
Introduction
Marginal zone lymphomas (MZL) are indolent non-Hodgkin lymphomas (NHL), which develop from B lymphocytes present in secondary lymphoid organs. They are the second most popular kind of NHL, constituting 7% of all cases [1, 2]. Marginal zone lymphomas can be divided into three subtypes: nodal, splenic and extranodal mucosa-associated lymphoid tissue lymphoma. The third type is the most common (60.8% of cases) [3]. The most frequent sites of its location are: stomach (30%), adnexa, salivary gland, lung, skin, thyroid and breast [1]. Therefore, presence of MZL in arytenoid cartilage, which is reported below, is a very infrequent event.
Case report
On 21 September 2020, a 61-year-old male was admitted to the otolaryngological ward due to hoarseness, which had been present for four years. During the first visit to a specialist in 2016, Reinke’s oedema was observed. The patient underwent decortication of the right vocal fold and laryngeal ventricle, but there were not any tissue abnormalities. Therefore, sections of the vestibular fold were taken in 2016, 2017 and 2018. Biopsies did not reveal any neoplastic lesions. During a follow-up in May 2019, a biopsy of a deep section of the larynx including mucous membrane, adipose tissue and muscle tissue was done due to suspicion of the right vocal fold neoplasm. The procedure was repeated two months later, but in both cases no neoplastic lesion was present. Therefore, in November 2019 the patient underwent a microlaryngoscopy. The section of mucosa covered with stratified squamous epithelium revealed no characteristics of atypia. However, chronic inflammatory infiltration was present in mucous membrane stroma. As a result, magnetic resonance imaging (MRI) scan was used in April 2020 to analyse the larynx and trachea of the patient. A hyperplastic tuberous change was present in the right area posterior to the glottis, presenting characteristics of restricted diffusion (Figure 1 A, B). Therefore, the patient underwent a second microlaryngoscopy in June 2020. The analysis with use of immunohistochemistry rejected neoplastic lesions in the acquired section. Indirect laryngoscopy in September 2020 exposed a smooth tumour, which caused bulging of the right vestibular fold. Therefore, the patient underwent microlaryngoscopy during which a fragment of the right arytenoid cartilage was excised with the use of a laser. The patient left the ward two days after the procedure. The section analysed during histopathological examination consisted of mucosa covered with stratified squamous epithelium, present on lymphoid stroma. It was mostly infiltrated with small and medium-sized lymphoid cells. Their immunophenotype review confirmed indolent B-cell lymphoma, specifically extranodal marginal zone lymphoma (EMZL) (Figure 2 A–I). After the patient was diagnosed, he underwent bendamustine and rituximab (BR) chemoimmunotherapy, which ended in September 2021. The patient has remained in remission and attends annual follow-ups in the laryngological and haematological ward.
Figure 1
Magnetic resonance imaging scan presenting the larynx and trachea with hyperplastic tuberous change in the right area posterior to the glottis, presenting characteristics of restricted diffusion. A) Transverse section of the tuberous change. B) Coronal section of the tuberous change
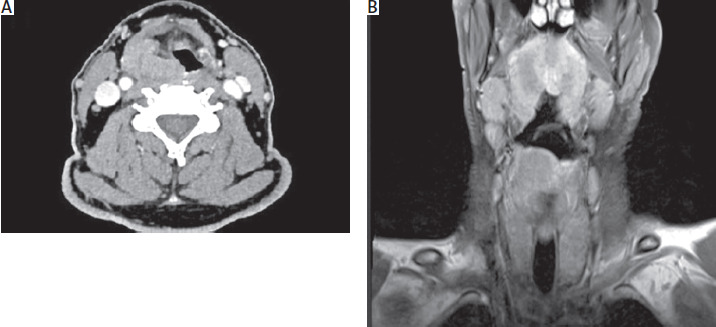
Figure 2
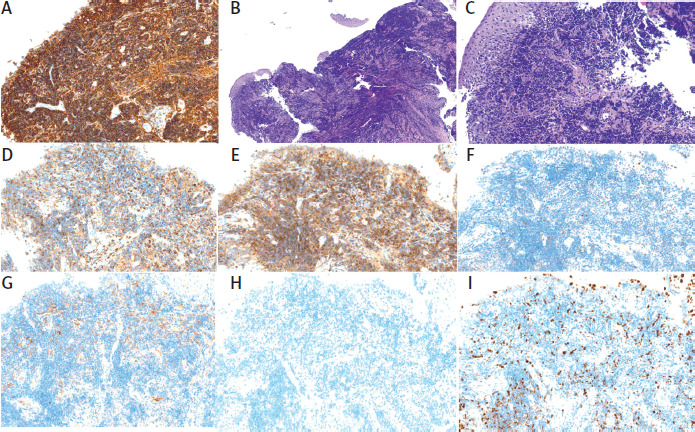
Immunohistochemistry staining in the arytenoid cartilage affected by extranodal marginal zone lymphoma. A) CD20 staining (B-cell marker). B) Hematoxylin and eosin staining, presenting lymphoid cells (4× magnification). C) Hematoxylin and eosin staining (20× magnification). D) CD3 staining. E) BCL2 staining. F) BCL6 staining. G) CD10 staining. H) CD23 staining. I) Ki-67 staining
Discussion
Extranodal marginal zone lymphoma appears in tissues as a result of chronic inflammation, usually caused by specific pathogens (Helicobacter pylori in gastric EMZL, Chlamydia psittaci in ocular adnexal EMZL) or autoimmune diseases (Sjögren syndrome in salivary gland EMZL, Hashimoto thyroiditis in thyroid EMZL) [1, 3]. The abnormalities are also commonly located in the skin, lungs and breast [1, 2]. Location of EMZL in arytenoid cartilage is extremely uncommon, as less than 1% of laryngeal tumours are NHLs. They are most usually located in the supraglottic region [4]. Extranodal marginal zone lymphoma has the highest 5-year relative survival rate (94%) of all MZL subtypes [2]. Median survivals in this disease are over 10 years [5].
Diagnosis of MZL demands the use of imaging techniques, for instance positron emission tomography/computed tomography (PET/CT) or MRI. In case of the patient, MRI was used because PET/CT is not always recommended in MZLs (Lugano Classification does not recommend it, in contrary to the National Comprehensive Cancer Network, in case of specific patients) [3]. As extranodal sites present various fluorodeoxyglucose-avidity, use of PET/CT could lower reliability of the examination [3]. Results of MRI scan and detection of smooth tumour during laryngoscopy were the reasons for performing microlaryngoscopy. This procedure is necessary to obtain a tissue section for immunopathological examination. Microlaryngoscopy with the use of CO2 laser was chosen due to its multiple assets, such as precision, relatively small scar and swelling of the affected tissues, satisfactory haemostasis and decreased postoperative pain [6].
Histopathological examination was used to analyse the immunophenotype of the neoplastic cells. Expression of CD20, CD43, and absence of CD10, CD23, bcl6 and cyclin D1 revealed similarity of the examined cells to normal marginal zone B-cells [3, 7]. Therefore, EMZL diagnosis was confirmed. Ki-67 antigen was also detected to analyse the percentage of tumour cells which undergo proliferation G1–M phase of the cell cycle [8].
Chemoimmunotherapy was the applied treatment method because it is considered the most appropriate for the advanced-stage extranodal MZL [1, 2]. Therapies including BR, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) or rituximab, cyclophosphamide, vincristine, and prednisone (R-CVP) are standards of care. According to randomized clinical trials (StiL and BRIGHT) concerning patients with indolent NHL and mantle cell lymphoma, the above treatments result in a similar rate of progression-free survival. However, adverse events are more frequent in R-CHOP and R-CVP than in BR [2, 3]. The patient was treated with BR to lower the risk of high-grade cytopenia and infections following chemoimmunotherapy [2].
Conclusions
Extranodal marginal zone lymphoma is an indolent NHL, rarely present in arytenoid cartilage. In the above case, MRI and microlaryngoscopy were crucial diagnostic methods, which enabled locating and excising the tumorous lesion. Histopathological examination and immunophenotyping were used to establish the diagnosis by differentiating between MZL and other lymphomas. Chemoimmunotherapy in EMZL prevented progression of the condition and side effects of the therapy. All the above methods applied one by one lead to remission of MZL.






