
Valve dislodgement during transcatheter pulmonary valve implantation is an uncommon but potentially serious complication [1]. In rare cases, the valve may embolize into the right ventricle or pulmonary arteries, often necessitating surgical retrieval. We present the technical aspects and rescue techniques that ultimately enabled the implantation of an embolized Melody valve (Medtronic, USA) in the pulmonary trunk.
A 23-year-old man with a history of tetralogy of Fallot repair at 6 months and biological pulmonary valve replacement at 15 years presented with progressive exercise intolerance. Imaging confirmed severe stenosis and mild regurgitation of the pulmonary conduit.
Percutaneous valve implantation was planned. Due to bilateral femoral vein occlusion, access was obtained via the right internal jugular vein and left femoral artery. The pressure in the right ventricle was 69/5–10 mm Hg, pulmonary artery 28/14/19 mm Hg, and systemic 89/61/72 mm Hg, indicating significant outflow tract obstruction. After excluding coronary collision, we implanted a CP stent mounted on a 22 × 45 mm BIB balloon (Numed, USA) into the pulmonary trunk as a landing zone.
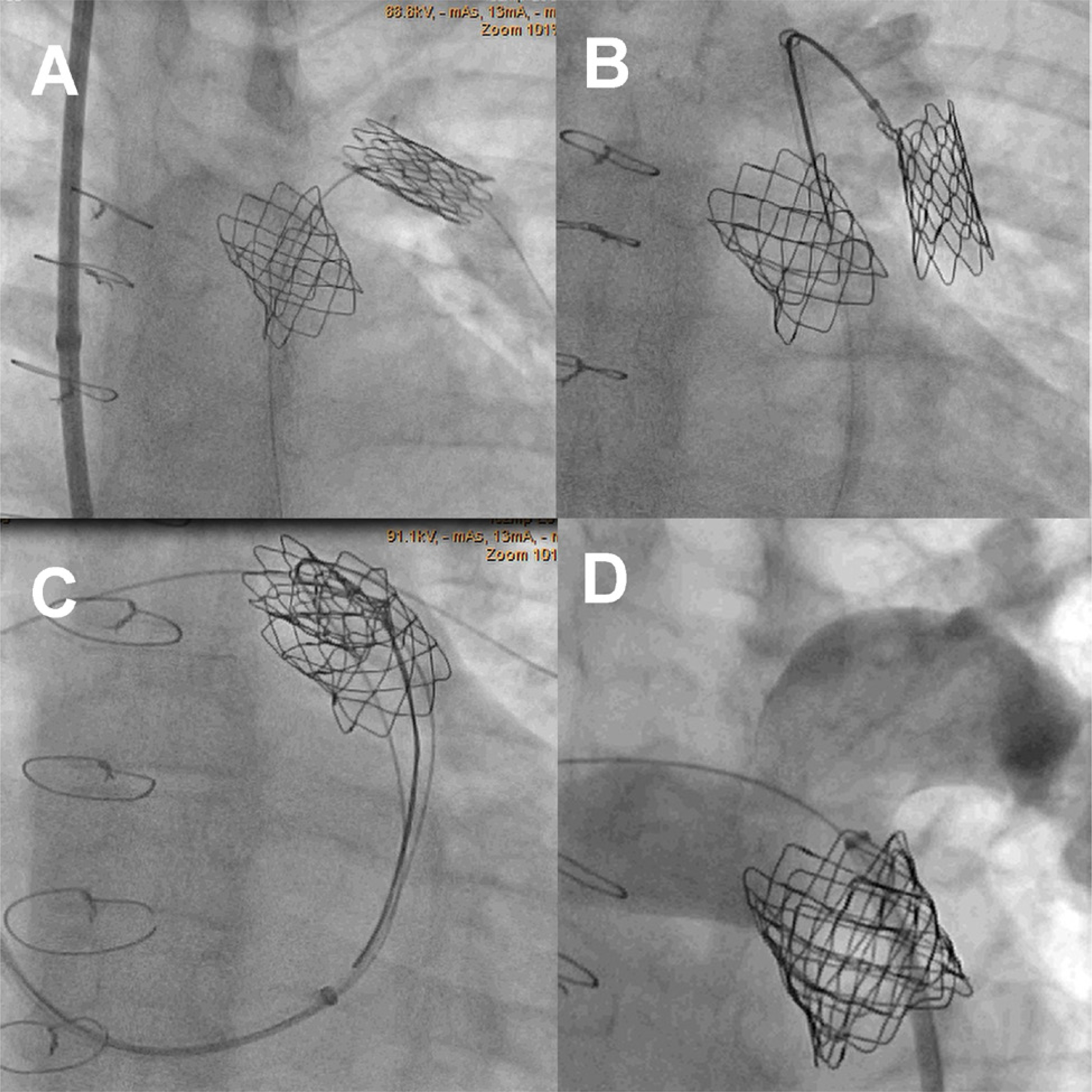
A Melody valve was advanced over a Cook Lunderquist wire (Cook Medical, USA) positioned in the left posterior basal artery. During deployment, an episode of ventricular tachycardia occurred, leading to valve dislodgement from the balloon to the proximal part of the delivery system. An attempt to reposition the valve on the delivery balloon was unsuccessful, and ultimately the valve embolized to the left pulmonary artery (Figure 1 A).
Figure 1
A – Melody valve embolized to the left pulmonary artery. B – Embolized Melody valve held with loop. C – Melody valve with two guidewires positioned in the left and right pulmonary artery held with the loop. D – Final result with competent implanted Melody valve
Following multidisciplinary consultation, a percutaneous rescue strategy was pursued.
First, we exchanged the Ensemble delivery system for a long 14F Dryseal sheath (W. L. Gore, USA) and introduced a 20 × 45 mm BIB balloon over the guidewire. Using the partially inflated balloon and the long sheath, we repositioned the valve back into the landing zone. However, during inflation of the outer balloon, the valve slipped again and embolized back into the left pulmonary artery.
A second rescue strategy involved grasping the stent strut using a 20 mm Multi-snare (Pfm Medical, Germany) (Figure 1 B) and retrieving the valve into the pulmonary trunk. To prevent further displacement during deployment, two Amplatz Super Stiff guidewires (Cook Medical, USA) were inserted through the valve into the right and left pulmonary arteries – the “buddy wire” technique [2] (Figure 1 C). After releasing the valve from the snare, we advanced a 20 × 40 mm Atlas balloon over the guidewire into the lumen of the Melody valve and fully expanded the valve within the pulmonary trunk. Subsequently, we performed a redilation of the Melody valve with a 22 × 40 mm Atlas balloon. Final angiography confirmed optimal valve positioning with a residual systolic gradient of 7 mm Hg and no regurgitation (Figure 1 D).
This case highlights two critical technical considerations. First, if the valve is capable of rotating after embolization, ensuring proper valve orientation becomes essential. In our case, a bent stent strut served as a visual marker indicating the bottom of the valve; otherwise, contrast injection into the valve would have been necessary to confirm its orientation. Second, using dual guidewires stabilized the valve and minimized the risk of re-embolization during final deployment.







