
Introduction
Gastrointestinal parasites infections have widespread distribution across the globe, with the highest burden in developing countries where poor personal hygiene, environmental sanitation, socio-economic, demographic, and health-related behaviours have been documented to influence their transmission. The most familiar means of spread of intestinal parasitic infections is through ingestion of contaminated food and water, but they may also spread from human to human via faecal-oral contact.
Infection with single or multiple species of intestinal protozoa is common in humans and can result in either asymptomatic colonization or symptoms of intestinal disease.
Gastrointestinal problems, mainly prolonged diarrhoea, are a very common feature of hospitalization among travellers returning from intertropical countries. Traveller’s diarrhoea is the most frequent travel-related illness, affecting up to 70% of travellers to certain destinations. Intestinal parasitic infections are ubiquitous in humans, both in urban and rural environments from tropical and subtropical countries. The poorest and most deprived communities are at increased risk of intestinal parasite infections, which are present in more than a quarter of the world’s population [1]. Its aetiology is predominantly bacterial (in approximately 80–90% of cases), but it can also be caused by parasites such as Giardia intestinalis, Cryptosporidium spp., and Blastocystis spp. [2]. Patients suffer from abdominal pains, flatulence, nausea, and numerous loose watery stools. In some cases, the patients’ complaints refer also to dermatologic symptoms such as disseminated urticaria [3].
Moreover, in symptomatic patients careful parasitic stool examination gives evidence of coinfection with several pathogens that are very often associated with irritable bowel syndrome or other intestinal dysfunction [4]. Long-lasting intestinal parasitic infection can be complicated by malnutrition, intestinal obstruction, growth retardation, and immunodeficiency, affecting the socioeconomic development of nations [5]. Protozoal parasites, especially Cryptosporidium sp. and Giardia intestinalis cause diarrhoea and contribute to impaired growth, neurocognitive development, and even mortality [6]. Protozoan parasites that inhabit the proximal small bowel are of particular concern [7]. Parasites affect more than 200,000,000 people annually worldwide. In tropical regions and in low- or middle-income settings its prevalence can be higher [8]. Risk factors include destination, dietary habits, quality of local sanitation, and age – younger adults and children tend to be at higher risk and the traveller’s susceptibility to infection. The increased prevalence in developing countries is likely secondary to overcrowding, poor personal and environmental hygiene, lack of safe water supply, and poor sewerage and waste removal services. Working closely with animals may also be a risk factor for acquisition of protozoa [9]. Approximately 50 million people develop colitis or extra-intestinal disease worldwide as a result of E. histolytica infection, with over 100,000 deaths reported annually. In developed countries amoebiasis is generally seen in immigrants and travellers coming from endemic areas [10]. Persistent abdominal symptoms are common among returning travellers. In the absence of sensitive tests to identify intestinal parasites, gastrointestinal symptoms often remain a diagnostic challenge [11]. Evaluation of travellers with gastrointestinal complaints should include a careful examination for typical infecting organisms such as Giardia and Entamoeba as well as for emerging parasites such as Cryptosporidium, Cyclospora, and microsporidia [12].
Aim
In this work we retrospectively analysed patients from Poznan Tropical and Parasitic Clinic of the Poznan University of Medical Sciences, Poland to evaluate the presence of parasitic infections in the alimentary tract and to find possible correlations between infections, journeys, and gastrointestinal symptoms.
Material and methods and Results
In our study performed between 2015 and 2018 we examined 2561 stool samples obtained from the patients (1321 from men, 1240 for women) hospitalized in the Tropical and Parasitic Department of the Medical University in Poznan, Poland. The patients’ ages were between 19 and 65 years.
The microscopic examinations of patients’ stool samples were performed based on a direct thin smear in 0.9% NaCl, which allowed the assessment of the presence of protozoa life stages (Table I, Figure 1).
Table I
Numbers of cases of positive stool samples and parasite life stages (77 samples, 1 parasite; 18 samples, 2 parasites; 11 samples, 3 and more)
In 106 (62 men, 44 women) (4.14%) cases intestinal parasites were detected: Blastocystis sp. in 73 (48%) probes, Entamoeba coli in 25 (17%) samples, Giardia intestinalis in 24 (16%) cases, Entamoeba histolytica/dispar in 19 (13%) cases, Entamoeba histolytica in 3 (2.0%) cases, Iodamoeba butschlii in 3 (2.0%) stool samples, Endolimax nana in 2 (1.0%) cases, and Cystoisospora belli in 1 (0.5%) case.
In 77 (72.64%) cases we detected one parasite (cysts of Blastocystis hominis in 49 stool samples, cysts of Giardia intestinalis in 16 cases, cysts of Entamoeba coli in 9 cases, and cysts of Entamoeba histolytica/dispar in 3 stool samples), in 18 (16.98%) cases 2 parasites were detected, and in 11 (10.38%) stool samples 3 or more parasites were detected. The presence of the parasite’s morphological elements (trophozoites, cysts, oocysts) were more frequently detected in stools samples originating from travellers to tropical countries, i.e. in 65 of 106 positive samples (61.32%).
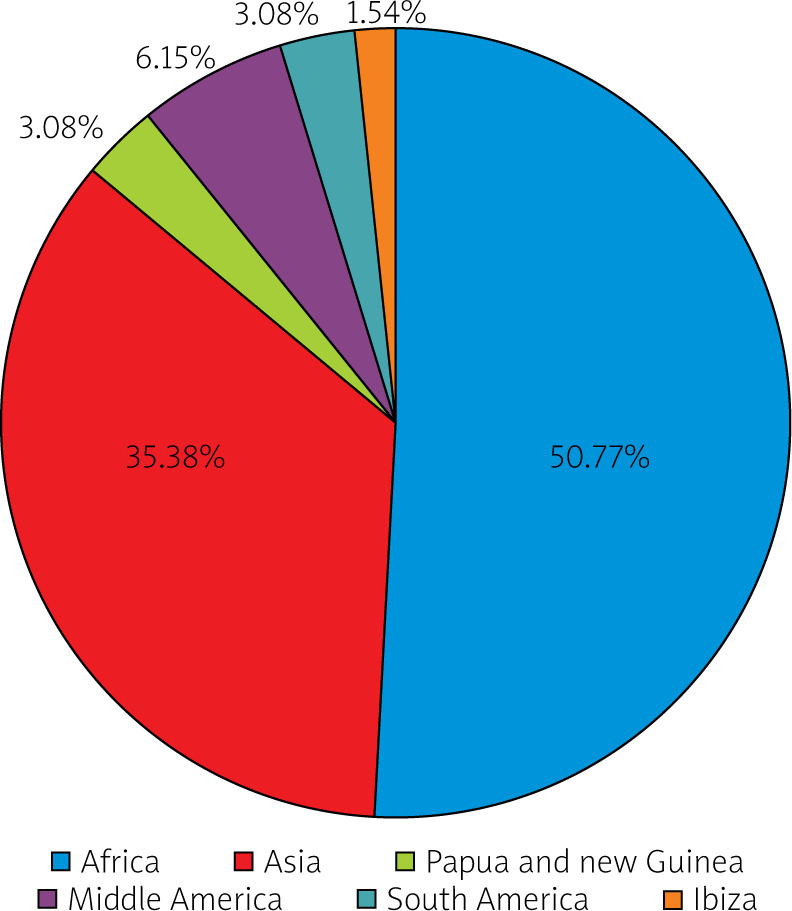
Thirty-three (50.77%) persons returned from Africa, 23 (35.38%) from Asia, 2 (3.08%) from Papua and New Guinea, 4 (6.15%) from Middle America, 2 (3.08%) from South America, and 1 (1.54%) case from the Balearic Islands (Ibiza).
Forty-nine of 106 (46.27%) positive patients suffered from different intestinal symptoms. The most frequent complaints were diarrhoea (loose watery stools) in 32 (65.31%) cases, abdominal pains in 9 (18.37%) cases, irregular stools in 4 (8.16%) cases, flatulence in 1 (2.04%) case, and general weakness in 1 (2.04%) case.
The gastrointestinal complaints were present mainly in patients infected with 2 or more protozoa.
In every symptomatic patient we performed bacteriological stool culture to exclude Salmonella, Shigella, Escherichia coli, Yersinia sp., and Campylobacter sp. infection. In travellers returning from the tropics we also made anal swabs to detect the possible presence of VRE and CPE, and we confirmed 2 patients with Escherichia coli with an NDM-1 resistant mechanism.
Discussion
International travel has increased due to cheaper air fares allowing some of most seemingly inaccessible countries in the world to be reached relatively easily. In 2016, there were estimated to have been 58.2 million international tourists to Africa, 53.6 million to the Middle East, 302.9 million to Asia and the Pacific, 200.9 million to the Americas, and 619.7 million to Europe [13]. Traveller’s diarrhoea, although not life-threatening, is often a vexing problem that impacts the overall functioning of the traveller while on holiday [14]. Ross et al. give in their work proof that of the 2902 clinically significant pathogens that were isolated from human faeces after international trips, approximately 65 were parasitic, 32% bacterial, and 3% viral [15]. Intestinal parasitic infestations, which are a serious public health threat, are distributed throughout the world and are a common problem in third-world countries. Globally, intestinal parasites infect approximately one-third of the total world population, with the highest burden in the tropics and subtropics. In the world, an estimated 1.2 billion, 795 million, 740 million, 500 million, and 2.8 million people are infected with Ascaris lumbricoides, Trichiuris trihciura, hookworm, Entamoeba histolytica, and Giardia lamblia, respectively.
Protozoan parasites are still a serious public health problem, and they are strongly associated with socio-economic conditions. According to Cociancic et al., in studies performed in Argentina almost 70.9% individuals were parasitized. The most prevalent species were Blastocystis spp. (42.7%) and Giardia lamblia (17.6%) [16].
Although parasitic infections belong to the group of WHO neglected diseases, they may range from asymptomatic to chronic or severe diarrhoea and even persistent post-infectious bowel syndrome [17]. Protozoa parasites rarely cause severe life-threatening diarrhoea but they are a major contributor to malnutrition in developing countries. The presence of parasites probably contributes to changes in the composition of the microbiota and activation of immune responses [18]. Amoebiasis is the principal cause of acute diarrhoea. Other intestinal parasites responsible for chronic diarrhoea include Giardia intestinalis, Cryptosporidium spp., and Microsporidium spp. [19]. Giardia intestinalis infections can lead to post-infectious syndrome. Irritable bowel syndrome and chronic fatigue syndrome develop years after this parasite has been eliminated [20]. Hussain et al. in their work indicate that 38% of 256 examined individuals were found to be infected, and the most commonly detected parasites included Blastocystis hominis (47%), Giardia lamblia (38.9%), Entamoeba histolytica (17.9%), Entamoeba dispar (17.9%), and Cryptosporidium hominis (4.2%) [21].
Similar results were obtained by Al-Jawabreh et al., who performed parasitic investigations among the population of the Palestinian part of the Jordan Valley. The overall prevalence of intestinal parasitic infection was 48% from 104 examined stool samples. Thirteen percent of them harboured multiple infections, 10% of which were double and 3% triple. The most frequently detectable agents were Giardia intestinalis (37%), amoebae (19%), Entamoeba coli (8%), Endolimax nana (4%), and Cryptosporidium parvum (6%) [22]. Hailegebriel, in a study performed in Ethiopia among 359 students, detected 235 (65.5%) positive stool samples. The rates of single, double, and triple parasitic infections were 174 (48.5%), 58 (16.2%), and 3 (0.8%), respectively. Among these parasites, E. histolytica/dispar was the most prevalent, at 88 (24.5%) cases, followed by hookworm, at 82 (22%) cases, A. lumbricoides 49 (13.6%), and G. lamblia 41 (11.4%) [23]. The results of a study by Bakarman et al. show that intestinal parasites are endemic in many parts of the world. The prevalence of gastrointestinal tract parasitic infections is variable among populations, and each varies among regions of the same country. The authors indicate that the most commonly detected parasites were Blastocystis hominis (1.7%) and Giardia lamblia (1%). The infestations were both symptomatic and asymptomatic [24]. Similar results were obtained by Barbosa et al., who showed that the overall prevalence in patients from Rio de Janeiro district, by parasitological analysis, was 64.3% (189 out of 294) and the most common protozoa were Blastocystis (55.8%), Endolimax nana (18.7%), Entamoeba histolytica (7.1%), Entamoeba coli (5.8%), Giardia intestinalis (4.1%), and Iodameba butchli (1.0%) [1].
A prospective study performed in Madagascar in 2015 identified a wide panel of intestinal parasites. From 265 stool samples, from whom 67 complained of digestive symptoms (abdominal pains, diarrhoea, bloated feeling), 77% of all subjects were carrying at least one intestinal parasite; 75.9% were protozoa positive, with Blastocystis sp. being the most prevalent (69.8%). The overall prevalence of Entaboeba sp. was 34.0%, Entamoeba coli being the second most prevalent protozoa in this study. There was little difference between the asymptomatic group (73.7%) and the symptomatic group (62.7%) [25].
The risk of gastrointestinal problems varies greatly accordingly to the destination, nationality of travellers, duration of stay, and eating behaviours.
Roure et al. indicated that diarrhoea, abdominal pain, and dysentery were the most frequently recorded symptoms. Diagnosis was made through microbiological examinations. The results showed that the parasites were detected in 46% of immigrants and in 56% of antecedents of any international travels. The most common destinations were the Indian Subcontinent, South and Central America, and Sub-Saharan Africa [26].
Examinations conducted in Munich, Germany on 5378 individuals with intestinal infections showed that among 103 cases with cysts of Entamoeba histolytiuca/dispar, 55 (53.4%) had intestinal co-infections with one or two other pathogenic protozoa, helminths, or bacteria, 41 (39.8%) with Blastocystis hominis, 10 (9.7%) with Giardia lamblia, 2 (1.9%) with Cryptosporidium parvum, and 1 (1.0%) with Giardia lamblia and Isospora belli. Ninety-six stool samples were from travellers. The destinations were as follows: 48 (50.0%) to Asia, 31 (32.3%) to Africa, 8 (8.3%) to Latin America, 2 (2.1%) around the world, and one (1.0%) to Spain [27]. In Iran the overall prevalence of any enteric protozoa in the population was 37.6% (385 out of 1025 cases), with some individual having multiple infections. Giardia lamblia was detected in 179 (17.46%), Blastocystis hominis in 182 (17.76%), Entamoeba histolytica/dispar in 9 (0.87%), and Dientamoeba fragillis in 2 (0.19%) cases. Moreover, non-pathogenic protozoa including Entamoeba coli were detected in 151 (14.3%), Ioedamoeba butschlii in 45 (4,39%), Endolimax nana in 216 (21.07%), Chillomastix mesnili in 22 (2.14%), and Trichomonas hominis in 2 (0.19%) participants [28].
Our investigations gave similar results to those obtained by other scientists. In 106 (4.14%) of 2561 examined stool samples we detected parasites, mainly from people returning from tropical areas (61.32%). Our data showed that most parasites were present in the stool samples of travellers from Africa (almost 51%). The most frequently detected parasites are Blastocystis sp. and Giardia intestinalis. We did not observe a connection between the presence of parasites and gender. Approximately 50% of our hospitalized patients suffered from gastrointestinal symptoms, so a careful microscopic stool examination should be performed in every case in which an intestinal pathology occurs, and certainly in travelling individuals.
Our observations strongly highlighted the correlation between the travel destination and the frequency of protozoa infestations among people, and they suggest a relationship between parasitic infection and intestinal signs.
Although diarrhoea occurs in up to 50% of people who travel to a developing country, it is only one of a number of infectious gastrointestinal illness that travellers may acquire [15].
It is known that the gut microbial communities including protozoa, fungi, bacteria, and viruses share the same environment and live in a close relationship. Their interactions may result in an altered microbiota composition, referred to as dysbiosis. The composition of the intestinal bacterial population modulates the progression of protozoal infection by Entamoeba histolytica, Giardia intestinalis, Blastocystis hominis, and Cryptosporidium parvum, which probably have an immunoregulatory effect of the intestinal autoimmune disorder [29, 30].
Moreover, changes in gut microbiota communities are linked to the pathophysiology of irritable bowel syndrome, which can develope even several months after protozoa infection. Polymicrobic interactions involving protozoa parasites and gut microbiota with biofilm changing and bacterial invasions may also cause persistent post-infection gastrointestinal disorders [31].
However, this protozoa-associated dysbiosis remains poorly understood and requires further examinations.
Conclusions
Traveling to tropical and inter-tropical countries is a risk factor for protozoa infection and gastrointestinal symptoms. The most common parasites detected in the stool samples are Blastocystis sp. and Giardia intestinalis. Parasites should be considered as pathologic agents in patients suffering from abdominal signs. Prolonged protozoa infection and its role in microbiota alterations requires further investigation.











