









Introduction
Menopause is the period when the reproductive capacity ceases in women’s life. During this transition, a wide range of symptoms occur as a consequence of estrogen decrease. The age and symptomatology of menopause vary across the world. Evidence suggests that there is a difference in the prevalence of symptoms among Asian and Western women. Most of the women are unmindful about menopausal symptoms and their health effects. Symptoms of menopause can be extreme and affect the day-to-day life of some women [1]. The climacteric changes happen for several years, approximately 5–8 years [2].
Menopausal status was defined on the basis of menopausal symptoms and the regularity of menstrual cycles. Women with regular menstrual bleeding with menopausal symptoms during the last year were classified as pre-menopause, those with irregular bleeding during the last 12 months as peri-menopause, and those with cessation of menstrual bleeding from 1 year and above were classified as post-menopause [3].
Worldwide, the age range of natural menopause is 45–55 years. The average age of menopause of an Indian woman is 46.2 years, whereas it is 51 years for the Western population [4]. Education, occupation, socio-economic status, marital status, parity, mode of delivery, age and body mass index (BMI) are the factors related to one or more menopausal symptoms [5].
Evidence indicates that the midlife crisis of women is related to an increase in body weight. Central fat and intra-abdominal fat increase during menopause [6]. Obese women scored significantly higher on menopausal physical symptoms. Maintaining normal anthropometric indices might improve the quality of life (QoL) in menopausal women [7].
Most symptoms experienced during menopause are self-limiting and not life-threatening but are nonetheless unpleasant and sometimes disabling. Menopausal symptoms are related to deterioration in physical, mental, sexual health and lowered QoL [8]. The information regarding postmenopausal QoL has often been neglected over the years, especially in India [9]. Due to lack of awareness the majority of women do not seek medical treatment for menopausal symptoms which affect their physical and mental health [10].
Lifestyle modifications such as adhering to structured exercise and physical activity (PA) can decrease vasomotor menopausal symptoms. Physical activity has a positive influence on improving psychological function and the overall QoL of menopausal women. On the whole, exercise has a lot of beneficial effects on menopause [2].
Marlatt et al. stated that considering the opinions of menopausal women, a lifestyle modification program targeting weight loss or weight maintenance is warranted to reduce metabolic impairments and symptoms during the menopause transition and is considered as a potential alternative to hormone replacement therapy [11].
Studying the symptomatology and menopause- related health problems gives us an insight into the unmet needs of middle-aged women and helps us to supply focused service. Creating awareness about menopausal symptoms and improving the QoL of menopausal women would improve the community health.
This study primarily aimed to analyze the association between menopausal symptoms, PA level, anthropometric measurements and QoL among south Indian menopausal women.
Material and methods
A cross-sectional observational study was conducted among south-Indian menopausal women, aged 45–65 years. Participants were recruited through online platforms such as WhatsApp and Facebook and by e-mail. The data were collected through Google Forms with 5 sections during the period April 2021 to June 2021. Section 1 contained the consent form, which detailed the study process and participant’s consent. Section 2 collected the data on the participant’s characteristics which included personal, obstetric and gynecological history. The third section contained the Menopause Rating Scale (MRS) questionnaire, which had 11 questions, depending on the severity; each symptom was scored 0–4, with 0 being none and 4 being extremely severe. The fourth section contained the Menopause-Specific Quality of Life Questionnaire (MENQOL). It consists of 29 items with four domains: vasomotor, psychosocial, physical and sexual (Cronbach’s α 0.86) [12]. The final section contained the International Physical Activity Questionnaire (Cronbach’s α 0.63–0.85), a self-reported questionnaire used worldwide which assesses the general PA over the last seven days [13]. The level of PA was categorized as low, moderate or vigorous. The participants were required to complete all the sections. In all, 168 responses were received. Based on the inclusion and exclusion criteria the received responses were segregated. Finally, 153 responses were included in the study.
Exclusion criteria
Women who had experienced menopause due to medical conditions such as hysterectomy, oophorectomy, radiation or chemotherapy. Women with mental illness and chronic disease.
Statistical analysis
The collected data were statistically analyzed through SPSS version 24.0. To describe the data, descriptive statistics and percentage analysis were used for categorical variables. The associations of variables such as PA, menopausal symptoms and QoL were analyzed using the χ2 test.
Results
The age range of the participants in this study was 45–65 years (Table 1). Baseline characteristics of the study participants are presented in Table 2. The majority of the women were homemakers (71.8%). 68.6% did not have any co-morbidities. 13.7% had regular exercise habits. On the whole, women were found to have the following symptoms: joint and muscular discomfort (80.4%), irritability (72.5%), depressive mood (68%), sleep discomfort (60.8%), anxiety (67.3%), hot flush (53.6%), physical and mental exhaustion (50.3%), bladder problems (32.7%), heart discomfort (31.4%) vaginal dryness (25.5%) and sexual problems (11.8%) (Fig. 1). A significant difference was found among the groups of varied PA in physical and sexual domains of MENQOL (p-value ≤ 0.05) (Table 3). A statistically significant difference was observed between BMI and MRS menopausal symptoms among the participants in the variables such as irritability and depressive mood (p-value ≤ 0.05) (Table 4).
Table 1
Demographic characteristics
| Menstrual cycle, N = 153 | Age | BMI |
|---|---|---|
| Pre-menopause, n = 61 | 48.52 ±3.18 | 26.75 ±6.68 |
| Peri-menopause, n = 36 | 48.92 ±3.41 | 27.92 ±4.05 |
| Post-menopause, n = 56 | 52.73 ±4.91 | 27.18 ±5.44 |
Table 2
Characteristics (life style, education, health and menopausal status) of participants
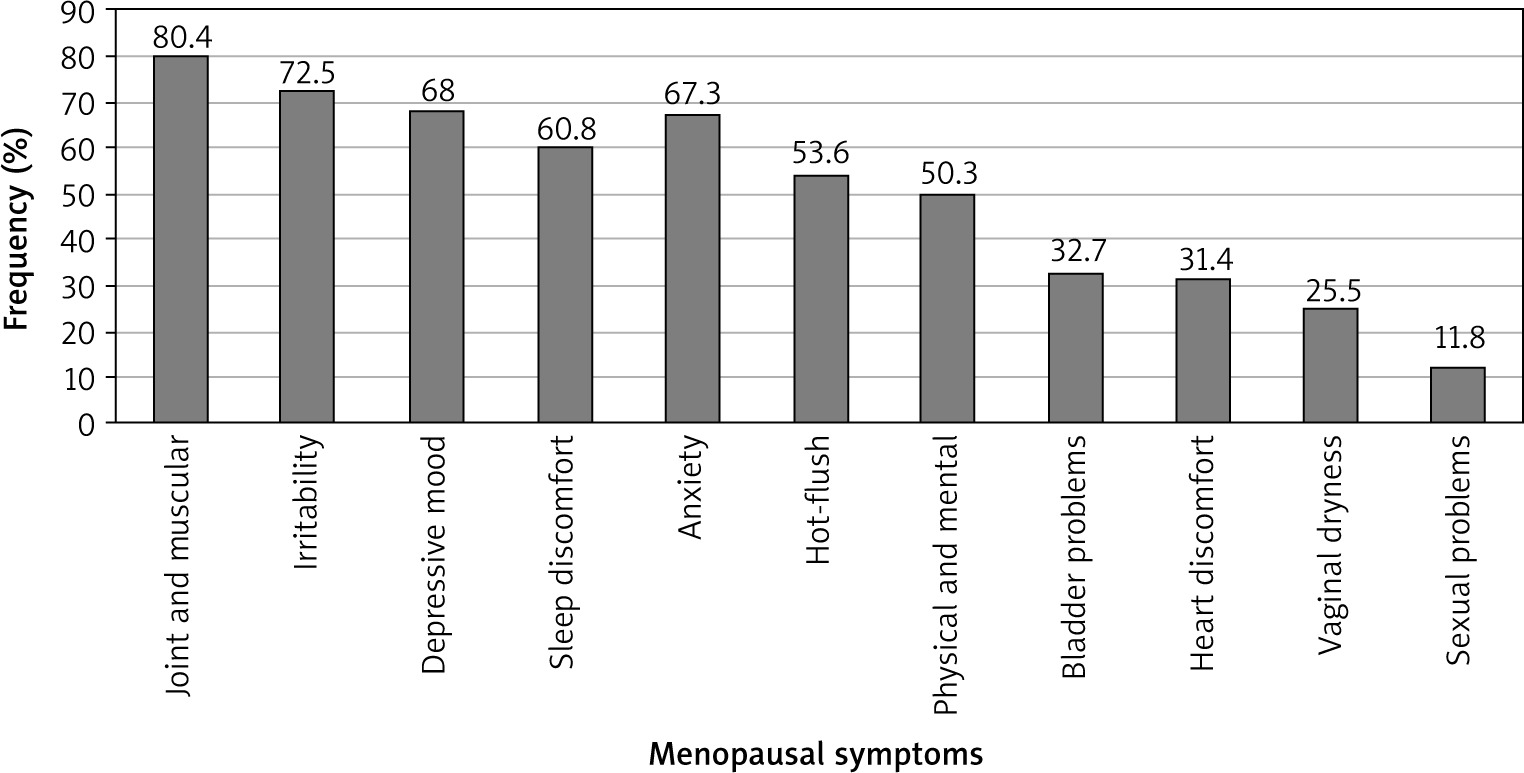
Table 3
Physical activity and Menopause-Specific Quality of Life Questionnaire domains among participants
Table 4
Menopausal symptoms and body mass index
Discussion
Management of vaginal bleeding in advanced cervical cancer
To our knowledge, this is one of the few studies which has investigated the relationship between PA, anthropometric measurements, QoL and menopausal symptoms.
In the present study 91.5% of women had one or more symptoms. Similarly, Waidyasekera et al. (2008) in Sri Lanka found that the prevalence of any bodily symptom during the post-menopausal period was 90% [14]. The majority of participants in this study were homemakers and graduates. A study by Nadia et al. (2015) showed that a low literacy rate was associated with more psychological stress and with high risk for vasomotor symptoms. Similarly, in a study conducted by Alquiz et al. (2004), women with higher education had fewer vasomotor symptoms [15]. A cross-sectional study by Madhukumar et al. (2017) revealed that occupation and marital status had a significant impact on the health of post-menopausal women and homemakers experienced more vasomotor symptoms [5].
Menopausal symptoms such as sleep discomfort, depressive mood, irritability, physical and mental exhaustion, bladder problems, dryness of the vagina, and joint and muscular discomfort were the common complaints observed in this study. Khatoon et al. (2018) reported that joint and muscular discomfort, depressive mood, and physical and mental exhaustion were the chief complaints of the menopausal women. Secondly, hot flushes, sleep problem, irritability and anxiety were reported. Urogenital symptoms such as bladder problems, dryness of the vagina and sexual problems were found to be less prevalent, which was similar to the findings of this study [16]. On the whole, joint and muscular discomfort (80.4%), irritability (72.5%), depressive mood (68%), sleep discomfort (60.8%), anxiety (67.3%), hot flushes (53.6%), physical and mental exhaustion (50.3%), bladder problems (32.7%), heart discomfort (31.4%), vaginal dryness (25.5%), and sexual problems (11.8%) were experienced by the menopausal women (Fig. 1).
The analysis of PA and MENQOL showed a significant difference between PA level and physical and sexual domains of MENQOL. Women with moderate PA had fewer menopausal symptoms than the lower and vigorous PA group (Table 3). Kim et al. mentioned that a moderate level of PA was associated with reduced psychosocial and physical symptoms but not with changes in vasomotor and sexual symptoms [17]. Evidence supports that moderate PA reduces menopausal symptoms. Morgan, 1985, and Takenaka, 1998, stated that exercise could reduce symptoms such as depression and anxiety. Physical activity brings more relief for general physical and mental issues including sleep quality, psychological distress and weight gain. Depressive symptoms decreased with high and moderate PA compared to low PA level. Physical activity promotes higher QoL both in middle-aged women and during menopause [18].
Women who were obese reported higher vasomotor symptom scores than women of normal weight and women who were overweight reported lower health- related QoL scores than women of normal weight [3]. There was a significant association between BMI and menopausal symptoms such as depressive mood and irritability (p = 0.001 and 0.019) in the present study. Engaging in PA is essential for weight reduction in obese and overweight categories since PA is a vital part of health promotion across various age group (Table 4).
Elavsky et al. (2009) stated that increasing PA may enhance menopause-related QoL. When designing PA interventions, researchers and practitioners should include strategies to identify women’s physical self- perceptions and plan for optimal symptom management to improve QoL [19]. Physical activity has been shown to reinforce the QoL among menopausal women, probably due to its action on neuroendocrine balance and the release of endogenous opioids, which leads to decreased vasomotor symptoms. Moreover, PA enhances psychosomatic well-being by improving self-esteem and quality of sleep and decreasing musculoskeletal pain and menopausal complaints [16]. Evidence suggests that a moderate amount of PA should be recommended for menopausal women to have a good QoL [17, 18]. In the present study, there was a decrease in the physical and sexual symptoms in women with moderate PA. Physical activity has numerous health benefits, has no side-effects and is safe to practice at any age. Moreover, moderate PA promotion among menopausal women would benefit overall well-being and improved QoL.
However, the results cannot be generalized as the sample size proportion is varied for the PA level and the menopausal category. Sample size and detailed anthropometric measurements including waist-hip ratio and skinfold measurements are the limitations of this study. Due to COVID, data collection was performed online.
Future studies can be done with a larger sample size with objective measurements as outcome measures. Further studies based on levels of PA, practicing or adherence to exercises and their impact on menopausal symptoms can be done, which may be useful for physiotherapists to develop an appropriate exercise protocol for menopausal women.
Clinical implication
The clinical implication is that there are a lot of health benefits over all age groups. Women’s PA decreases as age increases. Inclusion of PA as a lifestyle modification among peri- and post-menopausal women results in better QoL. Appropriate PA quantification and exercise prescription based on individual variation are recommended.