
Mechanical thrombectomy (MT) has emerged as an adjunctive treatment for high-thrombus-burden lesions, particularly in cases involving highly resistant thrombi [1]. An invasive treatment of such lesions might be a therapeutic challenge for cardiologists, due to the need to achieve a hemodynamically optimal result while avoiding serious complications, such as stroke, no-reflow syndrome, or coronary artery dissection. Aspiration systems such as the Penumbra device show growing potential when they are applied in coronary artery treatment, particularly in complex cases where thrombus removal is critical for achieving optimal reperfusion, especially after failed manual aspiration [2].
A 53-year-old male patient with multimorbidity – hypertension, hyperlipidemia, type 2 diabetes, multivessel coronary disease – and a history of multiple percutaneous coronary interventions (PCIs), presenting with non-ST-elevation myocardial infarction, was admitted to the cardiology department. Coronary angiography showed total occlusion of the proximal right coronary artery (RCA) (Figure 1 A), with developed collateral circulation. Echocardiography on admission showed slightly decreased left ventricular ejection fraction (LVEF) of 45–50%.
Figure 1
A – Angiographic image of the right coronary artery (RCA) before the first stage of percutaneous coronary intervention (PCI). B – Angiographic image of the RCA after the primary PCI; large aneurysm visible (arrow). C – Intravascular ultrasound (IVUS) during the second stage of PCI. D – Angiographic image of the RCA after the mechanical thrombectomy (MT)
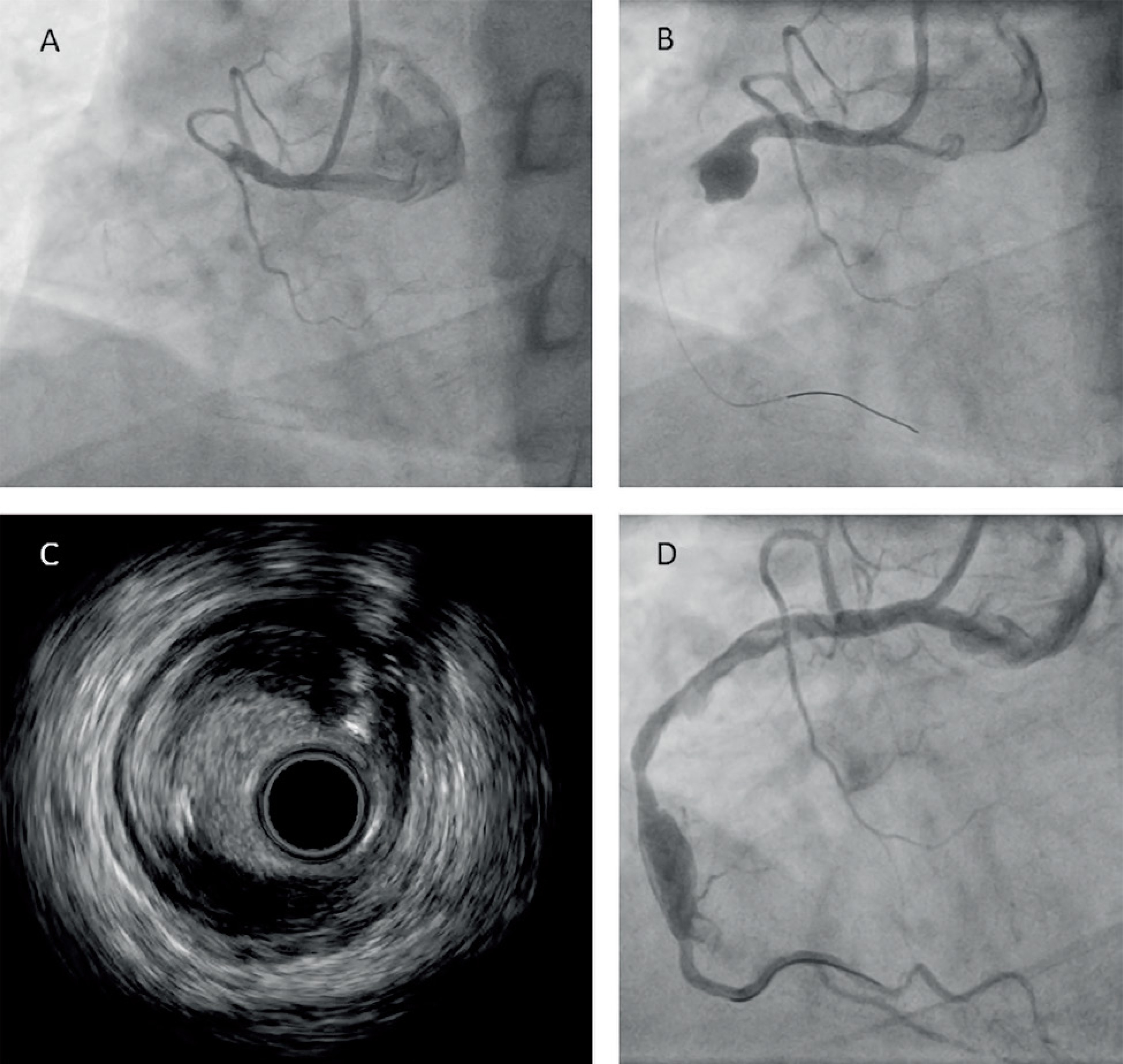
Primary PCI of the RCA with subsequent 7F manual thrombectomy (iVascular, Spain) was performed. The aspirate contained multiple fragments of thrombus. Control coronary angiography revealed a large aneurysm with a 12 mm diameter and a massive thrombus in its distal part, occluding the middle and distal segments of the RCA (Figure 1 B). Due to the clinical image and very low probability of restoring vessel patency, the patient was managed conservatively with dual antiplatelet therapy (including ticagrelor) and anticoagulation with low molecular weight heparin.
Seven days later, follow-up angiography, performed due to exertional angina, revealed total occlusion of the RCA, and another PCI, this time with an MT IndigoCath RX 6F system (Penumbra, USA), was performed under intravascular ultrasound (IVUS) guidance (Figure 1 C). Multiple passages of thrombectomy were performed with removal of abundant debris, restoring a TIMI 3 flow (Figure 1 D). Next, several balloon inflations (2.5 × 20 mm to 20 atm, 3.0 × 15 mm to 16 atm), including prolonged inflation of a drug-eluting balloon (DEB) 3.5 × 30 mm, were performed. The posterior descending branch of the RCA remained occluded, as it turned out to be a chronic total occlusion. The patient was started on further conservative treatment and discharged home in a good overall condition.
Data regarding the use of MT aspiration systems, such as the IndigoCath RX 6F, in acute coronary syndromes are relatively scarce. However, based on the available data, they appear to reduce the prevalence of post-procedural no-reflow syndrome, particularly when used as part of double protection [3]. Moreover, use of mechanical systems may result in clinically meaningful benefits, at least non-inferior to manual thrombus aspiration technique [4]. Therefore, the use of aspiration systems might become a part of a novel approach to treatment of high-thrombus-burden lesions, especially in cases involving very large thrombi or patients at high risk of no-reflow.







