






Introduction
Breast cancer (BC) is a highly heterogeneous disease, with 2.26 million new cases estimated in 2020, BC has become the world’s most frequently diagnosed cancer and second most common cause of cancer death in women worldwide [1–3].
In Algeria BC occupies the first place with an incidence of 12,536 cases, a prevalence of 38,886 cases, and a mortality rate of 12.5% in 2020 [4].
Breast cancer involves a multi-step process with several cell types. It generally starts with ductal hyperproliferation and progresses to benign tumours and even metastatic carcinomas after being constantly stimulated by various carcinogenic factors [5].
Reactive oxygen species (ROS) are mediators that can induce DNA damage and genomic instability, resulting in the loss of cellular integrity, function, and viability [6]. Breast cancer cells have higher levels of ROS, and DNA damage induced by ROS is strongly associated with the occurrence and development of BC [7]. Most studies have evaluated the systemic pro-oxidative profile of BC patients by measuring the action of free radicals on lipids, known as lipid peroxidation, resulting in the production of aldehydes, such as 4-hydroxy-2-nonenal (4-HNE) and other toxic substances [8, 9]. Interleukin-6 (IL-6) is a pleiotropic cytokine that plays important roles in the immune response, inflammation, and haematopoiesis [10]. The direct effect of IL-6 on BC cell growth is not entirely understood, and results are slightly contradictory, with some studies showing both direct growth inhibitory effects and inhibitory effects on proliferation, while other studies show growth promoting effects [11]. IL-6 expression in BC tissues is related to early stages of the disease. In advanced stages, IL-6 expression predicts a better prognosis [12].
Hypoxia-inducible factor 1-α (HIF-1α) is a transcription factor implicated in carcinogenesis and in the metastatic propagation of tumour cells [13]. In BC, cells react to oxygen reduction by activating HIF-1α, regulating multiple genes involved in metastatic progression [14].
The limitations of existing detection methods indicate the need for alternative tests to assist in the early identification of BC. This need has highlighted the potential value of circulating biomarkers for the early detection of BC [15].
Furthermore, there is a lack of biomarkers to predict BC initiation and progression, and more accurate markers are needed to aid in the differential diagnosis of premalignant breast lesions and disease progression.
The objective of this study was to examine the concentrations of IL-6 and HIF-1α, and to evaluate the oxidative stress by the determination of the marker of lipid peroxidation 4-HNE, as well as to study the correlation with clinicopathological parameters and find the influence of age and molecular subtype on serum levels of these molecules in patients with BC from western Algeria.
Material and methods
Population
The current study is a case-control study. Seventy patients with BC and 23 controls presumed to be healthy were recruited from October 2020 to February 2022 at the University Hospital Establishment of Oran of Oran (Department of Medical Oncology and Department of Gynaecology and Obstetrics), all of whom consented to participation by answering questionnaires and accepting all biological examinations performed on their blood. The dosage of IL-6, 4-HNE, and HIF-1α were established by ELISA technique in the Biology of Development and Differentiation Laboratory (Ahmed Ben Bella Oran 1 University) and the Pasteur Institute of Algeria, Oran Branch (immunology laboratory).
Patients who had received chemotherapy or any other type of cancer therapy and patients with incomplete medical records are not included in this study.
The information collected by the basic questionnaire included socio-demographic and anthropometric characteristics (weight and height), fertility history, hormone use for infertility and menopause, date of cancer diagnosis, anatomopathological characteristics, and family and/or personal history of BC.
For each patient, age, Scarff-Bloom-Richardson (SBR) grade, histologic type, and molecular classification were collected from the medical records.
Methods
The blood is collected from a venipuncture in the fold of the arm on a heparinized tube, and the plasma was separated by centrifugation at 3000 g for 10 minutes and then stored at –80°.
Two ELISA tests were used in our investigations. The ELISA sandwich test for dosage of IL-6 with Human IL-6 ELISA Kit (Product number: Rab 0306) and HIF-1α with Human HIF-1α ELISA Kit (Product number: RAB1057. Laboratoire sigmaaldrich), whereas the ELISA competitive test was used for the dosage of 4-HNE with the 4-HNE ELISA Kit (Catalogue No. abx257639, Laboratoire Abbexa).
The optical density OD was measured spectrophotometrically at 450 nm in a microplate reader, from which the concentration of IL-6, 4-HNE, and HIF-1α was calculated.
Statistical analysis
Statistical Package for Social Sciences version 21.0 was used for the statistical analysis. The Kolmogorov-Smirnov test showed that the data were not normally distributed (p < 0.05), and hence a non-parametric test was used. The Kruskal-Wallis and Mann-Whitney U tests were used to compare the study variables. Spearman’s correlation test analysis was conducted to assess the strength of IL-6, 4-HNE, and HIF-1α serum levels with SBR grade and number of lymph nodes. P < 0.05 was considered statistically significant.
Results
The average age of the patients was 52.37 ±12.23 years.
As shown in Figure 1, the most common age groups were 40–49 years and 50–59 years, with a percentage of 31.4% for each group, the 30–39 year olds and the over 70 year olds with 12.9%, and finally the 60–69 year olds with 11.4%.
Fig. 1
Percentage of breast cancer patients by age group
Descriptive analysis of breast cancer cases shows that the most frequent age groups are 40–49 and 50–59 with 31.4% for each group, followed by 30–39 and over 70 with 12.9% and finally 60-69 with 11.4%.

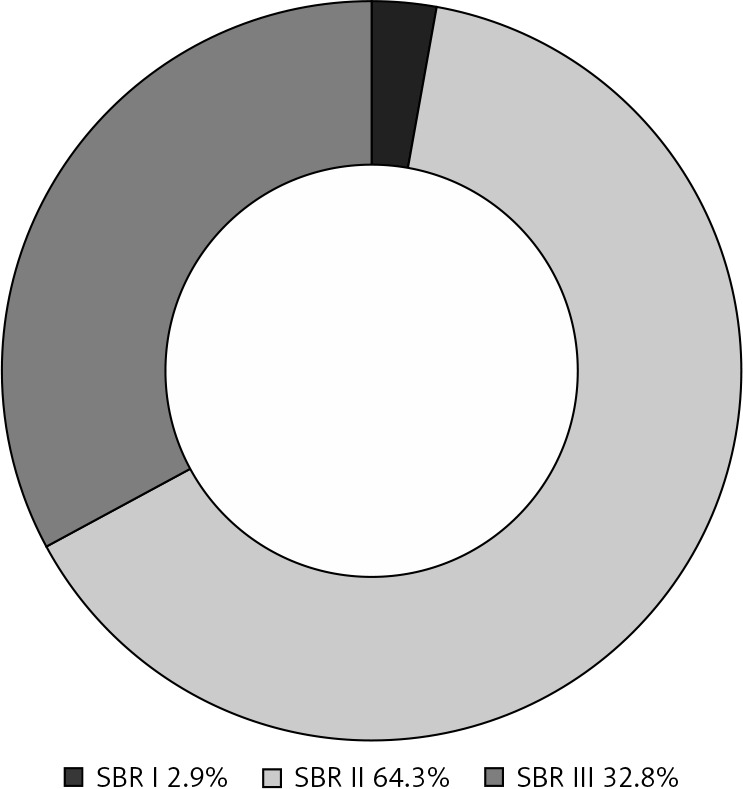
According to the SBR histoprognostic classification of the tumours, more than half of the cases were grade II (64.3%), followed by grade III (32.8%), and grade I (2.9%). Analysis of the SBR prognostic value is shown in Figure 2.
Fig. 2
Scarff-Bloom-Richardson grade of patients
SBR – Scarff-Bloom-Richardson
Scarff-Bloom-Richardson histoprognostic classification of tumors shows that over half of cases belong to grade II with 64.3% of cases, followed by grade III (32.8%) and grade I (2.9%).
Histopathological analysis of BC cases shows that 81.3% were invasive carcinoma of no special type – 57 cases, followed by ductal carcinoma in situ, invasive lobular carcinoma, and metaplastic breast carcinoma – 4.3% for each type (3 cases), and finally invasive micropapillary breast carcinoma and pure mucinous breast carcinoma represent 2.9% (2 cases) for each type.
The results of patients’ histological type of BC are illustrated in Table 1.
Table 1
Patients’ histological types of breast cancer
[ii] Histopathological analysis of breast cancer cases shows that 81.3% are Invasive carcinoma of no special type, followed by ductal carcinoma in situ, Invasive lobular carcinoma and metaplastic breast carcinoma with 4.3% for each type, finally Invasive micropapillary breast carcinoma and Pure mucinous breast carcinoma represent 2.9% for each class.
The immunohistochemical (IHC) study revealed that 35.4% of the tumours were luminal B, 32.3% were triple negative (TN) with absence of progesterone receptor (PR), estrogen receptor (ER), and human epidermal growth factor receptor 2 (HER2) expression, 26.2% were luminal A, 4.6% were luminal (we could not determine whether they were subtype A or B because the Ki-67 test was not performed), and 1.5% were HER2+ overexpression of the HER2 receptor and absence of PR and ER expression. The molecular classification of patients’ tumours is outlined in Figure 3.
Fig. 3
Molecular classification of patients tumours
HER2 – human epidermal growth factor receptor 2
According to immunohistochemical analysis, 35.4% of tumors are luminal B,followed by triple-negative with 32.3% of cases and luminal A, luminal
(we couldn’t determine if it was a subtype A or B because the Ki-67 test was not performed), and HER2+ with 26.2%, 4.6%, and 1.5% of cases respectively.

No significant difference (p > 0.05) was observed in IL-6 serum levels between patients and controls, with p = 0.104; average for patients = 119.42 pg/ml, and for controls = 498.35 pg/ml, standard deviation (SD) for patients = 303.76 pg/ml, and for controls = 650.49 pg/ml.
There was no significant difference (p > 0.05) in serum HIF-1α levels between patients and controls, with p = 0.051; the average for patients = 0.21 ng/ml and for controls = 1.87 ng/ml, SD for patients = 0.71 ng/ml and 4 for controls = 72 ng/ml.
However, a significant difference was observed between patients and controls in terms of 4-HNE serum levels, with p = 0.006; average for patients = 2.66 ng/ml and for controls = 1.73 ng/ml, SD = 1.67 ng/ml and 0.94 ng/ml of patients and controls, respectively.
The results of the comparative analysis are presented in Table 2.
Table 2
Comparison analysis of interleukin-6, 4-hydroxy-2-nonenal and hypoxia-inducible factor 1-α serum levels between patients and controls
| Parameters | Average | SD | p-value | |
|---|---|---|---|---|
| IL-6 [pg/ml] | ||||
| Patients | 119.42 | 303.76 | ||
| Controls | 498.35 | 650.49 | 0.104 | |
| 4-HNE [ng/ml] | ||||
| Patients | 2.66 | 1.67 | ||
| Controls | 1.73 | 0.94 | 0.006 | |
| HIF-1α [ng/ml] | ||||
| Patients | 0.21 | 0.71 | ||
| Controls | 1.87 | 4.72 | 0.051 | |
No significant difference (p > 0.05) was found in the analysis of IL-6 serum levels in different age groups, with p = 0.094; average (SD) = 6.52 (19.58) pg/ml, 202.91 (469.19) pg/ml, 41.37 (78.65) pg/ml, and 172.88 (224.72) pg/ml for age groups 30–39, 40–49, 50–59, and ≥ 70 years, respectively.
No significant difference (p > 0.05) was found in the analysis of 4-HNE serum levels in different age groups, with p = 0.35; average (SD) = 2.67 (1.07) ng/ml, 3.01 (1.83) ng/ml, 2.23 (0.75) ng/ml, and 2.21 (0.92) ng/ml for age groups 30–39, 40–49, 50–59, and ≥ 70 years, respectively.
No significant difference (p > 0.05) was found in the analysis of HIF-1α serum levels in different age groups, with p = 0.738; average (SD) = 0.06 (0.19) ng/ml, 0.28 (0.8) ng/ml, 0.35 (0.97) ng/ml, and 0.01 (0.04) ng/ml for age groups 30–39, 40–49, 50–59, and ≥ 70 years, respectively.
The results are presented in Table 3.
Table 3
Comparison analysis of interleukin-6, 4-hydroxy-2-nonenal and hypoxia-inducible factor 1-α serum levels in different age groups
The results in Table 4 indicate that no significant difference of IL-6 was noted between different molecular subtypes of BC, with p = 0.492; average (SD) = 0 (0) pg/ml, 59.17 (5.38) pg/ml, 21.73 (45.55) pg/ml, 118.79 (225.33) pg/ml, and 228.22 (490.07) pg/ml for molecular subtypes HER2+, luminal, luminal A, luminal B, and triple-negative, respectively.
Table 4
Comparison analysis of interleukin-6, 4-hydroxy-2-nonenal and hypoxia-inducible factor 1-α serum levels in different subtypes molecular of breast cancer
No significant difference in 4-HNE was observed between different molecular subtypes, with p = 0.622; average (SD) = 0 (1.73) ng/ml, 1.96 (0.33) ng/ml, 2.39 (0.67) ng/ml, 2.7 (1.49) ng/ml, and 2.96 (2.42) ng/ml for molecular subtypes HER2+, luminal, luminal A, luminal B, and triple-negative, respectively.
No significant difference of HIF-1α was noted between different molecular subtypes of BC, with p = 0.369; average (SD) = 0 (0) ng/ml, 0 (0) ng/ml, 0.29 (0.96) ng/ml, 0.068 (0.25) ng/ml, and 0.394 (0.939) ng/ml for molecular subtypes HER2+, luminal, luminal A, luminal B, and triple- negative, respectively.
The correlation analysis of patients’ serum of IL-6, 4-HNE, and HIF-1α levels with SBR grade and numbers of lymph nodes is as follows (Table 5):
Table 5
Correlation analysis of patients serum interleukin-6, 4-hydroxy-2-nonenal and hypoxia-inducible factor 1-α levels with Scarff-Bloom-Richardson grade and numbers of lymph nodes
[i] HIF-1α – hypoxia-inducible factor 1-α, Il-6 – interleukin-6, SBR – Scarff-Bloom- Richardson, 4-HNE – 4-hydroxy-2-nonenal
[ii] No correlation (p > 0.05) was observed between serum levels of IL-6, 4-HNE and HIF-1a and SBR grade of tumors and no significant correlation (p > 0.05) was observed between serum levels of 4-HNE, HIF-1a and number of lymph nodes on the other hand IL-6 expression was negatively correlated (p < 0.05) with number of lymph nodes.
there was no correlation (p > 0.05) between IL-6, 4-HNE, and HIF-1α serum levels and SBR grade of tumours with p (correlation coefficient) = 0.248 (0.142), 0.564 (–0.071), and 0.173 (0.165), respectively,
the expression of IL-6 expression was negatively correlated (p < 0.05) with number of lymph nodes, with p (correlation coefficient) = 0.026 (–0.272),
no significant correlation (p > 0.05) was observed between 4-HNE, HIF-1α serum levels, and number of lymph nodes, with p (correlation coefficient) = 0.762 (–0.038) and 0.943 (–0.009), respectively.
Discussion
Breast cancer is known to be a major cause of death and the most common cancer in women [16, 17]. However, the incidence of BC is estimated to be around 260,000 per year, and more than 400,000 will die from this disease [18, 19].
Age is a very important risk factor in BC [20]. The incidence rate of BC increases significantly with age, peaking at the age of menopause and then gradually decreasing or remaining constant [21]. Goswami et al. [22] found that the age range most affected was between 41 and 60 years. Our results are in accordance with these findings.
The average age of patients is 52.37 ±12.234 years. The literature review shows similar averages to our results: 50 ±11.8 years in Algeria [23], 51.1 ±11.2 years in Morocco [24], and 52 years in France [25].
Scarff-Bloom-Richardson grade is a well-established prognostic factor in BC [26]. In our study we found that grade II is the most frequent with 64.3%, followed by grade III with 32.8%, and grade I with 2.9% of cases. These results reflect those of Bangaly Traoré et al. [27] and Mahjoub et al. [28], who also found that SBR grade II takes first place followed by grade III and grade II, respectively.
The histological type of BC can easily be detected in clinical practice. It has been shown to be an important indicator of prognosis [29]. The most common form of invasive carcinoma, called “invasive carcinoma of no special type (NST)”, does not fit into any other category and accounts for 80% of BC [30]. Ben Hammouda et al. [31] and Djounidi et al. [32] found that NST presents 82.5% and 88.87% of cases, respectively. We also found that NST occupies the first place with 81.3% of cases; our results are in line with the previous literature data.
The World Health Organization and other learned societies recommend determination of hormone receptor status and HER2 oncoprotein status at the tumour cell level by IHC as predictive and prognostic markers for BC [31]. The determination of ER, PR, and HER2 protein expression allows tumours to be classified as luminal A, luminal B, HER2+, and TN [33]. The immunohistochemical study shows that subtype luminal B is the most frequent, followed by TN, luminal A, luminal, and HER2+ (35.4%, 32.3%, 26.2%, 4.6%, and 1.5%, respectively). Our results agree with a study performed in Morocco by El Fouhi et al. [34], which also found that luminal B is the most frequent phenotype followed by triple-negative, luminal A, and finally HER2+. IL-6 is a pleiotropic cytokine that plays an important role in various aspects of tumour behaviour, including apoptosis, tumour growth cell proliferation, migration and invasion, angiogenesis, and metastasis [35]. Indeed, the prognostic significance of the expression of these cytokines in BC has not yet been studied in a large cohort of patient samples [10]. Our results are consistent with the literature data. In fact, a meta-analysis performed by Lin et al. [36] showed that IL-6 expression in BC was not correlated with histological grade SBR. Another study conducted at the National Centre Hospital in Korea showed no association between serum IL-6 level and SBR grade [37].
Several studies found that serum IL-6 levels are high in BC compared to control subjects [38–40]. Other studies have reported that IL-6 expression predicts a better prognosis of BC, and their expression is associated with earlier stages [10, 12]. In the present study, we observed no statistically significant difference of serum IL-6 levels between BC patients and controls. According to Benoy et al. [40] the median serum IL-6 levels were almost 10 times higher in patients with metastatic BC than in those with locoregional BC. Patients with 2 or more metastatic sites had higher IL-6 values than those with a single metastatic site [41]. Further studies are needed to clarify the different functions of IL-6 at each stage of BC and the variation in their effects in metastatic and locoregional BC.
Any factor associated with the number of positive lymph nodes is likely to be associated with survival and is a significant prognostic factor in BC [42]. One of the main findings of the present study is the negative correlation between IL-6 expression and lymph nodes. IL-6 was found to be a positive prognostic factor for overall survival and disease-free survival, and its expression was strongly associated with early-stage tumours [12]. A study performed in 2018 revealed that high levels of IL-6 suggest a good prognosis in early-stage invasive BC [10]. Accor-ding to the traditional American Joint Committee on Cancer, N-stage is based on the number of positive lymph nodes and is considered to be one of the most powerful prognostic factors for BC [43]. Furthermore, IL-6 has been demonstrated to be produced by dendritic cells (DCs) in lymph nodes, where it impacts on T cell activation, expansion, survival and polarisation by mobilising anti-tumour T cell responses [44, 45]. Wang et al. [46] report that intact IL-6 signaling in T cells is important for controlling cancer progression and that IL-6 signaling in peripheral blood T cells at diagnosis is considered as a predictive biomarker for clinical result in BC. Vecchi et al. [47] found that IL-6 expression was lower in BC samples classified as N1 and N2 and high in N0 samples.
According to the literature, the IL-6 findings are a good prognosis in early-stage invasive BC, probably by its effect on the number of positive lymph nodes, which is considered as one of the most powerful prognostic factors for BC.
A number of studies indicate that the expression of certain cytokines is influenced by age [48]. A study in the USA found that IL-6 production does not increase with age [49]. Also, Cai et al. [50] and Salgado et al. [41] reported that serum IL-6 levels were not significantly related to age. The results of our study showed that there was no significant difference of IL-6 in different age groups. This result is in agreement with the previous literature data showing that age does not influence IL-6 expression.
Each tumour subtype can communicate differentially with the immune system and produce a specific cytokine profile [15, 51], which may have different effects on tumour progression [37]. Vecchi et al. [47] showed that IL-6 expression is elevated in triple-negative BC (TNBC), and weakly and moderately expressed in the other subtypes (luminal A, luminal B, and HER2+). Another in vitro study by Pe et al. [52] shows that IL-6 levels are significantly elevated in TNBC tissue compared to non-TNBC tissue. Our results are in line with previous studies showing that IL-6 expression is higher in the triple-negative subtype compared to the other molecular subtypes, but no significant difference of IL-6 was observed in the different molecular subtypes. According to our results and those of the literature, the expression of IL-6 differs depending on the BC subtype, but extensive studies are required to elucidate the precise roles of IL-6 in each BC subtype.
Production of ROS is a physiological phenomenon. The disequilibrium in this phenomenon is called oxidative stress, which is involved in the aetiology of several pathologies such as cancer by accelerating the lipid peroxidation of polyunsaturated fatty acids in the cell membrane, leading to the production of toxic substances such as 4-HNE [8, 53]. 4-HNE has been demonstrated to play an important role in cell signal transduction, while increasing cell growth and differentiation, with elevated levels found in invasive human BC. In physiological situations, 4-HNE is present at low levels, but with high concentrations it can become cytotoxic and mutagenic [54, 55].
Our study found a significant difference between 4-HNE serum levels of BC patients and controls. These results mirror those of Sharma et al. [56], who found that high levels of 4-HNE were observed in BC. AL-Musawi et al. [57] demonstrated that high lipid peroxidation is an important risk factor for BC. Another study conducted in Finland by Karihtala et al. [58] showed that 4-HNE is a marker of lipid peroxidation, which increases during breast carcinogenesis, suggesting a role of oxidative stress in the pathogenesis of BC.
Many scientific articles have been published since 1956 on the theory of ageing by free radicals, confirming or refuting this theory [59]. In the present study there was no statistical difference between serum 4-HNE concentrations in the different age groups. According to Câmara et al. [60] age does not influence lipid peroxidation. Kozakie- wicz et al. [59] also found no age-dependent change in malondialdehyde (MDA) levels (markers of lipid peroxidation) during aging. Our results corroborate with data from the literature, in which age does not impact lipid peroxidation. As a result, numerous researchers have focused on the broader concept that multiple forms of damage are causative factors in the ageing process, with ROS as one of the main causes, but not the only one [61].
There are not many studies comparing serum levels of 4-HNE or other markers of lipid peroxidation in different subtypes of BC. Our results showed no significant difference between serum 4-HNE levels in the different molecular subtypes. Antioxidants are a wide range of compounds that can protect lipids from oxidation [62]. Zhang et al. [7] showed that there was no statistical difference between the BC subtypes and systematic oxidative stress (based on 5 biomarkers of systematic oxidative stress). Another study by Bel’skaya et al. [63] found that there was no statistical difference of antioxidant activity in the different BC subtypes. According to previous literature, our results suggest that the anti-oxidative capacity is equivalent in different BC subtypes. However, further studies are needed to understand the role of oxidative stress and antioxidant capacity in each molecular subtype of BC.
There was no correlation between serum 4-HNE levels and SBR grade of tumours. This finding corroborates the work of Karihtala et al. [58], who found that 4-HNE was not associated with SBR grade. Another study conducted by Tas et al. [64] also showed no correlation between lipid peroxidation and histological grade. Indeed, our results suggest that lipid peroxidation was independent of tumour SBR grade.
Lymph node metastasis is an important predictor of disease survival, and it is affected by several cellular and molecular events, notably oxidative stress [65]. A study conducted in Brazil demonstrated that the assessment of lipid peroxidation profiles shows no difference with lymph node status [9]. Carioca et al. [65] showed that there is no association between oxidative stress parameters and lymph node status. Tas et al. [64] also showed that there was no correlation between lipid peroxidation marker MDA and axillary nodes. Our results agree with previous studies, according to which the number and status of lymph nodes are not correlated with the lipid peroxidation marker 4-HNE. These results suggest that oxidative stress does not influence the number and status of lymph nodes, and probably other factors and molecules are involved. Further studies are needed to understand the molecular mechanisms and molecules involved in lymph node metastasis.
Hypoxia is a common feature associated with many types of cancer, and it is an ever-present condition in the tumour environment due to the rapid growth of tumour cells that are not supported by an adequate blood supply. This state may impact on the production of HIF-1α, a transcription factor implicated in carcinogenesis, tumour growth, and other biological mechanisms [66, 67]. In BC, hypoxia is known to play a crucial role in cancer progression and cancer treatment failure [68].
The results obtained in the current study show there was no statistically significant difference in serum HIF-1α levels between controls and patients.
No significant difference was found between HIF-1α serum levels in different molecular subtypes of BC. This finding supports the study of Gunawan et al. [14], who found that the levels of HIF-1α mRNA and soluble HIF-1α protein in tissues and blood were similar in different molecular subtypes, and that no association was found. Our results also agree with the findings of Nie et al. [69], who reported that there is no significant difference of HIF-1α in the different molecular subtypes.
Detecting significant age-related changes would contribute to understanding how the response to hypoxia changes with age and may provide important information on how to predict hypoxia-induced diseases. However, it is not known if the expression of HIF-1α changes with age [70]. Several studies have noted that there is no correlation or association between HIF-1α expression and age [69, 71, 72]. Our results corroborate with previous studies that there is no significant association between HIF-1α serum levels in different age groups. These results indicate that the concentration of HIF-1α is not influenced by age.
HIF-1α expression has been reported to be associated with lymphatic metastasis in various types of cancer, but the underlying mechanism has not yet been well established [73]. We noted that there was no correlation between serum HIF-1α levels and the number of lymph nodes. Similar results have been obtained in other studies [13, 74, 75]. Our results suggest that HIF-1α is not a marker of lymph node metastasis in BC.
No significant correlation was noted between the expression of HIF-1α and SBR tumour grade. This result concurs with the findings of Cai et al. [71] and Li et al. [72].
Conclusions
Our results showed high levels of 4-HNE, a marker of lipid peroxidation, in our BC patients, indicating the presence of oxidative stress; this imbalance between the production of ROS and antioxidants has been implicated in several diseases such as cancer, including BC.
IL-6 was found to be negatively correlated with lymph node count, which is one of the strongest prognostic factors for BC, suggesting that IL-6 is a good prognostic factor.
However, there was no association between 4-HNE, HIF-1α, and the number of lymph nodes.
In addition, our results show that serum levels of 4-HNE, IL6, and HIF-1α were independent of tumour SBR grade as well as age, and that BC molecular subtypes do not influence their levels.
In the future we plan to analyse the mutational spectrum of the P53 tumour suppressor gene by analysing specific hotspots altered under the effects of oxidative stress, and to study the polymorphism of antioxidant enzymes such as superoxide dismutase, catalase, and glutathione peroxidase.