
Summary
The study suggests that while global left ventricular longitudinal strain and other myocardial work parameters do not exhibit substantial variation with mitral regurgitation (MR) severity, global constructive work could be a more sensitive measure of changes in cardiac function due to MR. These findings underscore the potential clinical value of myocardial work assessment in patients with aortic stenosis and concomitant MR, particularly in evaluating myocardial efficiency and function after transcatheter aortic valve implantation.
Introduction
Non-invasive assessment of myocardial work based on global left ventricular longitudinal strain (GLS) is gaining increasing recognition as a valuable tool for evaluating left ventricular function independent of loading conditions. The clinical utility of myocardial work assessment has been validated across various cardiac pathologies, including aortic stenosis, primary and secondary mitral regurgitation (MR), and other cardiovascular diseases [1].
Pederson et al. described in detail changes in GLS and myocardial work parameters in patients with different types of aortic stenosis, highlighting their prognostic value [2]. It has been demonstrated that in patients with high-gradient aortic stenosis (AS) and preserved left ventricle ejection fraction (LVEF ≥ 50%), a decrease in LVEF is observed after transcatheter aortic valve implantation (TAVI), accompanied by an improvement in GLS and a significant reduction in global work index (GWI). In patients with high-gradient aortic stenosis and LVEF < 50%, the procedure results in a significant increase in LVEF and GLS, with only a minimal rise in GWI. Conversely, in patients with low-gradient aortic stenosis, where LVEF is initially ≥ 50%, a post-procedural decline in LVEF and GWI is observed, while GLS remains unchanged. However, in cases where LVEF is initially < 50%, an increase in LVEF, GLS, and GWI is noted following the procedure.
The observed changes in LVEF, GLS, and GWI in aortic stenosis are closely linked to left ventricular hypertrophy, volume reduction, and, in advanced stages of the disease, myocardial fibrosis. Despite the increasing pressure load, compensatory mechanisms often help preserve normal LVEF. However, a decline in LVEF is typically indicative of irreversible myocardial damage [3]. Although LVEF often remains preserved in severe aortic stenosis, GLS is significantly impaired, potentially indicating an early stage of left ventricular systolic dysfunction. However, a reduction in GLS may result from both myocardial fibrosis and increased pressure overload. MW parameters provide a more precise assessment of left ventricular function, independent of afterload.
Concomitant MR is an unfavorable prognostic factor in patients with AS [4–7]. In the progression of AS, volume overload serves as an additional factor impacting left ventricular function. It is estimated that moderate to severe MR affects approximately 15% of patients with severe AS [8]. Previous studies have not analyzed changes in GLS and myocardial performance in the context of concomitant MR in aortic stenosis.
Aims
This study aimed to evaluate the effects of concomitant MR on myocardial work parameters in patients with severe AS undergoing TAVI.
Material and methods
This prospective observational registry included 95 consecutive patients with AS who were hospitalized between November 2023 and September 2024 and met the clinical and imaging criteria for TAVI. The sample size was not formally calculated, as all eligible patients during the study period were enrolled. Patients with insufficient echogenicity for reliable strain and myocardial work assessment were excluded. Demographic and clinical data were collected for each patient, and all underwent transthoracic echocardiography (TTE). According to national regulations and institutional policies, observational studies based exclusively on standard diagnostic procedures do not require approval from a bioethics committee; therefore, formal ethical approval was not sought. In view of its non-interventional nature, the study was not registered in ClinicalTrials.gov or other trial registries.
TTE was performed on a GE VIVID E95 (General Electric Healthcare, Horten Norway) with a transducer with a frequency range of 1.5–4.5 MHz, with simultaneous ECG recording. In patients with sinus rhythm, images were recorded and archived during a single cardiac cycle, while in patients with atrial fibrillation, recordings from six cardiac cycles were archived. Projections were obtained according to the American Society of Echocardiography (ASE) and the European Association of Cardiovascular Imaging (EACVI) recommendations [9].
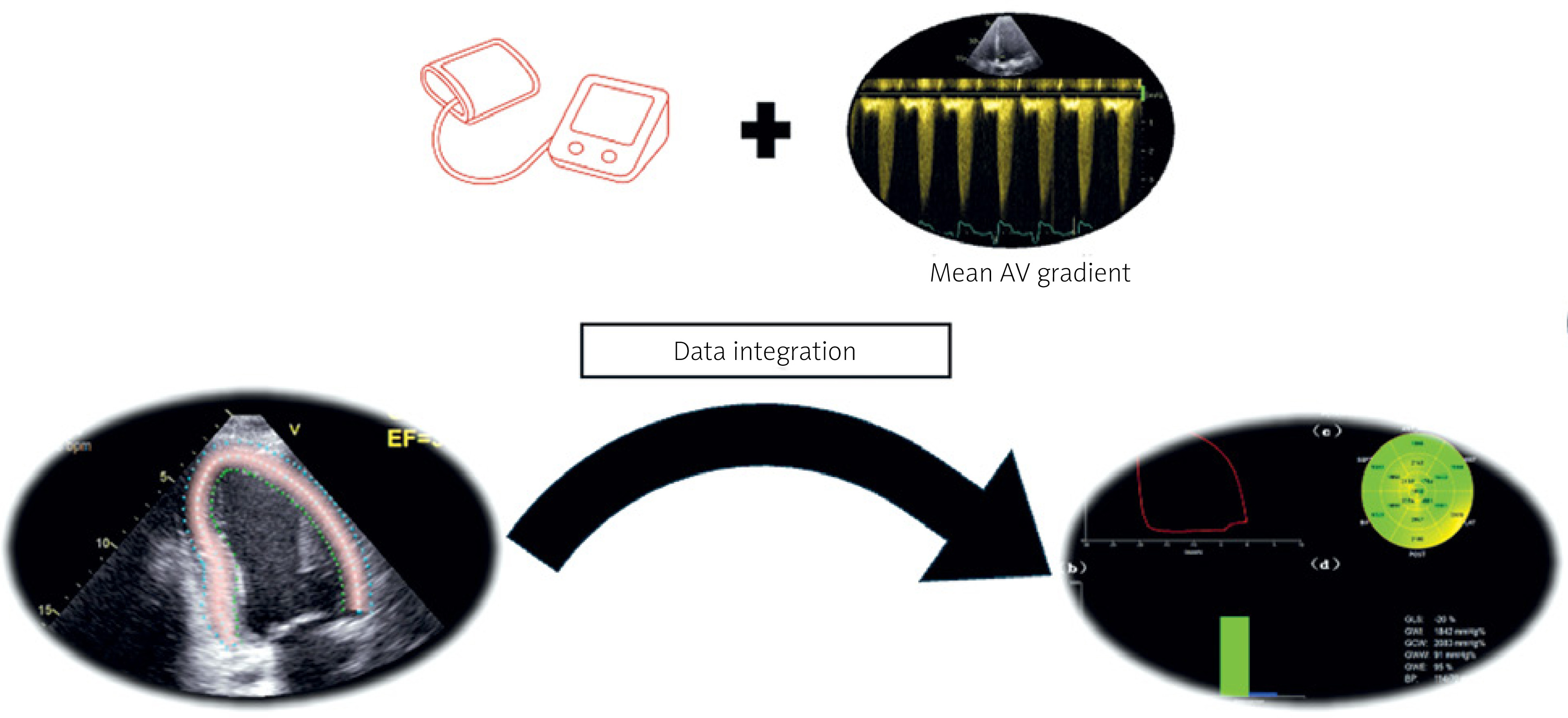
Brachial blood pressure was measured non-invasively immediately before echocardiographic image acquisition, with the patient in the supine position and after at least 5 min of rest. Measurements were performed using an appropriately sized cuff placed on the right arm, in accordance with current guidelines. Systolic and diastolic blood pressure values were obtained using an automated oscillometric device. For myocardial work analysis, systolic blood pressure entered into the EchoPac software was calculated as the sum of the measured brachial systolic pressure and the mean transvalvular gradient across the aortic valve (Figure 1), in accordance with the methodology for estimating left ventricular systolic pressure proposed by Ilardi et al. [10] Echocardiographic parameter analysis was conducted offline using an EchoPac workstation (EchoPac 205, General Electric Vingmed Ultrasound, Horten, Norway). The severity of aortic stenosis was assessed using a multiparametric approach, incorporating measurements of maximum aortic valve flow velocity, mean transvalvular pressure gradient, and aortic valve area (AVA), which was calculated based on the continuity equation. Severe low-gradient aortic stenosis was defined by an AVA of ≤ 1 cm2 in conjunction with a reduced mean transvalvular pressure gradient, provided that the stroke volume index (SVI) relative to body surface area was less than 34 ml/m2.
Figure 1
Methodology for obtaining myocardial work parameters based on the integration of longitudinal strain (GLS) and arterial pressure measurement in patients with aortic stenosis
The severity of MR was evaluated using a comprehensive, multiparametric approach, integrating several echocardiographic parameters. These included the extent of the regurgitant jet, the vena contracta diameter, the effective regurgitant orifice area calculated using the proximal isovelocity surface area method, and the regurgitant volume. Based on these measurements, MR was classified into four grades: (0) no or trace regurgitation, (1) mild regurgitation, (2) moderate regurgitation, and (3) severe regurgitation. This systematic approach ensures an accurate assessment of MR severity, which holds significant prognostic value.
Myocardial deformation, specifically GLS, was analyzed using speckle-tracking echocardiography, employing an automated analysis algorithm based on four-chamber, two-chamber, and three-chamber apical views, with a primary focus on the left ventricle. The region of interest for GLS assessment was automatically delineated by the software and subsequently reviewed and, if necessary, manually adjusted by an experienced echocardiographer to ensure optimal accuracy. The frame rate for the recorded images used in GLS analysis was set between 80 and 100 frames per second to enhance temporal resolution and tracking precision.
Following the completion of GLS analysis on the EchoPac workstation, myocardial work parameters were assessed, including:
global constructive work (GCW) – the total myocardial work performed during the shortening of myocardial fibers in the systolic phase and their lengthening during isovolumic diastole.
global wasted work (GWW) – the myocardial work expended during fiber lengthening in systole and shortening in isovolumic diastole while the aortic valve remains closed.
global work efficiency (GWE) – the ratio of GCW to the total myocardial work, calculated as GCW divided by the sum of GCW and GWW, expressed as a percentage [11].
Statistical analysis
Statistical analysis was performed using the JAMOVI software (Version 2.3.21.0). Normality was assessed using the Shapiro-Wilk test. Quantitative variables were expressed as mean ± standard deviation, while categorical variables were presented as counts and percentages. Group comparisons based on MR severity were conducted using the Kruskal-Wallis ANOVA test for quantitative variables and the chi-square test (χ2) for categorical variables. A p-value of < 0.05 was considered statistically significant. In the case of global test significance, pairwise comparisons were performed using the Dwass-Steel-Critchlow-Fligner (DS-CF) procedure with family wise error rate control.
Results
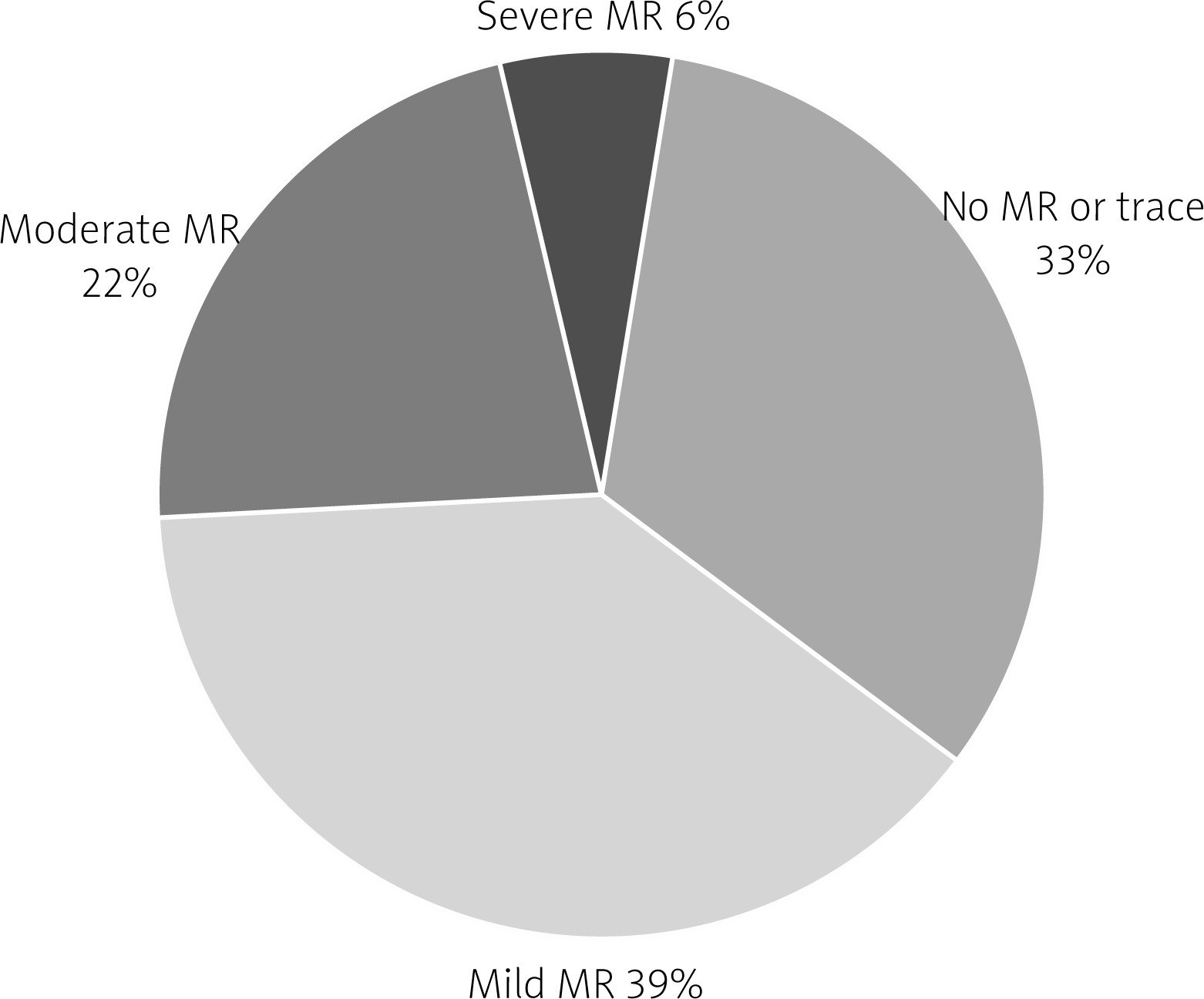
The study cohort consisted of 95 patients with a mean age of 79.1 ±5.3 years. Women accounted for 47.4% (45 patients), while men comprised 52.6% (50 patients). MR was identified in two-thirds of the study population, with moderate to severe MR present in 28% of patients (Figure 2).
According to the Carpentier classification [12], type IIIa MR was the most prevalent, observed in 39 patients (67.24%), while the remaining 19 patients (32.76%) exhibited type IIIb regurgitation. The prevalence of moderate to severe MR was comparable between the two subtypes, occurring in 19 (48.7%) cases of type IIIa and 8 (42.1%) cases of type IIIb (χ2 = 0.2245, p = 0.64). No statistically significant differences were observed in demographic characteristics or comorbidities between patients depending on the degree of MR (Table I). Although not significant, patients with severe MR were on average younger and had a lower body mass index (BMI) compared to those with mild or moderate MR.
Table I
Characteristics of the study group
Table II compares echocardiographic parameters between groups stratified by the severity of MR. No statistically significant differences were observed between the groups in parameters related to aortic stenosis, left ventricular dimensions, or left ventricular wall thickness. Similarly, left ventricular volume and LVEF did not differ significantly between the groups.
Table II
Echocardiographic findings according to the degree of mitral regurgitation
[i] LV-EDD – left ventricle end-diastolic diameter, LV-ESD – left ventricle end-systolic diameter, LV-EDV – left ventricle end-diastolic volume, LV-ESD – left ventricle end-systolic volume, LV-EF – left ventricle ejection fraction, IVS – intraventricular septum, PW – posterior wall, LA – left atrium, RV – right ventricle, RVSP – right ventricular systolic pressure, TAPSE – tricuspid annulus plane systolic excursion, AV – aortic valve.
However, significant differences were noted in left atrial size, with both left atrial diameter and left atrial area being highest in the group with severe MR. Additionally, E-wave velocity increased significantly with the severity of MR, which may indicate left ventricular volume overload or suggest alterations in left ventricular diastolic function associated with MR. No other echocardiographic parameters demonstrated significant differences between the groups.
Figure 3 presents the analysis of cardiac parameters stratified by the severity of MR. No significant differences were observed in GLS, with a mean value of –13.7 ± 3.9% across the entire cohort, and similar values across all groups (p = 0.35).
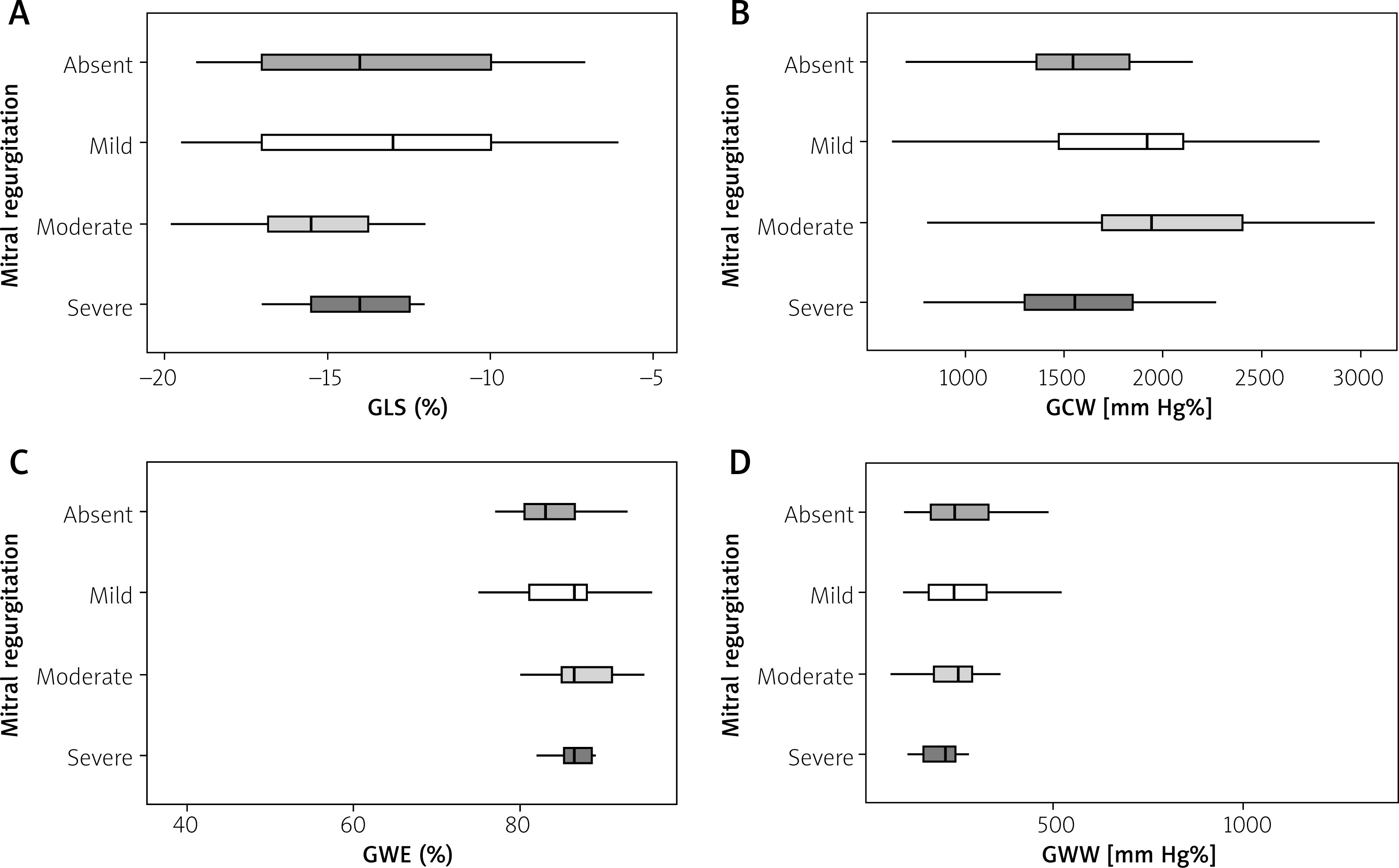
In contrast, GCW demonstrated significant differences between groups (p = 0.01). The lowest GCW value was observed in patients with severe MR (1483.3 ±282.7 mm Hg%), whereas the highest value was recorded in those with moderate MR (2114.9 ±534.6 mm Hg%). Post-hoc DS–CF testing revealed significant differences between mild and severe MR (p = 0.035) and moderate and severe MR (p = 0.010); all other pairwise comparisons were non-significant. GWW did not differ significantly between groups (p = 0.21). Consequently, significantly lower GWE values were observed in patients with severe MR compared to the other groups. For GWE, there was a significant overall between-group effect (Kruskal-Wallis: χ2(3) = 9.99, p = 0.02). However, after controlling the familywise error rate, the DS–CF pairwise comparisons did not identify any significant contrasts (all p ≥ 0.07). This pattern suggests that several minor, concordant deviations occur across specific groups, rather than a single pronounced pairwise separation. The values for individual parameters are presented in Table III.
Table III
Results of myocardial strain and myocardial work analysis in relation to the degree of mitral regurgitation
In summary, the findings indicate that while parameters such as GLS and GWW remain comparable across patient groups with varying degrees of MR, GCW and GWE may serve as a more sensitive indicator of changes in cardiac function in relation to MR severity.
Discussion
Aortic stenosis and mitral regurgitation represent a complex hemodynamic interplay that significantly alters myocardial performance. Understanding how myocardial work indices respond to these valvular pathologies is essential for early identification of myocardial dysfunction and for optimizing treatment strategies. Our study addresses this clinical gap by analyzing myocardial work components in symptomatic patients with AS, both with and without concomitant MR – a subgroup often underrepresented in previous research. These findings not only deepen insight into the pathophysiology of AS-related myocardial remodeling but also highlight the prognostic relevance of advanced echocardiographic markers in complex valve disease.
Increased afterload pressure in aortic stenosis acts as a stimulus for myocardial hypertrophy and an increase in myocardial work to preserve stroke volume. Consequently, myocardial work parameters such as GWI, GCW, and GWW tend to rise. A study by Ilardi et al. reported a significant increase in GWI, GCW, and GWW in patients with aortic stenosis compared to controls (GWI: 2528 ±521 vs. 2005 ±302 mm Hg%, GCW: 2948 ±598 vs. 2360 ±353 mm Hg%, p < 0.001; GWW: 139 ±90 vs. 90 ±49 mm Hg%, p = 0.005), while GWE remained unchanged [10]. However, this study focused on asymptomatic patients, in whom compensatory mechanisms are still active, and the myocardium has not yet shown signs of damage.
In a symptomatic patient population, such as those in our study, compensatory mechanisms are depleted, and the myocardium undergoes damage associated with fibrosis and progressive dysfunction. Consequently, GLS, GCW, and GWE values observed in our study are significantly lower, while GWW is higher than the reference values. The increase in GWW may result from the heightened myocardial load in response to the exhaustion of compensatory mechanisms, ultimately leading to reduced cardiac efficiency.
Similar findings have been reported in previous studies, indicating that patients with advanced-stage aortic stenosis, particularly those who are symptomatic, exhibit a significant reduction in GWE despite an increased myocardial workload aimed at preserving hemodynamic capacity [13]. These studies also observed that alterations in cardiac mechanics parameters, such as a decrease in GLS, may serve as valuable indicators for monitoring disease progression and prognosis. Notably, changes in indices such as GLS and GWE may be early markers of developing diastolic dysfunction [14].
In patients with aortic stenosis and concomitant MR, a reduction in afterload and stroke volume leads to a low-flow state across the aortic valve. This effect is further exacerbated by aortic stenosis-induced left ventricular hypertrophy, contributing to decreased preload. These hemodynamic alterations associated with coexisting MR may have significant prognostic implications. Several studies have demonstrated that the presence of significant MR is associated with increased in-hospital and long-term mortality following interventional treatment for aortic stenosis [4, 5, 7, 15]. This is particularly evident when MR does not improve following aortic valve intervention. This scenario is prevalent in cases of degenerative MR [16]. The poorer prognosis in patients with MR may be attributed to a higher burden of comorbidities and more extensive left ventricular damage [6].
Pastore et al., in an analysis of echocardiographic myocardial parameters in a cohort of patients with primary MR, found that GCW was significantly higher in severe compared to mild MR (2261 ±333 mm Hg% vs. 2501 ±632 mm Hg%, p < 0.01), along with an increase in GWW. Additionally, GWE was markedly reduced in patients with higher MR severity [17]. In contrast, our findings indicate that compensatory mechanisms enhancing GCW appear insufficient when severe aortic stenosis (AS) coexists with severe MR. This discrepancy may be attributed to the different etiologies of MR studied. While Pastore et al. focused on primary (degenerative) MR, most of our patients presented with secondary (functional) MR, often resulting from left ventricular remodeling and dysfunction. Consistent with Pastore’s results, however, we also observed a significant reduction in GWE in patients with severe MR, suggesting that regardless of MR etiology, global myocardial efficiency diminishes as MR severity increases – particularly when accompanied by advanced AS-related myocardial damage.
In our study, GWW was significantly elevated compared to reference values, irrespective of the presence and severity of MR. Moreover, severe MR was associated with a significant reduction in GCW and marked left atrial enlargement. Left ventricular diastolic dysfunction, often linked to myocardial fibrosis, impairs ventricular filling, ultimately leading to decreased GCW. Furthermore, chronic volume overload due to MR contributes to left atrial enlargement, which represents an adaptive response to the increased retrograde blood volume.
It is important to emphasize that a reduction in GCW and left atrial enlargement contribute to a significant decrease in left ventricular preload. In turn, diminished preload can lead to a reduction in stroke volume and impaired cardiac hemodynamic efficiency. As a result, despite a similar degree of aortic stenosis, these patients may experience more pronounced symptoms.
Furthermore, in our study, GCW remained relatively stable from no MR to mild MR, reached its highest in the moderate MR group, and decreased sharply in the severe MR group, showing an inverted U-shaped pattern. In early MR, preload augmentation and a lower effective afterload (via the regurgitant pathway) can temporarily improve myocardial performance – i.e., load-dependent metrics such as GCW – despite unchanged intrinsic contractility. As MR advances to the severe stage, particularly in the context of severe AS (elevated valvulo-arterial load), the LV encounters higher wall stress, chamber dilation, and mechanical dyssynchrony; a growing portion of the total work becomes wasted (ineffective for forward flow). Concomitant myocardial fibrosis likely reduces contractile reserve, leading to a fall in constructive work even when instantaneous loading remains high. Consistent with this mechanism, the framework anticipates lower GWE with advancing disease, reflecting rising energetic inefficiency. While a chance finding cannot be excluded – particularly given sample size and multiplicity control in pairwise testing – the shape of the association is physiologically plausible. To balance interpretation and inference, we treat GCW and related pressure–strain metrics as indicators of myocardial performance (load-dependent) rather than direct measures of intrinsic myocardial function (contractility).
These findings underscore the critical importance of monitoring myocardial parameters in patients with concomitant valvular pathologies, such as aortic stenosis and MR. A comprehensive assessment helps prevent misinterpretation of stenosis severity and provides a more accurate evaluation of myocardial damage in this patient population.
Furthermore, these observations highlight the necessity of early diagnosis and continuous monitoring in patients with coexisting valvular defects to optimize therapeutic strategies and improve clinical outcomes.
This study has several limitations that should be acknowledged. First, it was conducted as a single-center, prospective registry study with a relatively small sample size, which may limit the statistical power of the analyses and the generalizability of the findings. Second, the assessment of myocardial work parameters and GLS relied on echocardiographic image quality and manual adjustments by the operator, which introduces potential variability despite adherence to standardized protocols. Third, the presence of atrial fibrillation in a subset of patients required the use of multiple cardiac cycles for analysis, which may have influenced the reproducibility of strain and myocardial work measurements. Another limitation is the lack of long-term follow-up data, which prevents evaluation of the prognostic value of myocardial work parameters in patients with concomitant AS and MR undergoing TAVI.
Conclusions
The findings suggest that while GLS remains relatively consistent across different MR severity groups, GCW and GWE tend to decrease in patients with severe MR. This observation may indicate that GCW is a more responsive marker of myocardial function in the presence of concomitant MR. Although these results provide further insight into the interaction between MR and myocardial performance in patients with aortic stenosis, they should be interpreted with caution due to the limitations of the study design. Further prospective research is warranted to validate the clinical relevance of these parameters in this patient population.







