
Introduction
Transitional cell carcinoma (TCC) of the endometrium is an extremely rare histologic subtype of endometrial carcinoma. While TCC accounts for less than 2% of ovarian cancers [1], only a few cases have been described in the cervix, fallopian tubes, adnexa uteri, and endometrium [2]. The first case of endometrial TCC was reported by Chen in 1990 [3]. To date, only 22 cases have been reported in the literature, most of which were diagnosed at advanced stages due to symptomatic presentation and evidence of myometrial invasion. Our case contributes to this limited body of knowledge by illustrating a rare presentation of endometrial TCC in an asymptomatic patient with two prior negative endometrial curettage results, highlighting the importance of routine gynaecological evaluation and long-term follow-up – even when initial findings are benign.
Case report
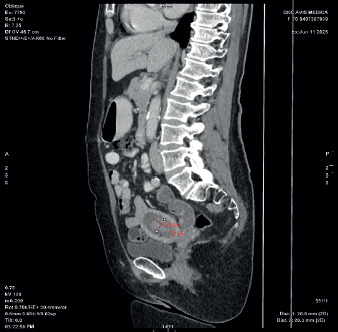
A 70-year-old woman was admitted for evaluation of a growing endometrial lesion identified on a computed tomography (CT) scan. She had no relevant comorbidities other than prior appendectomy and Caesarean section. She reported no allergies or relevant family history. She remained asymptomatic for one year and underwent two dilation and curettage procedures, both of which revealed no pathological findings. She remained asymptomatic throughout. On physical examination she presented in Eastern Cooperative Oncology Group. Gynaecological evaluation revealed a normal vaginal and cervical appearance with the uterus in anteversion-flexion and no palpable adnexal masses. Transvaginal ultrasound revealed a thickened endometrial area. The endometrial mass demonstrated interval growth on follow-up imaging. A subsequent CT scan (Figure 1) was performed and confirmed a 26 × 21 mm polypoid lesion protruding into the endometrial cavity, with no evidence of extrauterine spread, lymphadenopathy or ascites. A total laparoscopic hysterectomy with bilateral salpingo-oophorectomy and peritoneal lavage was performed. No gross intra-abdominal abnormalities were noted intraoperatively. The postoperative course was uneventful.
Histological findings
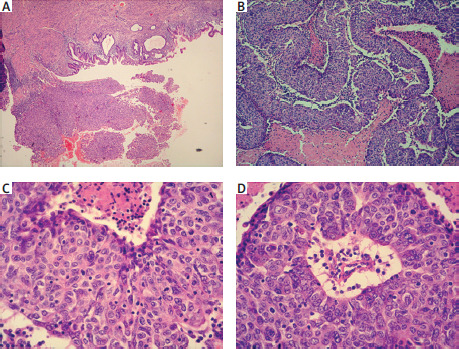
Microscopic examination revealed a malignant neoplasm with a papillary and solid architecture, composed of cells morphologically resembling urothelial epithelium. The tumour cells showed marked nuclear atypia, conspicuous nucleoli, and frequent irregular mitoses, consistent with a high-grade cytologic appearance. Hematoxylin and eosin staining demonstrated these features and is presented in Figures 2 A–D. The lesion was confined to the endometrium, showing only minimal superficial stromal invasion (a few millimetres) and no lymphovascular invasion. The cervix contained benign Nabothian cysts; the fallopian tubes showed fimbrial fibrosis, and the ovaries displayed white bodies, all without evidence of malignancy.
Figure 2
Microscopic finding of the transitional cell carcinoma. A) HE, 10×. B) HE, 25×. C) HE, 25×. D) HE, 25×
Immunohistochemistry
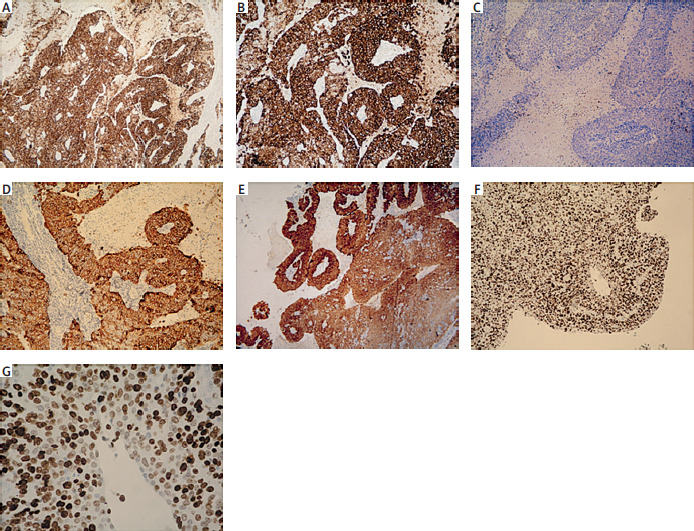
Immunohistochemical analysis demonstrated that the tumour cells were: positive for CK7 (Figure 3 A, B), Vimentin, CK HMW (Figure 3 D), and p16 (Figure 3 E); negative for CK20 (Figure 3 C), GATA3, WT-1, PAX8, and CEA. They also exhibited a very high Ki-67 proliferation index (> 90%) (Figure 3 F,G). This immunoprofile supported a Müllerian origin and confirmed the diagnosis of primary high-grade TCC of the endometrium.Although The Cancer Genome Atlas (TCGA)/ProMisE molecular classification was considered, p53 and mismatch repair (MMR) protein testing was not available, and molecular subtype could not be established.
Staging
Based on the combined surgical and histopathological findings, the tumour was staged as pT1aNxMxLV0 (FIGO IA), indicating that the carcinoma was limited to the endometrium, without myometrial invasion, lymphovascular invasion, or evidence of nodal or distant spread.
Follow-up
At four-month postoperative follow-up, the patient remained asymptomatic and showed no evidence of disease recurrence on clinical and imaging assessment. Given the high-grade morphology of the tumour, she underwent adjuvant radiotherapy, which was completed without complications. Ongoing surveillance is planned to monitor for potential late recurrence.
Discussion
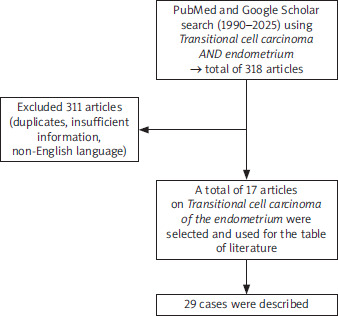
A literature review was conducted to summarize all reported cases and clinicopathological findings of TCC of the endometrium. A search of the PubMed and Google Scholar databases (Table 1) was performed for the period between 1990 and 2025 using the terms “transitional cell” and “endometrial carcinoma.” This search yielded 17 publications in PubMed and Google Scholar describing a total of 29 cases of endometrial TCC (Figure 4). These cases were included in the discussion and are systematically presented in Table 2 [1–10].
Table 1
Searching strategy and key words
| Database | Key words | Total number | Shared articles (PubMed and Google Scholar) | Included in Table 2 |
|---|---|---|---|---|
| PubMed | Transitional cell carcinoma, endometrium | 58 | 12 | 12 |
| Google Scholar | Transitional cell carcinoma, endometrium | 260 | 12 | 17 |
| Total | – | 318 | 12 | 17 |
Table 2
Clinicopathological features of previously reported transitional cell carcinomas of the endometrium
| No. | Author [year] | Age | Symptoms | Size [cm] | Treatment | Histological type | Myometrial invasion | Immunohisto-chemistry | FIGO stage | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Chen, 1990 [3] | 71 | 3-month vaginal spotting | 5.5 × 4 × 3 | TAHBSO | TCC (95%) + endometrioid + mucinous | Outer half | N/A | IIIA | Alive, NED at 5 years |
| 2. | Spiegel et al., 1996 [4] | 75 | Heavy postmenopausal bleeding | 2.8 × 1.6 | TAHBSO ≥ 0.4 | TCC (75%) + endometrioid | Inner third | N/A | IIIA | Alive, NED at 5 years and 15 months |
| 3. | Lininger et al., 1997 [2] | 41 | Dysmenorrhea, weight loss, bowel issues | 0.8 | TAHBSO | TCC (40%) + endometrioid and papillary | 32% | CK7+/CK20– | IIIA | Lost to follow-up |
| 43 | Uterine bleeding | 2 | TAHBSO + RT | TCC (80%) + endometrioid and papillary | 67% | N/A | IC | Lost to follow-up | ||
| 53 | Uterine bleeding | 3 | TAHBSO + chemo | TCC (5%) + endometrioid and papillary | 29% | CK7+/ | IB | Alive, NED at 0.3 years | ||
| 60 | Uterine bleeding | ≥ 1.5 | EMC only | TCC (95%) + squamous | N/A | CK20– | I | Lost to follow-up | ||
| 64 | Uterine bleeding | 7 | TAHBSO + RT | TCC (70%) + endometrioid + sero-papillary | 80% | CK7-/ | IC | Alive, NED at 2.9 years | ||
| 73 | Widespread colon cancer | ≥ 0.4 | EMC only | TCC (95%) + squamous | N/A | CK20– | I | Died of other disease at 12.9 years | ||
| 76 | Uterine bleeding | 5 | TAHBSO + RT | TCC (75%) + endometrioid + squamous | 95% | CK7+/ | IC | Alive, with recurrence at 1 year | ||
| 83 | Uterine bleeding | 3.2 | TAH + vaginal RT | TCC (50%) + squamous + spindle cell sarcoma | 38% | CK20+ (focal) | IB | Alive, NED at 8.2 years | ||
| 44 | Unknown | 16.5 (ovarian) | TAHBSO + RT | papillary TCC, endometrioid, serous, clear cell, squamous | N/A | CK7-/ | IIA (meta-ovary) | Died of disease at 4.8 years | ||
| 4. | Fukunaga et al., 1998 [5] | 50 | 4-month vaginal bleeding, lower abdominal pain, anaemia | 10 × 6 × 4 | TAH + chemo | TCC (95%) + endometrioid | Inner third | CK7+/ CK20– | IB | Alive, NED at 7 years and 7 months |
| 5. | Labonté et al., 2001 [6] | 46 | intermenstrual bleeding, leukorrhea of several months’ duration | 8 × 7 × 3 | TAHBSO + selective pelvic and para-aortic lymphonodectomy, infracolic omentectomy + RT | TCC (90%) + endometrioid | Outer half | CK7+/ CK20– | IV | Alive, NED at 6 months |
| 6. | Lum et al., 2005 [7] | 77 | abdominal pain, and offensive vaginal discharge | 8.6 × 5 | endometrial pipelle biopsy + RT | N/A | N/A | CK7+/ CK20– | IV | Alive, NED at 18 months |
| 7. | Ahluwalia et al., 2006 [8] | 78 | postmenopausal bleeding | 2 | Hysteroscopy + EMC + TAHBSO | TCC (95%) + endometrioid | 1 mm | CK7+/ CK20– | IB | Alive, NED at 10 months |
| 8. | Giordano et al., 2007 [9] | 61 | postmenopausal bleeding | 1.5 × 1.5 | TAHBSO + selective pelvic and paraaortic lymphonodectomy, omentectomy | TCC (100%) | N/A | CK7+/ CK20– | IB | N/A |
| 9. | Ribeiro-Silva, 2007 [10] | 84 | Postmenopausal bleeding, pelvic pain of 2 months | 5 × 3 × 3 | TAHBSO | TCC (15%) + squamous + papillary | N/A | CK7-/ CK20– | IB | Died after 1 year |
| 10. | Mariño-Enríquez et al., 2008 [11] | 63 | Postmenopausal uterine bleeding | 3.7 | TAHBSO | TCC (50%) + endometrioid | Inner half (6 mm) | CK7+/ CK20– | IB | Alive, NED at 16 months |
| 77 | Postmenopausal uterine bleeding | 5.5 | TAHBSO + selective PLND | TCC (90%) + endometrioid | Inner half (3 mm) | CK7+/ CK20– | IIB | Alive, NED at 8 months | ||
| 55 | Postmenopausal uterine bleeding | 4 | TAHBSO + selective PLND | TCC (100%) | Inner half (6 mm) | CK7+/ CK20– | IB | Alive, NED at 15 months | ||
| 73 | Postmenopausal uterine bleeding | 6.5 | TAHBSO | TCC (20%) + endometrioid | N/A | CK7+/ CK20– | IB | Alive, NED at 6 months | ||
| 76 | Postmenopausal uterine bleeding | N/A | TAHBSO | TCC (80%) + endometrioid | Inner half (5 mm) | CK7+/ CK20– | IB | Alive, NED at 3 months | ||
| 11. | Tong et al., 2013 [12] | 66 | Intermittent vaginal bleeding | 3.5 | TAHBSO | TCC (100%) | N/A | CK7+/ CK20– | IB | N/A |
| 12. | Cuccia et al., 2018 [13] | 65 | Postmenopausal uterine bleeding | 2.2 × 1 | TAHBSO | TCC (100%) | Less than one half | CK7+/ CK20– | IB | Peritoneal relapse after 43 months |
| 13. | Cubo-Albert et al., 2018 [14] | 40 | Vaginal bleeding | 3 × 2 | TLH + BSO + pelvic and para-aortic lymphonodectomy + chemotherapy | TCC (100%) | < 50% | CK7+/ CK20– | IIIC | Alive, 7 months MRI residual pelvic disease, began RT |
| 14. | Azzakhmam and Oukabli, 2020 [15] | 62 | Postmenopausal uterine bleeding | N/A | Hysterectomy | TCC (15%) + squamous papillary | N/A | N/A | IB | |
| 15. | Sahu et al., 2020 [16] | 62 | Postmenopausal uterine bleeding | N/A | TAHBSO | TCC (100%) | N/A | CK7+/ CK20– | IB | N/A |
| 16. | Amjad et al., 2022 [17] | 58 | Postmenopausal uterine bleeding | 0.1 | TAHBSO + BPLND | TCC (100%) | N/A | CK7+/ CK20– | II | Alive |
| 17. | Berhili et al., 2022 [1] | 58 | Abdominal mass, whitish leukorrhea, intermittent vaginal bleeding lasting for 2 months | 7 × 7 × 5 | TAHBSO | TCC (100%) | 0 mm | CK7+/ CK20+ | IA | Alive, NED at 5 years |
| 18. | Berhili et al., 2022 [1] | 70 | Growing endometrial mass | 2.6 × 2.1 | TLH + BSO | TCC (100%) | 0 mm | CK7+/ CK20- | IA | Alive, NED at 1 month |
These cases demonstrate a wide age distribution (41–84 years), with a predominance among postmenopausal women, consistent with other forms of endometrial carcinoma. Postmenopausal bleeding was the most common presenting symptom, although a minority of patients reported pelvic pain, discharge, or were entirely asymptomatic. The present case is notable for no reported symptoms, despite progressive tumour growth, and two prior negative biopsies, highlighting the importance of vigilance and imaging follow-up even after benign pathology.
Tumour sizes varied from 0.1 cm to over 10 cm, with a median around 3–4 cm. Most TCC of the endometrium demonstrated mixed histologic features, incorporating endometrioid, serous, squamous, or papillary components. However, in at least 10 of the 30 cases (including ours), a pure or near-pure TCC pattern (≥ 95%) was identified, suggesting a spectrum of differentiation. Our case showed 100% TCC architecture with no associated histologic subtype, confirming the diagnosis of primary pure TCC.
Transitional cell carcinoma is typically high-grade and often presents with mixed histology, including papillary TCC, endometrioid, serous, clear cell, or squamous components. However, this aggressive appearance under the microscope does not always mean the cancer will behave aggressively. In our review, several patients had high-grade tumours that were limited to the endometrium (Stage IA or IB), and most of them stayed disease-free after surgery, with no recurrence during follow-up. This suggests that early-stage TCC, even when it looks aggressive, may have a good prognosis if caught and treated early.
Myometrial invasion was documented in most cases among the 30 patients, depth of invasion ranged from no invasion (0 mm) to involvement of the outer half of the myometrium. Several cases, including the present one, showed tumours limited to the endometrium without any myometrial invasion, corresponding to FIGO Stage IA. In contrast, others demonstrated varying degrees of penetration, with some extending into the inner third, inner half, or outer half of the myometrium. A higher percentage of transitional cell component (≥ 50%) was frequently associated with deeper invasion. These findings support the importance of assessing the extent of myometrial invasion for accurate staging and prognostication, as deeper invasion is a known risk factor for recurrence and may influence decisions regarding adjuvant therapy.
Since previously published cases and our case lacked the molecular data required to utilize the FIGO 2023 molecular classification, we used the FIGO 2018 staging system for consistency with previously reported cases. Additionally, the TCGA/ProMisE molecular classification – now widely highlighted in endometrial carcinoma – was not applicable since p53 and MMR protein expression were not examined. One major knowledge gap is the lack of molecular data in published cases. The Cancer Genome Atlas/ProMisE patterns (such as POLE-mutated, MMR-deficient, p53-abnormal, or no particular molecular profile) may offer crucial information about tumour biology, prognosis, and the best way to treat this uncommon subtype as more cases undergo molecular profiling.
Consistent with previous findings, CK7 positivity and CK20 negativity were the predominant immunohistochemical pattern in endometrial TCC, distinguishing them from urothelial carcinomas of the bladder or metastatic ovarian TCC. Our case aligned with this profile (CK7+, CK20–, GATA3–, PAX8–), confirming its Mullerian origin. High Ki-67 index (> 90%) further emphasized the tumour’s proliferative activity, even in the absence of invasion.
Surgical management was the mainstay across all reported cases, typically involving total abdominal hysterectomy with bilateral salpingo-oophorectomy. Adjuvant therapies (radiation or chemotherapy) were variably employed depending on the stage and risk factors. Among patients with localized disease and no vascular invasion, surgery alone often sufficed.
Of the 30 cases, 21 had reported follow-up; 75 were alive with no evidence of disease, 2 had local recurrence, and 2 died – one from disease and one from unrelated causes. This indicates that primary endometrial TCC, although rare and histologically high-grade, may not necessarily behave more aggressively than conventional endometrial carcinomas, especially if diagnosed early.
Conclusions
Primary TCC of the endometrium is an uncommon histologic diagnosis. Even though it frequently has high-grade cytological characteristics, if caught early and limited to the endometrium, it may grow slowly. For an exact diagnosis, histopathological and immunohistochemical profiling is still necessary.
Despite having a high proliferative score, the current case adds significantly to the small body of research because it is a pure TCC without invasion or recurrence. Due to the disease’s rarity, there are no standard treatment regimens; instead, multidisciplinary evaluation and individual risk factors should inform therapy choices. Further reporting of similar cases is needed to clarify prognostic markers and optimal management strategies for this unusual tumour type.








