






Cutaneous metastases are not commonly encountered in everyday dermatologic practice, but their appearance indicates an advanced stage of the disease and portends poor outcome. The exact incidence is not well established, but it is estimated that cutaneous metastases account for approximately 0.9–9% of all internal malignancies. The clinical presentation of skin metastases varies significantly, making the diagnosis particularly challenging when the primary cancer is unknown. Moreover, when the cancer diagnosis is already established, distinguishing between skin changes caused by therapy and those resulting from disease dissemination can be difficult. Therefore, histopathological and immunohistochemical evaluation is very valuable for proper diagnosis as metastatic deposits exhibit the same patterns as the underlying primary tumour [1–3]. In men, malignant tumours that most often metastasize to the skin are lung cancer, colon cancer, and melanoma. Among women, the most common tumours that metastasize to the skin are breast cancer, followed by colon cancer, melanoma, and ovarian carcinoma. Additionally, the most frequently affected site of metastases in men is the head and neck region, whereas in women the anterior chest wall [4, 5].
We present the case of a 58-year-old woman who sought dermatologic consultation in October 2023 due to multiple erythematous, firm, non-tender skin papules, plaques, and nodules of varying sizes, accompanied by shallow ulcers around a postoperative scar on her right upper arm (Figure 1 A). Upon clinical examination and a comprehensive review of her medical history, it was revealed that the patient had been admitted to the Gynaecologic Outpatient Department in February 2023 due to vaginal discharge and bleeding. Further examination detected tumorous tissue in the cervix, leading to a biopsy. Pathohistological analysis confirmed invasive squamous cell carcinoma. Pelvic magnetic resonance imaging (MRI) indicated Stage IIIC of cervical infiltration (Figure 2 A), and thoracic multi-slice computed tomography (MSCT) showed no evidence of tumorous dissemination but identified a solitary nodal change in the right lung lobe, likely a granuloma.
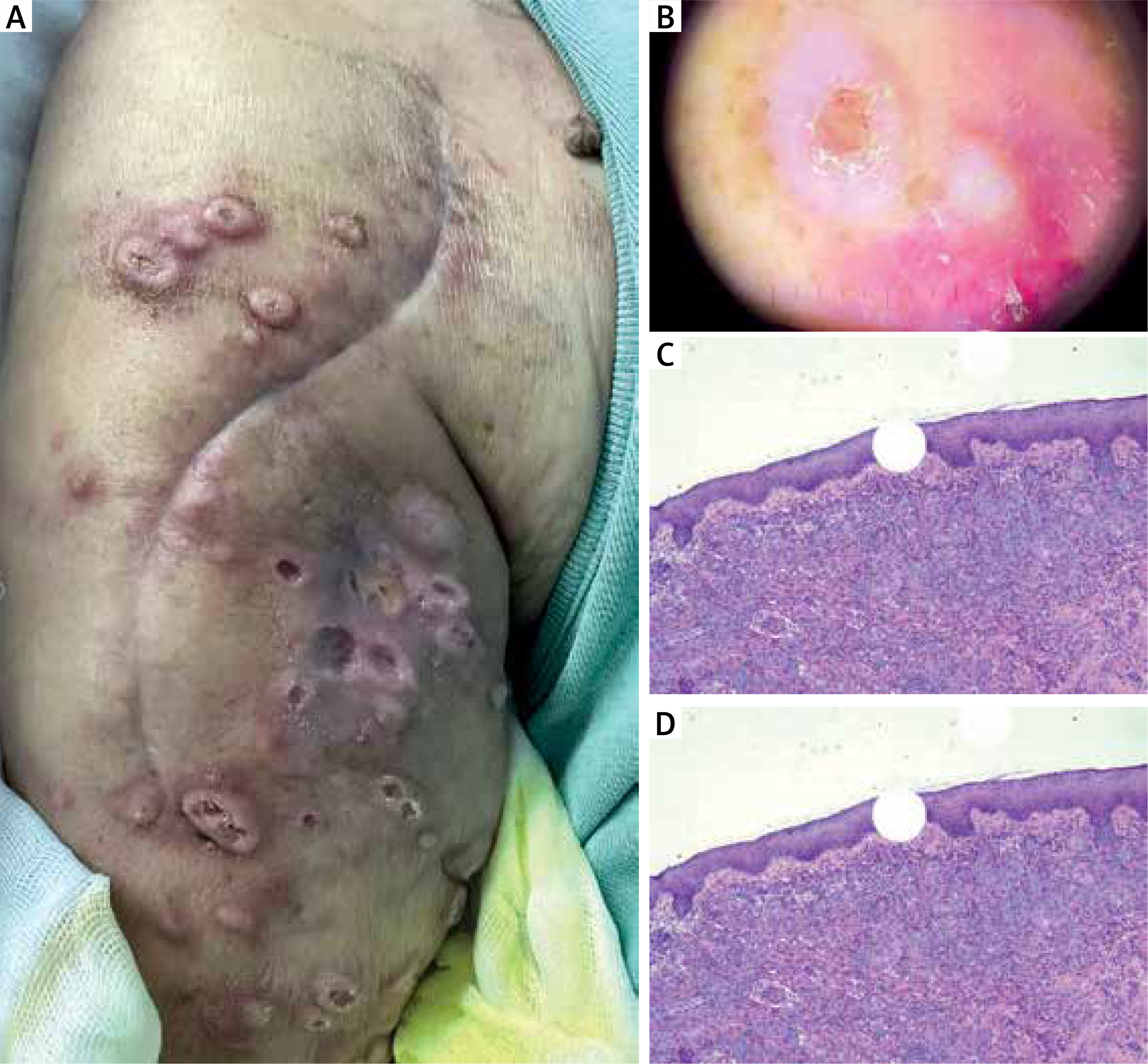
Figure 1
A – Clinical presentation of the skin changes; B – Dermoscopic examination of cutaneous deposits; C, D – Proliferation of neoplastic cells in dermis and adipose tissue; hematoxylin-eosin, original magnification ×40, ×100

Following a thorough evaluation, the Gynaecological-Oncological Board recommended intravaginal brachytherapy along with chemotherapy (HT/CHT/CTX) potentiation. This treatment regimen was completed by mid-May 2023. Based on the TNM classification, the patient was diagnosed with FIGO Stage IIB/IIIC1 disease.
A follow-up thoracic MSCT in late June 2023 revealed a solitary soft tissue lesion in the posterobasal segment of the lower right lung lobe, suggestive of a secondary deposit.
In June 2023, due to severe right shoulder pain, an MSCT was performed, revealing a 21 × 12 mm osteolytic zone at the humeral neck and a 15 × 8 mm zone at the posterior humeral neck contour, consistent with secondary deposits. Considering the atypical nature of cervical cancer metastases particularly to the humerus, a biopsy and pathohistological analysis of these changes were recommended. Consequently, the pathohistological evaluation of the proximal right humerus specimen confirmed joint metastases of squamous cell carcinoma. Additionally, in October 2023 the patient was hospitalized at the Orthopaedic Clinic due to a pathological fracture of the right humerus and the surgical intervention was performed (Figures 2 B, C). During her stay, livid nodules with shallow ulcerations around the postoperative scar were observed, prompting a consultation with a dermatologic oncologist. Dermatoscopic examination revealed signs consistent with cutaneous metastases, including a polymorphic vascular pattern, keratinization signs, central homogenous white zones, peripheral brown pigmented networks, and a polymorphic vascular pattern with arborized, linear, and comma-like blood vessels. Adjacent areas displayed structureless blue surfaces, bright white lines, and fields with brown pepper-like speckles (Figure 1 B). Based on these findings, the dermatologist-oncologist suspected cutaneous metastases and recommended a skin nodule biopsy for pathohistological analysis, which confirmed the presence of metastatic deposits on the skin proximal to the right humerus (epidermis is preserved; in dermis there is a cluster of atypical epithelial cells, pleomorphic nuclei, and visible mitoses with signs of keratinization) (Figures 1 C, D).
Cervical cancer is one of the most prevalent cancers in women. It tends to spread via the lymphatic system. According to a population-based study in 2020, single-site metastases were present in 68.7% of cases. Among these cases, nearly 38% of metastases occurred in the lungs, followed by the joints (primarily the pelvic and spine regions), liver, and brain. According to the available literature, cutaneous metastases from cervical neoplasms are extremely rare [6–8]. The chance of cutaneous metastases occurrence may vary upon the stage of cervical cancer. Thus, in stage I, the incidence seems to be around 0.8%, and in stages II, III, and IV, it is found to be around 1.2%, 1.2%, and 4.8%, respectively [9, 10]. Moreover, while there have been reported cases of cutaneous deposits in various sites of the skin, the occurrence of such deposits on the upper limb is particularly uncommon. It was previously believed that cutaneous metastatic deposits tend to develop in the skin region near the primary tumour [11–13]. Even though skin metastases of cervical cancer are a very rare event, according to the available literature, the most common site for metastatic deposits were found to be the skin in the proximity of lower abdomen and lower extremities. There has been one report showing the cutaneous dissemination of cervical cancer in the scalp [9]. As mentioned above, cervical cancer tends to spread via lymphatics, however haematological dissemination could provide a plausible explanation for remote metastases, and it is most likely the mechanism of dissemination for the deposit in the right humerus. In our patient, the route of dissemination to the skin of the right upper arm is quite intriguing. It could potentially occur via haematogenous spread, although direct implantation from an underlying metastatic deposit in the bone is also a reasonable and highly probable mode of dissemination. All in all, cutaneous metastases are fortunately infrequent in dermatological practice, but they represent the rare entity caused by common malignancies [12]. It should not be neglected that their occurrence is on the rise. This letter serves as a reminder that common malignant neoplasms can give rare cutaneous metastases and reminds of the risks that surgical interventions pose regarding the spreading of the neoplastic deposits.