
Introduction
Among the recognised gynaecological aetiologies of chronic pelvic pain (CPP) are pelvic venous disorders (PeVD) and adenomyosis [1]. These entities may coexist, producing overlapping symptomatology and reciprocal exacerbation that complicates clinical assessment and management.
Case report
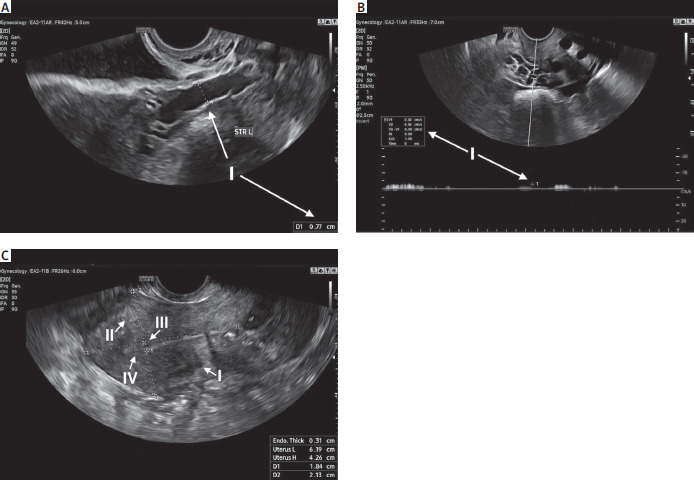
A 45-year-old multiparous woman (three prior vaginal deliveries) was referred for management of CPP. She reported persistent abdominal, lumbar and hip pain, exacerbated by prolonged standing and associated with postcoital discomfort. Menstrual symptoms comprised marked dysmenorrhoea and menorrhagia, culminating in anaemia (haemoglobin – Hb, on admission 9.8 g/dl). Transvaginal ultrasonography demonstrated findings in keeping with PeVD: dilatation of the left ovarian vein to 7.7 mm (cut-off diameter – 6 mm) (Figure 1 A) with reduced blood-flow velocity of 2.82 cm/s (cut-off velocity – 3.0 cm/s) (Figure 1 B). Concurrent sonographic features of adenomyosis were evident, including myometrial cysts (Figure 1 CI), hyperechogenic islands (Figure 1 CII), subendometrial lines and buds (Figure 1 CIII) and an irregular junctional zone (Figure 1 CIV) [2–5].
Figure 1
A) Transvaginal ultrasonography (TVUS) examination revealing signs of pelvic venous disorders (PeVD) – dilatation (7.7 mm) of the left ovarian vein (cut-off diameter – 6 mm). B) TVUS examination revealing signs of PeVD – low blood flow (2.82 cm/s) in the left ovarian vein (cut-off velocity – 3 cm/s). C) TVUS examination revealing signs of adenomyosis – myometrial cysts (I), hyperechogenic islands (II), subendometrial lines and buds (III) and irregular junctional zone (IV)
Over the 24 months preceding hospitalisation the patient received pharmacotherapy with dienogest and venoactive agents, started lifestyle modifications, and underwent pelvic-floor physiotherapy [6, 7]. Despite these measures, symptoms persisted.
As conservative management proved ineffective and the patient declined surgical intervention, she was deemed eligible for simultaneous embolisation of the uterine arteries and ovarian veins. Eligibility was determined in accordance with the Lublin Protocol for Uterine Artery Embolisation by a multidisciplinary team of gynaecologists, interventional radiologists, and angiologists following pelvic magnetic resonance imaging (MRI) [8].
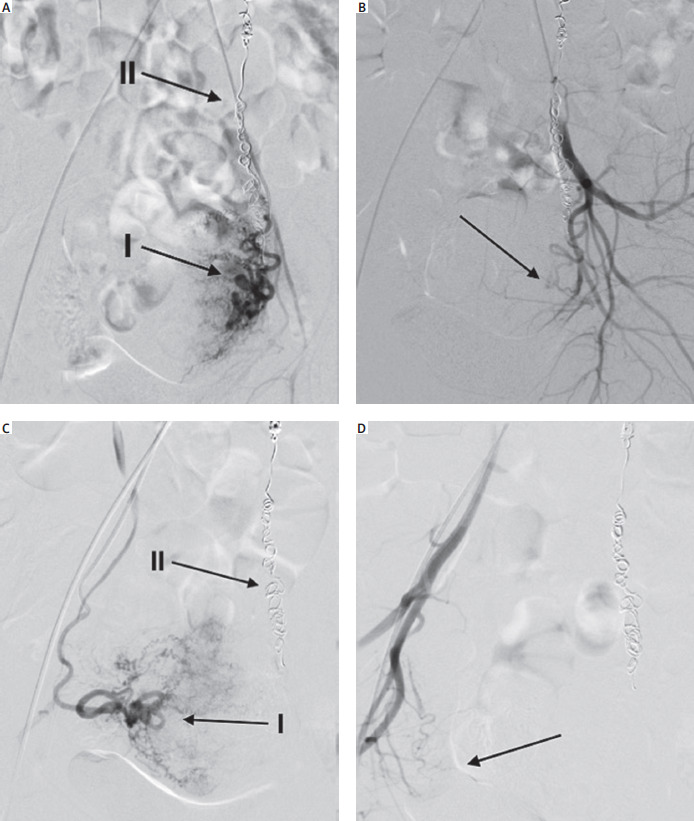
Simultaneous embolisation of the uterine arteries and ovarian veins was performed by an interventional radiologist under local anaesthesia via a right transfemoral approach, with catheterisation of the common femoral artery and vein. Venous intervention commenced with angiography of the left and right ovarian veins, followed by imaging of the iliac venous system; incompetent veins were subsequently embolised using a sclerosing agent in conjunction with a coil. Arterial assessment of the uterine vascular bed was then undertaken and uterine artery embolisation for adenomyosis was performed using 500 µm particulate embolic material (Figures 2 A–D). At completion of the procedure, vascular access was secured by manual compression and application of a pressure dressing.
Figure 2
A) Embolisation of the left uterine artery (I). In the background, spirals used to embolize the left ovarian vein are visible (II). B) Control angiography after the left uterine artery embolisation. No blood flow into the uterine vascular bed was observed. C) Embolisation of the right uterine artery (I). In the background, spirals used to embolize the left ovarian vein are visible (II). D) Control angiography after the right uterine artery embolisation. No blood flow into the uterine vascular bed was observed
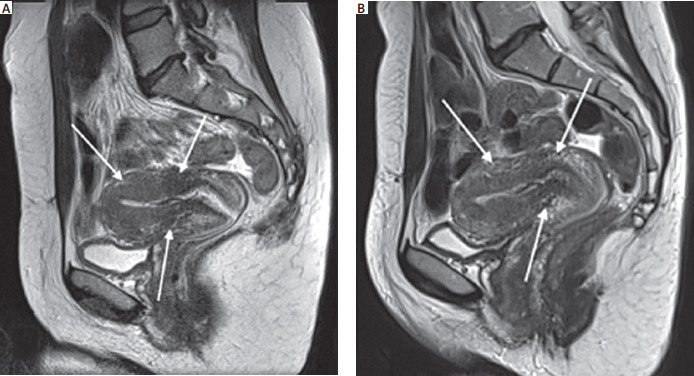
The patient was discharged on postoperative day 2 following an uncomplicated perioperative course. At six-month review, previously reported symptoms – abdominal, lumbar and hip pain, dysmenorrhoea, and menorrhagia – had resolved completely. Postcoital ache persisted but with markedly reduced intensity, the Visual Analogue Scale score declining from 7 to 3. After two months of oral iron replacement therapy, Hb concentration rose to 12.3–9.8 g/dl at admission. Follow-up MRI (Figure 3 A) demonstrated features of adenomyosis of diminished severity compared with the previous examination, characterised by lower signal-intensity myometrial foci on T1-weighted sequences (Figure 3 B), and there was no evidence of PeVD. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Figure 3
A) Pelvic magnetic resonance imaging (MRI) conducted before simultaneous embolisation of uterine arteries and ovarian veins revealing features of adenomyosis. B) Pelvic MRI conducted after simultaneous embolisation of uterine arteries and ovarian veins revealing features of less severe adenomyosis (lower signal intensity myometrial foci on T1-weighted imaging)
Conclusions
The case presented herein delineates a novel therapeutic strategy for a patient with CPP. Chronic pelvic pain of complex aetiology is an increasingly prevalent condition in both pre- and post-menopausal women; its heterogeneous pathophysiology, frequent comorbidities and variable clinical presentation render timely diagnosis and effective management particularly challenging.
Whether tumour markers such as CA-125 or CA19-9 should be measured routinely in patients presenting with CPP remains unresolved. In the case reported here, ovarian imaging furnished no oncological concern, and therefore tumour-marker assays were not performed. Furthermore, the embolisation was undertaken in accordance with the Lublin Protocol for Uterine Artery Embolisation, and a preprocedural endometrial biopsy demonstrated normal histology. Nonetheless, when clinical or radiological features raise the possibility of gynaecological malignancy, assessment of CA-125 and CA19-9 prior to intervention would be a prudent precaution [9–11].
To our knowledge, this report constitutes the first description of simultaneous embolisation of the uterine arteries and ovarian veins as a management strategy for CPP secondary to PeVD and adenomyosis. Although the efficacy and safety of this combined endovascular approach require confirmation in appropriately powered, well-designed clinical trials, it appears to represent a promising therapeutic option for patients with CPP of complex, multifactorial aetiology.








