
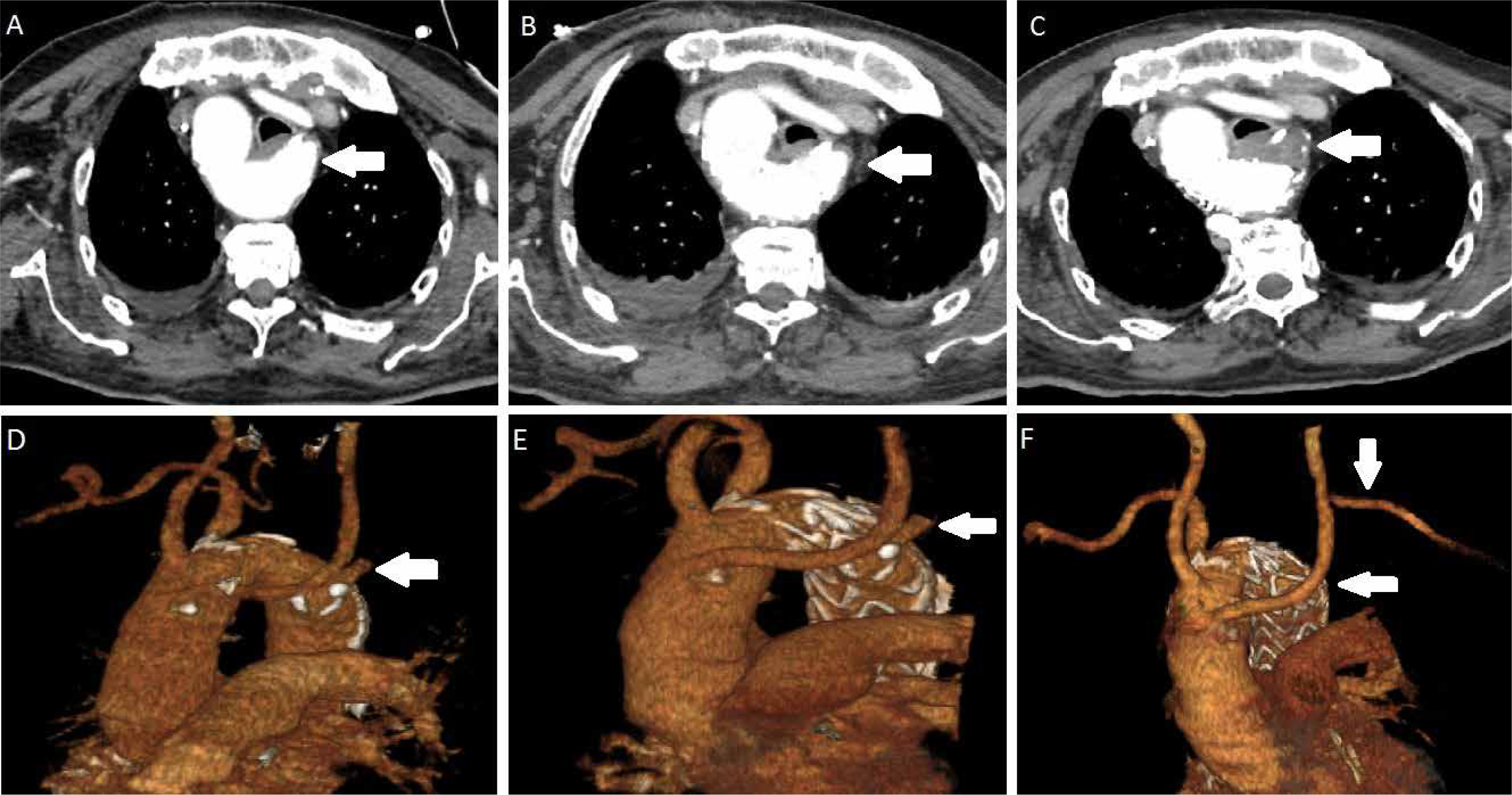
Right-sided aortic arch accompanying aberrant left subclavian artery is mostly asymptomatic and incidentally detected. Guidelines or surgical indications for Kommerell’s diverticulum have not been established because of the rareness of the anomaly. Ota et al. [1] recommend treating patients with the diameter of Kommerell’s diverticulum more than 50 mm in patients who had symptoms associated with Kommerell’s diverticulum. Czerny et al. [2] stated that aberrant subclavian arteries ≥ 3 cm in diameter and Kommerell’s diverticula with a diameter ≥ 5.5 and in addition symptomatic patients should be treated. Symptoms including dysphagia, respiratory failure, or chest pain can be present in 5% of patients. Treatments options include open surgery via sternotomy or thoracotomy under deep hypothermic circulatory and endovascular and hybrid surgery [3]. An 84-year-old man who presented with pneumonia due to compression of the trachea was admitted to our hospital. Computed tomography revealed right-sided aortic arch and the left subclavian artery arose from the descending aorta in a Kommerell’s diverticulum. The right-sided descending aorta had a maximum diameter of 45 mm and the diverticulum had a 25 mm diameter. He was intubated in the emergency service due to severe dyspnea and appropriate antibiotic therapy was administered. After informed consent had been taken from the patient’s family, a tracheostomy was performed 2 weeks after intubation. Due to compression symptoms of Kommerell’s diverticulum, the first stage was performed via a subclavian artery to carotid artery transposition and the second stage was performed via thoracic endovascular repair (TEVAR) with 40 × 40 × 150 mm Valiant Captivia (Medtronic, Santa Rosa, Calif) endograft. Postoperative computed tomography showed complete exclusion of the diverticulum and no endoleaks (Figures 1 A–F). He was removed from the ventilator 2 weeks later and discharged at 1 month postoperatively. Six months later he was doing well without dyspnea and endoleak. Here, we report a case of successful hybrid treatment and resolution of a Kommerell’s diverticulum.
Full text
1/2023
vol. 20
Letter to the Editor
Hybrid treatment of type 2 right sided aortic arch and Kommerell’s diverticulum in an octogenarian
- Department of Cardiovascular Surgery, Institute of Cardiology, Istanbul University-Cerrahpasa, Instanbul, Turkey
Kardiochirurgia i Torakochirurgia Polska 2023; 20 (1): 60-61
Data publikacji online: 2023/04/03
Article file
References
Czerny M, Schmidli J, Adler S, van den Berg JC, Bertoglio L, Carrel T, Chiesa R, Clough RE, Eberle B, Etz C, Grabenwöger M, Haulon S, Jakob H, Kari FA, Mestres CA, Pacini D, Resch T, Rylski B, Schoenhoff F, Shrestha M, von Tengg-Kobligk H, Tsagakis K, Wyss TR; EACTS/ESVS scientific document group. Current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic surgery (EACTS) and the European Society for Vascular Surgery (ESVS). Eur J Cardiothorac Surg 2019; 55: 133-162.
Copyright: © 2023 Polish Society of Cardiothoracic Surgeons (Polskie Towarzystwo KardioTorakochirurgów) and the editors of the Polish Journal of Cardio-Thoracic Surgery (Kardiochirurgia i Torakochirurgia Polska). This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0) License (http://creativecommons.org/licenses/by-nc-sa/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, provided the original work is properly cited and states its license.









