
Introduction
Motility disorders are a common clinical problem in paediatric patients. The diagnosis is often difficult and time-consuming because its aetiology is heterogenous. Chronic constipation most frequently occurs for functional reasons; however, it may also be caused by alterations in the enteric nervous system. One of the most distinct diseases in newborns is Hirschsprung’s disease (HD), caused by failure of neural crest cells to migrate and form normal plexuses and bowel innervations [1]. Other disorders include desmosis of the colon (DC), neuro-muscular diseases, and inflammatory conditions [2–4]. The treatment depends on aetiology and so it is essential to establish proper diagnosis as soon as possible. The final diagnosis is based on clinical data and histopathology; sometimes imaging tests may be helpful. Rectal biopsy with rapid acetylcholinesterase reaction (frozen sample) is considered as the microscopic gold standard of motility disorder investigation. The evaluation is especially challenging in premature infants because their ganglion cells may be immature and difficult to find, and the ACHE reaction may be negative. To make assessment more reliable and quicker, new immunohistochemical (IHC) stains with formalin-fixed paraffin-embedded rectal biopsy markers have been studied. Calretinin is the most highly recommended stain [5, 6]. It is a calcium-binding protein involved in calcium signalling and is abundantly expressed in neurons. Other markers include the following: microtubule-associated protein-2 (MAP-2), peripherin, neuron-specific enolase (NSE), S100, and CD 117 [7, 8]. If the ganglion cells are present and the child presents clinical symptoms, further diagnosis is very complicated. There are no standards of patient management. Confirmation of desmosis of the colon, a rare condition characterised by total or focal lack of connective tissue net of the circular and longitudinal muscles without any abnormalities within enteric nervous system (ENS), involves full-thickness biopsy and histological staining with Pricrosirius red. Other causes of motility disorders such as neuronal dysplasia or post-inflammatory disorders may require different additional reactions.
Aim
The aim of our study was to create the optimal IHC and histological diagnostic protocol using novel antibodies, as well as to assess their patterns precisely.
Material and methods
Twenty-eight paediatric patients were enrolled to the study. The group consisted of 9 patients with confirmed HD, 11 patients with DC (3) or with chronic constipation of unknown aetiology, and 8 children operated on due to other problems (prior inflammatory bowel disease (IBD). The ages of patients enrolled to the study was from 3 months up to 18 years. They presented with the following: constipation (9); obstruction (6); enterocolitis (1); necrotising ileocolitis (1) and other symptoms of ex-abdominal pain, and diarrhoea (11). Retrospective analysis of full-thickness material from the large intestine was performed. In each specimen the number of ganglion cells was estimated per mm2 counted in 10 HPF (X400) in the muscular plane as well as the myenteric plexus separately. The following IHC and histological stains were also performed: calretinin, CD117, and picrosirius. Patterns (nuclear vs. cytoplasmic vs. membranous) and intensity (strong vs. faint) of the stainings were analysed. The analysis of IHC stains was semi-quantitative as follows: 0 – lack of stain, 1 – faint and focal stain, 2 – strong and focal stain, 3 – strong and diffuse stain.
Results
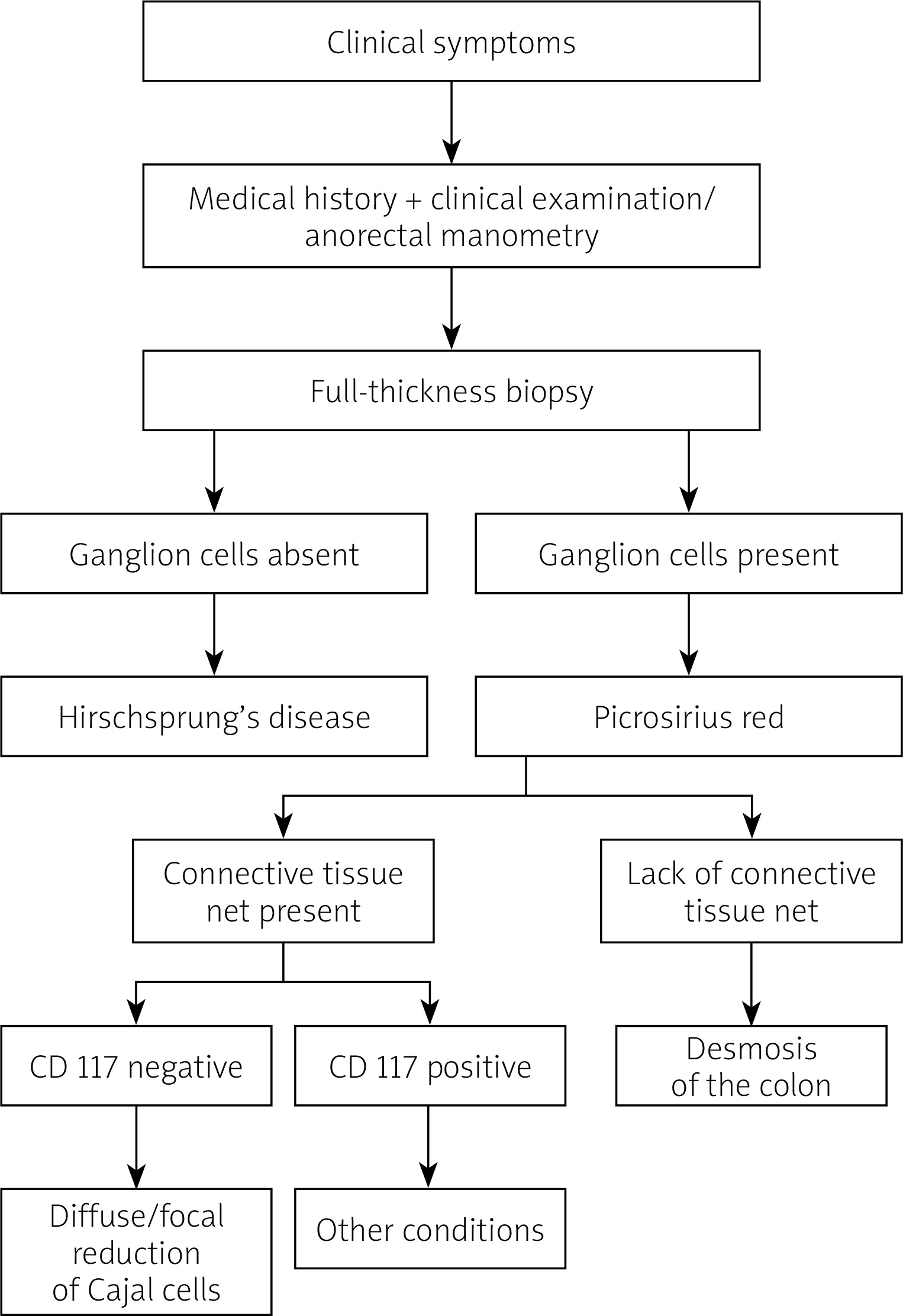
Statistical analysis of histopathological changes did not reveal any significant difference between groups, p > 0.001. Calretinin was positive in each patient with ganglion cells; however, it did not unequivocally stain all cells identified in routine haematoxylin and eosin (HE) staining. Picrosirius red (complete lack of the mesh network of collagen in the intestinal muscular wall) confirmed diagnosis of desmosis coli in each case. Marker CD 117 was not helpful in our group of patients. Therefore, based on our experience and results of statistical analysis, we created a schedule of diagnostic approach in patients with motility disorders (Figure 1).
Discussion
Motility disorders are a common and difficult clinical problem in paediatric patients. Their diagnosis is often time-consuming. Although most of these conditions are functional, in about 5% of cases, organic disorders can be identified [1] and histopathological examination is necessary. In our care centre there are many children with congenital constipation; therefore, it is mandatory to establish proper diagnosis as soon as possible. Based on our experience and literature review concerning useful immunohistochemical stains in the diagnosis of motility disorders in paediatric patients [2–4], we created a schedule of diagnostic approach in rectal biopsy specimens for this group. Aganglionosis should be excluded firstly because it is the most frequent congenital cause of constipation. We chose calretinin as a marker of mature/immature ganglion cells because it is believed to be the most reliable staining [5, 6, 8–13]. It can be particularly useful for less experienced pathologists. In our study it was helpful because the reaction was positive in all patients with presence of ganglion cells, but it did not stain all cells that were transparent in routine HE reaction. Therefore, we believe that no IHC staining can replace experienced a paediatric pathologist. If HD is ruled out, full-thickness surgical biopsy of the large intestine should be performed to exclude desmosis of the colon. It is a rare condition, but in our hospital it occurs relatively often. Histological staining with Picrosirius red showing complete lack of the mesh network of collagen in the intestinal muscular wall confirms the diagnosis. In both HD and desmosis of the colon surgery is a treatment of choice, but if they are excluded, we suggest performing c-kit/CD117 staining to prove the presence of Cajal cells, which control bowel muscular activity. Absence or reduction of the number of Cajal cells may cause chronic pseudo-obstruction [6]. In our group we did not identify any patient with this entity. Becheanu et al. [14] suggested that receptors for CD 117 and CD34 are also decreased in Crohn’s disease. In our study IBD patients were included as controls, but we did not prove any statistically significant difference between them and the studied group. Further trials on larger numbers of patients are needed. After excluding all these disorders there are still other diseases such as enteric neuropathies or myopathies that should be taken into consideration. It is important to remember that diagnosis of congenital constipation has to be based on the patient’s medical history and should also include radiological examination or anorectal manometry. Histopathology is useful in some cases, but in many patients it does not contribute to final diagnosis. Watchful waiting is then the best management because the clinical problem may be functional.











