migration and embolization. Half an hour after ICT, electrocardiography showed an accelerated idioventricular rhythm, which was well tolerated (Figure 1 C, Cath Lab hemodynamic monitoring system), and angiography demonstrated successful reperfusion with complete thrombus resolution (Figure 1 C). Predilation of the proximal RCA stenosis with a semi-compliant balloon (3.0 × 15 mm) was followed by intravascular ultrasound-guided implantation of a Resolute Onyx 5.0 × 18 mm drug-eluting stent. An excellent angiographical result was obtained following post-dilation with a non-compliant 6.0 × 8 mm balloon (Figure 1 D), with a non-Q MI evolution (Figure 1 D, post-procedure ECG).
Figure 1
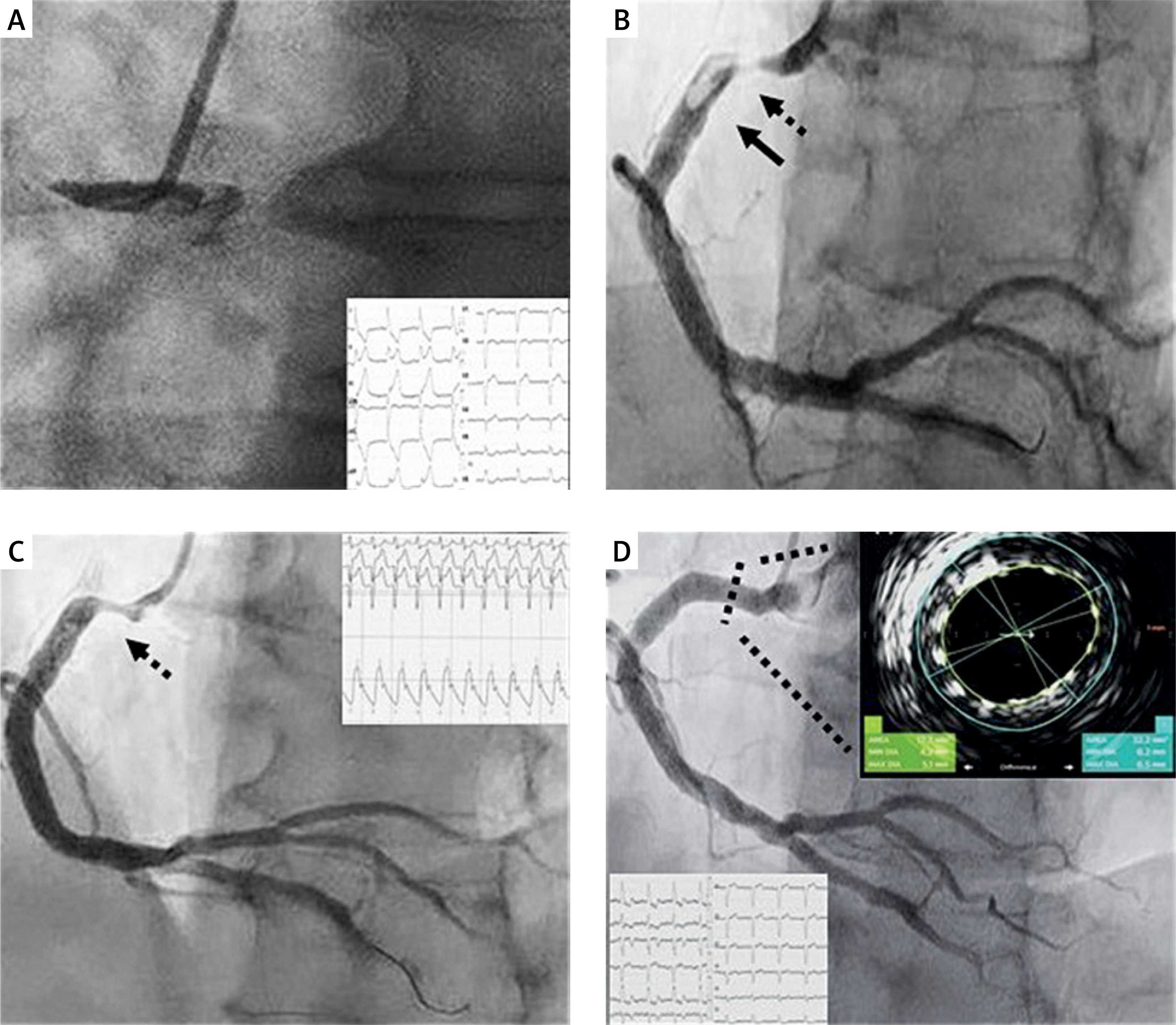
A – Baseline 12-lead electrocardiogram (ECG) showing inferior ST-elevation in leads II, III, aVF with the presence of left bundle branch block and an urgent coronary angiography an acute right coronary artery (RCA) occlusion with Thrombolysis in Myocardial Infarction (TIMI) grade 0 flow. B – Workhorse guidewire crossed the obstruction easily and positioned distally in the posterior descending artery (PDA). Severe stenosis (dotted line with arrow) with large thrombus burden (LTB) (black arrow) was revealed proximally in RCA. C – 30 min after intracoronary thrombolysis there was electrocardiographic (typical accelerated idioventricular rhythm, well tolerated) and angiographic evidence of successful reperfusion with TIMI 3 flow in PDA with complete thrombus resolution, and evidence of severe proximal RCA stenosis (dotted line with arrow). D – An excellent angiographical result was obtained following implantation of a Resolute Onyx 5.0 × 18 mm drug-eluting stent post-dilated with a non-compliant 6.0 × 8 mm balloon, based on cross-sectional intravascular ultrasound imaging with the Eagle Eye Platinum ST catheter (Volcano). Post-PCI 12-lead ECG showing inferior non-Q myocardial infarction evolution
Primary percutaneous coronary intervention (PPCI) is the preferred method of treatment of STEMI when the therapy can be delivered in a timely fashion [2]. LTB during PPCI is associated with a worse final TIMI flow grade, myocardial blush, as well as NR or DE and increased mortality [3]. In patients with LTB, routine thrombus aspiration did not improve outcomes at 1 year and was associated with an increased rate of stroke [4]. New therapies are needed to improve the outcomes of these high-risk patients. There is growing interest in the potential efficacy of adjunctive ICT during PPCI [5], and the results of the STRIVE trial (NCT03335839) are pending, investigating the safety and efficacy of reduced doses of alteplase in LTB STEMI patients undergoing PPCI. Antithrombotic drugs, deferred stenting, and active thrombectomy devices are alternative approaches for such patients [6, 7].







