
Introduction
The expression of immunohistochemical biomarkers such as estrogen receptor status (ER), progesterone receptor status (PgR), human epidermal growth factor receptor 2 (HER 2) and proliferative index Ki-67 determines the molecular subtype of breast cancer (BC). The molecular subtype has prognostic significance and influences the choice of therapy. Currently, in addition to the HER2-positive and HER2-negative subtypes, a group of patients with low HER2 expression (HER2-low) has been distinguished. This includes HER2 1+ or HER2 2+ expression on immunohistochemistry (IHC) with a negative fluorescence in situ hybridization result [1]. Traditionally, BC have been divided according to ER status into ER-positive tumours, which present with a better prognosis and ER-negative tumours. The updated American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP) guidelines recommend classifying ER status into three groups based on IHC results: ER-negative (< 1% of tumour cells), ER-low (1–10% of tumour cells), and ER-high (> 10% of tumour cells) [2]. In the literature, approximately 2–3% of BC have been described as ER-low positive [3–6].
Some studies have reported that ER-low patients display more aggressive clinical behaviour and worse survival outcomes than ER-high patients [7]. Estrogen receptor low status in BC has been associated with younger age, advanced pT, pN stage, HER2-positivity, grade III disease, high proliferation [4–6], or PR-negativity [7–9]. Estrogen receptor low positive BC were frequently classified as the luminal B (HER2+) subtype [10] and occurred in carriers of BRCA1/2 pathogenic/likely pathogenic (P/LP) variants [11, 12]. It has also been suggested that ER-low BC patients are more similar to the ER-negative group [4, 7, 10] and carry a less favourable prognosis than ER-high patients [7, 13].
In this study, we aimed to investigate the prognostic significance of ER-low status in BC patients. Additionally, we compared the ER-low subgroup with ER-negative and ER-high BC according to clinical, histopathological and molecular factors.
Material and methods
This retrospective study included 657 female patients diagnosed and treated for BC at the Maria Sklodowska-Curie National Research Institute of Oncology (Gliwice Branch) between 2002 and 2018. Inclusion criteria were: BC confirmed by microscopic examination and without distant metastases, genetic diagnosis, performance status ZUBROD 0–1, age above 18, the correct value of renal, liver function and normal values of bone marrow.
Genetic diagnostics were conducted in all 657 patients who gave written informed consent for genetic examination. All patients were tested for the presence of BRCA1 pathogenic variants (c.68_69delAG, c.181T>G, c.4034delA, c.5266dupC, c.3700_3704del5) which are most common in the Polish population. Additionally, the pathogenic variants of PALB2 (c.509_510 delGA; c.172_175 delTTGT) and CHEK2 (1100delC; IVS+1G>A; del5395; I157T) genes were also examined in BC patients. In some patients we evaluated the presence of pathogenic/likely pathogenic variants of BRCA1, BRCA2, PALB2 and CHEK2 genes using next generation sequencing technique (age at diagnosis < 45 years; triple- negative breast cancer (TNBC) of BC; family history of breast or ovarian cancer; synchronous or metachronous breast or ovarian cancer). Demographic data (age, menopausal status and family history) and tumour features (histology, ER, PgR, HER2 status including both IHC and in situ hybridization (ISH) results, Ki-67, and disease stage according to the TNM staging system: T-tumour size; N-nodal involvement; and M-metastasis) were retrieved from hospital medical files and pathology reports. The analysis of patient records was conducted in compliance with national legal regulations. Patients continue to undergo regular follow-up at the cancer research centre. A complete overview of patients’ demographic and clinicopathological features is presented in Table 1.
Estrogen receptor status was assessed by IHC in postoperative specimens or core needle biopsy samples. Estrogen receptor status was classified into three groups: ER-negative, ER-low positive or ER-high, according to the ASCO/CAP updated guidelines [2]. Tumour samples with > 1% of positive tumour nuclei for ER or PgR were classified as ER/PgR positive. Hormone receptor positivity was defined as the presence of ER and/or PgR positivity [2]. Human epidermal growth factor receptor 2 expression was evaluated using IHC and ISH based on the latest ASCO/CAP guidelines available at the time of surgery [14]. In summary, HER2-low was defined as IHC 1+ (HER2-low1+) and IHC 2+ with negative ISH (HER2-low2+/ISH(–). Human epidermal growth factor receptor 2 zero was defined as IHC 0, while IHC 3+ or 2+/ISH+ correspond to HER2-positive status. Statistical analysis was performed using Statistica 13.1 (TIBCO Software Inc.). Categorical variables were presented as frequencies and percentages. Fisher’s exact tests were used to compare patient subgroups. Statistical significance was defined as p < 0.05. Survival curves were generated using the Kaplan-Meier method, with comparisons between groups performed using the log-rank test. The Cox proportional hazards model was applied for both univariate and multivariate analysis to assess the impact of selected variables on overall survival (OS). Variables with p < 0.200 were included in the multivariate analysis. Completeness of follow-up was calculated using Clark’s Completeness Index C.
Table 1
Patient characteristics according to clinicopathological factors
Results
Patient characteristics according to clinicopathological factors
Of the 657 tumours, 93 (14.2%) were classified as ER-low, 344 (52.4%) as ER-high and 220 (33.5%) as ER-negative. Family history of cancer was observed significantly less often in the ER-low subgroup compared with ER-negative (26.9% vs. 47.7%, p = 0.001) and ER-high patients (26.9% vs. 45.6%, p = 0.001). No differences were found in menopausal status between ER-low and ER-negative (44.1% vs. 45.5%, p = 0.901) or ER-low and ER-high patients (44.1% vs. 52.3%, p = 0.163). Breast cancer patients with ER-low tumours were more likely to have larger tumour size (T3–T4) compared with ER-high (19.4% vs. 12.2%, p = 0.089) and less frequent compared with ER-negative patients (19.4% vs. 28.6%, p = 0.092). No significant differences were observed in lymph node metastases (N+) between ER-low and ER-high (41.9% vs. 42.7%, p = 0.907) or ER-low and ER-negative groups (41.9% vs. 37.7%, p = 0.527). High histological tumour grade (G3) was reported significantly less frequently in patients with ER-low compared with ER-negative tumours (21.5% vs. 48.6%, p < 0.001), with a nonsignificant trend toward fewer G3 tumours compared with ER-high (21.5% vs. 27.0%, p = 0.350). Similarly, ER-low patients were more likely to be PgR negative compared with ER-high (19.4% vs. 11.0%, p = 0.053) and less likely compared with ER-negative (19.4% vs. 92.3%, p < 0.001).
Human epidermal growth factor receptor 2 low and HER2-positive status was observed more frequently in ER-low compared with ER-negative patients (28.0% vs. 15.9% and 40.9% vs. 38.2%). No differences were found between patients with ER-low and ER-high groups in histologic cancer type (p = 0.853). On the contrary, lobular and ductal types were observed non-significantly more often in ER-low than ER-negative tumours (p = 0.097).
BRCA pathogenic/likely-pathogenic variants were reported significantly less frequently in ER-low compared with ER-negative patients (5.4% vs. 19.5%, p = 0.001). In contrary, no differences were observed between ER-low and ER-high groups (p = 0.779). Similarly, no differences in CHEK2 P/LP variants were detected between ER-low and ER-high (p = 0.267) or ER-low and ER-negative groups (p = 0.765). Estrogen receptor low status was associated with luminal B BC subtype.
Overall survival outcomes
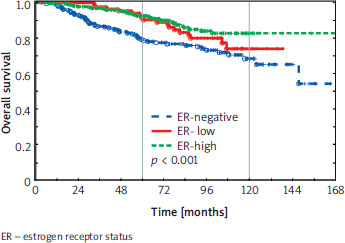
Overall survival was statistically significantly different among ER-negative, ER-low and ER-high groups (p < 0.001). Overall survival was significantly better in ER-high compared with ER-negative patients (p < 0.001). ER-low patients had OS outcomes between ER-high and ER-negative groups. Five- and seven-year OS were 93% and 86% in ER-high, 92% and 83% in ER-low, and 79% and 77% in ER-negative groups, respectively (Figure 1).
Multivariate analysis showed significantly worse survival in ER-negative compared with ER-high patients (hazard ratio – HR = 3.74, 95% CI: 1.89–7.40). In addition, no significant difference was observed for ER-low compared with ER-high patients (HR = 1.45, 0.81–2.60) (Table 2). Other factors associated with increased HR for death included age > 60 years, larger tumour size (T3–T4), nodal involvement (N+), and PgR positivity.
Table 2
Univariate and multivariate analyses of clinicopathologic factors affecting overall survival
The follow-up median (reverse Kaplan-Meier method) was 79 months. Clark’s Completeness Index was C = 89.9% for 5-year follow-up, and 65.9% for 10-year follow-up.
Discussion
In this study, we evaluated the clinical, histological, and survival features of ER-low BC compared with ER-negative and ER-high tumours in a cohort of 657 patients. Among them, 93 (14.2%) were ER-low, 344 (52.4%) ER-high and 220 (33.5%) ER-negative patients. In prior studies, ER-low tumours accounted for 2–5% of patients [4, 13].
According to the literature, ER-low tumours were associated with younger age, larger size, lymph nodal metastases, higher grade, more advanced stage, higher Ki-67, HER2 overexpression vs. patients with ER-high tumours [3, 5–7, 13]. Consistent with earlier findings [3, 7–9], our study confirmed younger age, larger tumour size, high proliferation and PgR-negativity in the ER-low subgroup. Skjervold et al. [10] reported the highest proportion of ER-low tumours in luminal B subtype (HER2+) and grade 3 subtypes. In our study, ER-low tumours were significantly associated with luminal B subtype (p < 0.001) vs. ER-high and ER-negative groups. A higher histological tumour grade was reported significantly less frequently in ER-low than ER-negative tumours.
Sanford et al. [12] indicated that ER-low tumours are more common in BRCA1/2 P/LP carriers and recommended genetic counselling. In our study, the presence of BRCA P/LP variants was reported significantly less frequently in patients with ER-low tumours compared with those with ER-negative status. No differences were observed between ER-low and ER-high subgroups regarding BRCA variants. Similarly, no differences in CHEK2 pathogenic/likely pathogenic variants were found between ER-low and ER-high or ER-low and ER-negative patients.
The risk of death from BC was lower in ER-low positive and ER ≥ 10% compared with ER-negative cases [10]. Estrogen receptor low patients seemed to have more aggressive clinical behaviour and worse survival outcomes than ER-high patients, and appeared to benefit less from endocrine therapy [4, 7]. Several studies have assessed the prognosis of patients with early-stage ER-low BC [10, 15–17]. The human epidermal growth factor receptor 2 negative/ER-low positive subgroup has been suggested to resemble TNBC [15, 16]. Other studies reported no significant survival differences between ER-low and ER-negative tumours [3, 9, 17, 18]. The benefit of endocrine therapy in patients with ER-low status remains uncertain [4]. However, ER-low tumours show sensitivity to chemotherapy and promising responses to neoadjuvant chemo-immunotherapy, as in triple-negative BC patients [19, 20]. Neoadjuvant olaparib plus durvalumab in the BRCAness subgroup of ER-low BC is under evaluation in the trial [21]. The role of CDK4/6 inhibitors in ER-low BC has not yet been established [13].
In our study, 5-year OS was similar in both groups: ER-high and ER-low (93% vs. 92%). Overall survival was non-significantly better in ER-low compared with ER-negative patients (p = 0.107; 5-year OS: 92% vs. 79%, 7-year OS: 83% vs. 77%).
There are several limitations of our study. First, the relatively small number of patients in some subgroups may weaken statistical power. Second, it was a single-centre and retrospective analysis, which limits generalizability. The strengths of this study include long follow-up time for survival events (7–13 years), relatively complete data, and consideration of genetic factors. This is a preliminary study. Therefore, results indicate a tendency that requires confirmation in a larger group of patients.
Conclusions
Significant differences were reported between ER-negative, ER-low, and ER-high subgroups in the T stage (p < 0.001), grade (p < 0.001), PgR (p < 0.001), BRCA status (p < 0.001), and family history of cancer (p = 0.002). Estrogen receptor low status was associated with larger tumour size (T3–T4) and PgR negativity compared with ER-high tumours, and with lower grade (G1–G2) and fewer BRCA P/LP variants compared with ER-negative tumours. Moreover, ER-low status was associated with improved 5- and 7-year OS compared with ER-negative tumours.








