Optical coherence tomography (OCT)-guided percutaneous coronary intervention (PCI), in comparison with angiography-guided PCI, helps to establish the diagnosis, define the treatment plan, and improve outcomes. However, its widespread adoption is still limited [1]. We present an OCT image in a patient after out-of-hospital cardiac arrest (OHCA), which changed the treatment course and allowed the deferred PCI to be conducted. A 61-year-old female patient with a history of atrial fibrillation (AF), ischemic stroke, type 2 diabetes and hypercholesterolemia was admitted because of OHCA due to ventricular fibrillation. After a successful resuscitation, electrocardiography showed evolution of the anterior ST-elevation myocardial infarction. Coronary angiography revealed normal coronary arteries and a large thrombus in the left anterior descending (LAD) artery with TIMI 3 flow (Figure 1 A). Considering chest pain resolution in the catheterization laboratory with no possibility to identify the place of plaque rupture and the risk of no-reflow associated with ad hoc PCI due to distal embolization, the decision to defer PCI was made. Eptifibatide was administered periprocedurally, and the patient was discharged home on triple antithrombotic therapy (acetylsalicylic acid, clopidogrel, rivaroxaban). After 2 weeks, the follow-up angiogram showed a normal LAD with no signs of plaque or thrombus (Figure 1 B). However, the OCT showed a clear plaque rupture in the mid LAD, defining the diagnosis and prompting PCI with a short stent (Figure 1 C). Since currently there are no clear guidelines regarding the treatment of patients with a large thrombus burden, the treatment options range from direct stenting with or without distal protection devices to deferred PCI or no PCI at all [2]. The risks associated with immediate PCI in this scenario include no reflow and suboptimal stent choice (too long or too small). Deferred PCI using stents or drug-coated balloons seems to improve outcomes compared to immediate stenting, provided that the patient is stable and there is TIMI 2-3 in the infarct-related artery [3, 4]. In the absence of significant stenosis in the infarct-related artery, patient management without PCI also appears safe [5]. In a prospective observational study including acute coronary syndrome (ACS) patients with a large thrombus burden who had undergone coronary angiography with OCT, 38% of patients were treated stent-free, all with favorable outcomes [4]. The optimal time for follow-up angiography has also not been defined and ranges from 1 day to 1 month. However, the later it is performed after the index event, the less stenting is required (preferably more than 7 days) [3–5]. Since angiography underestimates the thrombus burden, intravascular imaging is crucial to guide treatment in this complex scenario. It enables precise assessment of lesion morphology (plaque rupture vs. erosion vs. calcified nodule), length, and diameter, thereby avoiding PCI with implantation of too long or too short stents and reducing the risk of recurrent thrombotic events [3–5]. In our case, OCT provided information that could not be obtained with coronary angiography, helping to establish the diagnosis of coronary plaque rupture as a cause of OHCA and guide further management.
Figure 1
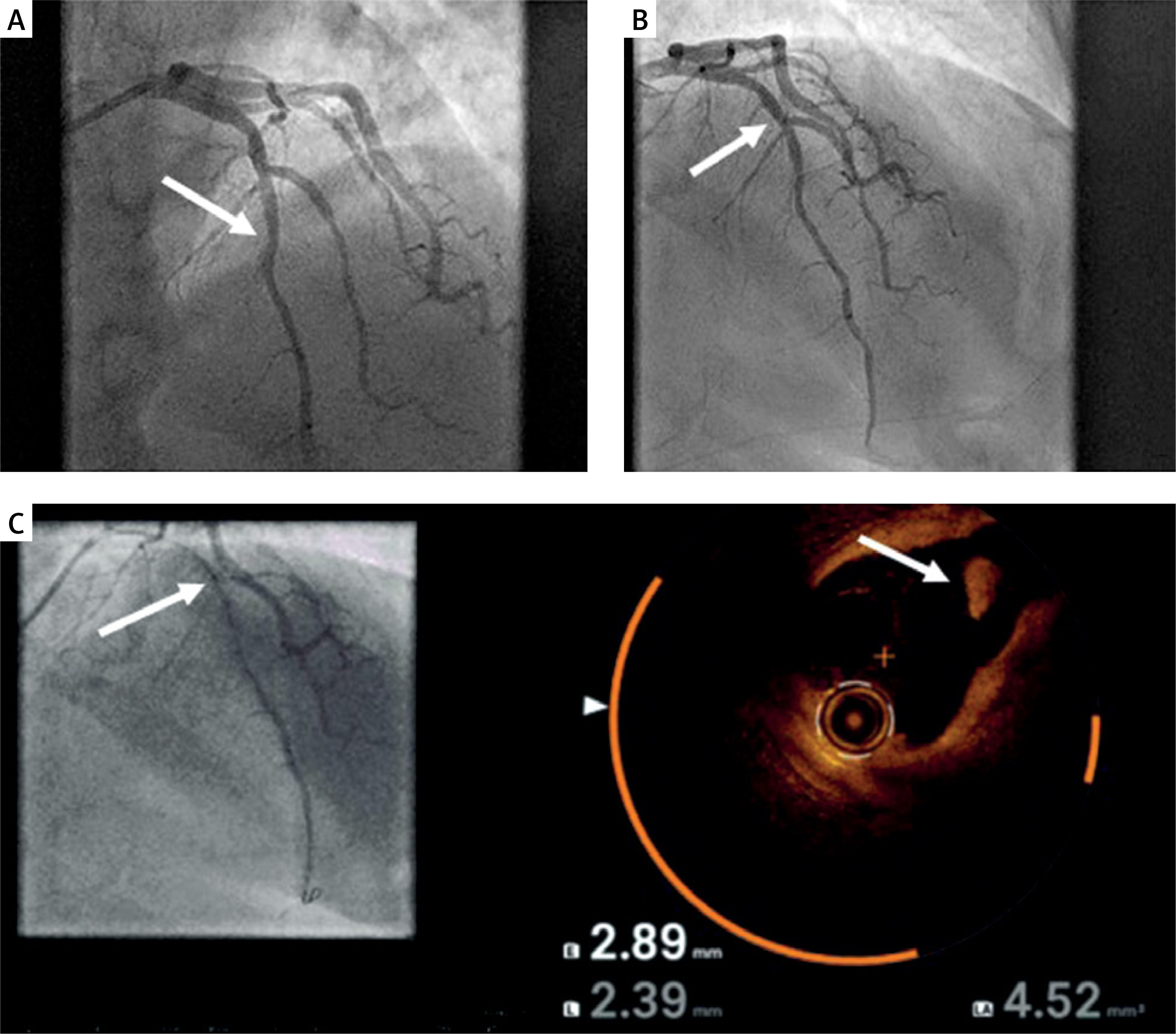
A – Coronary angiography showing thrombus in left anterior descending coronary artery (LAD; white arrow); B – Follow-up coronary angiography after 2 weeks of triple antithrombotic therapy with no signs of plaque or thrombus in LAD; C – Coregistration of angiography and optical coherence tomography showing plaque rupture in the mid LAD segment (white arrow)