








Introduction
Hilar cholangiocarcinoma (HC) is the leading cause of hilar biliary obstruction [1–3]. When patients with HC experience jaundice and related symptoms, their disease is generally inoperable, and their prognosis and expected overall survival (OS) are relatively poor [4]. Biliary stent insertion is often conducted in inoperable HC patients as it can provide rapid relief of jaundice while allowing patients to undergo radiotherapy or chemotherapy to prolong their survival [4].
Bilateral stent insertion in patients suffering from hilar biliary obstruction has been established by the Asia-Pacific consensus criteria and a series of meta-analyses as superior to unilateral stent insertion concerning both rates of clinical success and the duration of stent patency [5–8]. Bilateral stenting is associated with lower re-stenosis rates of 7–12% compared to unilateral stenting [7, 8]. As these bilateral stents lack intrinsic antitumor properties, they fail to extend the OS of treated patients [6–8]. Undergoing external radiotherapy or systemic chemotherapy, while common treatments for individuals with HC, can result in particularly severe toxic treatment-related effects [4].
Given the above challenges, researchers and clinicians have increasingly explored the deployment of radioactive stent systems consisting of a metal stent and a strand of 125I seeds to protect patients with HC against re-stenosis and thereby extend their survival [4]. In this method, a radioactive stent is implanted at the obstruction site so that the 125I seeds are fixed between the tumor and the inserted stent, enabling the delivery of persistent, localized radiotherapeutic treatment [4]. Critically, these 125I seeds can simultaneously deliver a high radiation level to the tumor while mainly avoiding the irradiation of surrounding healthy tissue [4]. A few reports have assessed the relative clinical efficacy of traditional and radioactive stent insertion procedures in patients with HC [9–11], but prospective studies on this topic are lacking.
Aim
The present study was designed as a prospective randomized controlled trial (RCT) to compare the clinical outcomes of inoperable HC patients following the insertion of either a normal or a radioactive stent.
Material and methods
Study design
The Ethics Committee of Xuzhou Central Hospital approved this open-label, prospective RCT, with all enrolled patients have provided written informed consent. This trial has been registered at https://clinicaltrials.gov/, No. NCT04779788.
Between April 2021 and March 2022, 90 patients with HC were randomly assigned to either a normal or a radioactive stent insertion group (n = 45/group). Patient baseline data are summarized in Table I, while a flowchart of the study process is provided in Figure 1. To be eligible for inclusion, patients had to: (1) have a definitive diagnosis of HC, (2) have inoperable HC, and (3) exhibit symptoms consistent with obstructive jaundice. Patients were excluded if they (1) had Bismuth I type IC, (2) had undergone perioperative external radiotherapy, (3) had any prior history of biliary stent insertion or drainage, (4) had any history of prior hepatolobectomy, (5) exhibited an Eastern Cooperative Oncology Group (ECOG) performance status (PS) ≥ 4, or (f) were unable to provide informed consent.
Table I
Baseline data of enrolled patients

The definitive diagnosis of HC was established based on the results of intraductal biopsy analyses. Bismuth type determinations were made based on the results of abdominal computed tomography (CT) and magnetic resonance imaging (MRI) scans. The inoperable criteria were as follows: (a) extensive infiltration to the adjacent tissues; (b) distant metastasis; and (c) poor physical condition [12].
Randomization
Patients were randomized to normal and radioactive stent groups at a 1 : 1 ratio via block randomization with a block size of four. Random numbers were generated with a computer and placed in sealed, opaque, sequentially numbered envelopes. Before stent insertion, a member of the Science and Education Department with no other role in this RCT opened the randomly assigned envelopes.
Stents
Self-expanded metal stents (Micro-Tech, Nanjing, China) that were 8 mm in diameter and 50–70 mm long were used for stent insertion in all patients. Radioactive stenting was performed by combining these stents with a 125I seed strand prepared by sealing 125I seeds (Chinese Atomic Energy Science Institution, Beijing, China) within a 4F catheter (PBN MEDICALS Denmark A/S, Stenlose, Denmark). Individual seeds were 0.8 mm in diameter and 4.5 mm long, and released low-energy 35.5-keV γ-rays with a 59.6-day half-life. The number of seeds was selected based on the obstruction length: N = length of stent (mm)/4.5 + 4 [11].
Normal stent insertion
A side-by-side percutaneous approach was used for the insertion of bilateral stents. Following the simultaneous puncture of the left and right intrahepatic biliary tracts, two VER catheters were introduced via a 0.035-inch Radifocus guide wire (Terumo, Tokyo, Japan) to detect the obstruction. After the catheters had reached the obstruction and entered the duodenum, stiff guide wires (Cook, IN, USA) were used to replace the Radifocus guide wires. Two delivery systems were then introduced with the stiff guidewires to the site of the obstruction and simultaneously released in a Y shape (Photo 1 A).

Radioactive stent insertion
A side-by-side percutaneous approach was used for the insertion of bilateral radioactive stents. Briefly, two stiff guidewires were initially introduced, with two additional guidewires being used to pass two 6F sheaths across the obstructed sites. Stents were placed at the center of the obstructed site with a 0.035-inch stiff guidewire. Then, 125I seed strands were placed within 6F sheaths; with these sheaths removed the seed strands were positioned between the stent and the biliary wall. These two stents were positioned in a Y shape (Photo 1 B).
Follow-up
Patients were followed for 2 weeks, 1, 3, and 6 months, and every 6 months after that until death or September 30, 2022. Blood tests, physical examinations, and abdominal CT scans were part of the follow-up examinations.
Definitions
Technical success for stent insertion procedures was defined by the release of stents precisely at the site of the obstruction so that the contrast medium could smoothly pass through the stent [12]. Clinical success was defined by a ≥ 30% reduction in total bilirubin (TBIL) levels within 2 weeks following stent placement [12]. Stent patency was defined by the period from stent insertion to jaundice recurrence [12]. When patients died without evidence of re-stenosis, stent patency and OS were identical, and results were not censored. OS was the period from stent insertion to all-cause death. Early and late postoperative complications were defined based on whether they occurred less than or more than 30 days after stenting.
Statistical analysis
The primary endpoint of this study was stent patency. When we registered this study, the primary endpoint was OS. However, we read many studies regarding biliary radioactive stent insertion and found that the primary function of biliary radioactive stent was reducing the re-stenosis rate [4, 11]. Therefore, we changed the primary endpoint to stent patency. According to results of a prior study comparing normal and radioactive stenting in malignant hilar biliary obstruction patients [13], a 30% higher 6-month stent patency rate was expected following radioactive stenting as compared to normal stenting (85% vs. 55%). Accordingly, power calculations indicated that a minimum of 76 patients (38 patients in each group) were necessary with a power of 0.8 and an α of 0.05 when taking a dropout rate of 10% into consideration.
This study was conducted using intention-to-treat (ITT) and per-protocol (PP) analytical approaches, with the former being conducted based on the total number of enrolled patients and the latter being based on the number of patients in whom stent insertion procedures were technically successful. ITT analyses were employed when assessing baseline data and rates of technical success, whereas rates of clinical success, stent patency, OS, and complications were compared via PP analyses.
Continuous data are given as medians or means ± standard deviation and were compared via the Mann-Whitney U test or t-test. Categorical data were compared with the χ2 test or Fisher’s exact test. Kaplan-Meier curves and log-rank tests were used to compare OS and stent patency. Predictors of OS and stent patency were assessed through Cox regression analyses, with those variables exhibiting p < 0.1 in univariate analyses being included in a multivariate analysis. P < 0.05 served as the significance threshold, and SPSS 16.0 (SPSS Inc., IL, USA) was used for all statistical testing.
Results
Technical success rates
A total of 5 patients in the normal stent group did not undergo bilateral stenting, 2 underwent unilateral stenting, and 3 underwent an extra-biliary drainage catheter placement. After drainage for 1 week, stent insertion was again attempted in these patients but without technical success. Similarly, bilateral stent insertion failed in 5 radioactive stent patients, of whom 3 and 2 underwent unilateral stenting and extra-biliary drainage catheter placement, respectively. Following drainage for 1 week, stent insertion was again attempted, without technical success. Thus, the respective technical success rates in the normal and radioactive stent insertion groups were 93.3% and 97.9% (p = 1.000, Table II).
Table II
Treatment effectiveness
Clinical success
Similar clinical success rates were seen in patients who underwent normal and radioactive stenting (95.3% vs. 97.7%, p = 0.983, Table II). The TBIL, aspartate transaminase (AST), and alanine aminotransferase (ALT) levels of patients in the normal stenting group declined from pre-stenting values of 210.2 ±89.3 µmol/l, 138.3 ±81.4 U/l, and 158.5 ±137.4 U/l, respectively, to 116.8 ±77.9 µmol/l (p < 0.001), 62.5 ±41.7 U/l (p < 0.001), and 62.2 ±40.0 U/l (p < 0.001) following stent placement. Similarly, the TBIL, AST, and ALT values of individuals who underwent radioactive stent insertion declined from 215.6 ±118.6 µmol/l, 163.1 ±128.4 U/l, and 155.2 ±120.1 U/l prior to stenting to 99.2 ±53.7 µmol/l (p < 0.001), 65.6 ±37.1 U/l (p < 0.001), and 64.6 ±43.0 U/l (p < 0.001) following stent placement.
Stent patency
Similar re-stenosis rates were found in the normal and radioactive stent insertion groups (26.2% vs. 23.2%, p = 0.754, Table II). All patients in the normal stenting group who experienced r-stenosis were treated via biliary drainage catheter placement, while 9/10 patients with re-stenosis in the radioactive stent group also underwent biliary drainage catheter placement. The remaining patient had originally undergone unilateral radioactive stent insertion and was therefore treated by placing a second stent from the contralateral intrahepatic biliary tract.
Radioactive stent insertion was associated with significant prolongation of stent patency relative to the normal stent group (195 days vs. 115 days, p < 0.001, Figure 2 A). Cox regression analyses revealed that factors related to increased stent patency included Bismuth III HC (p = 0.027) and radioactive stent use (p = 0.018) (Table III).
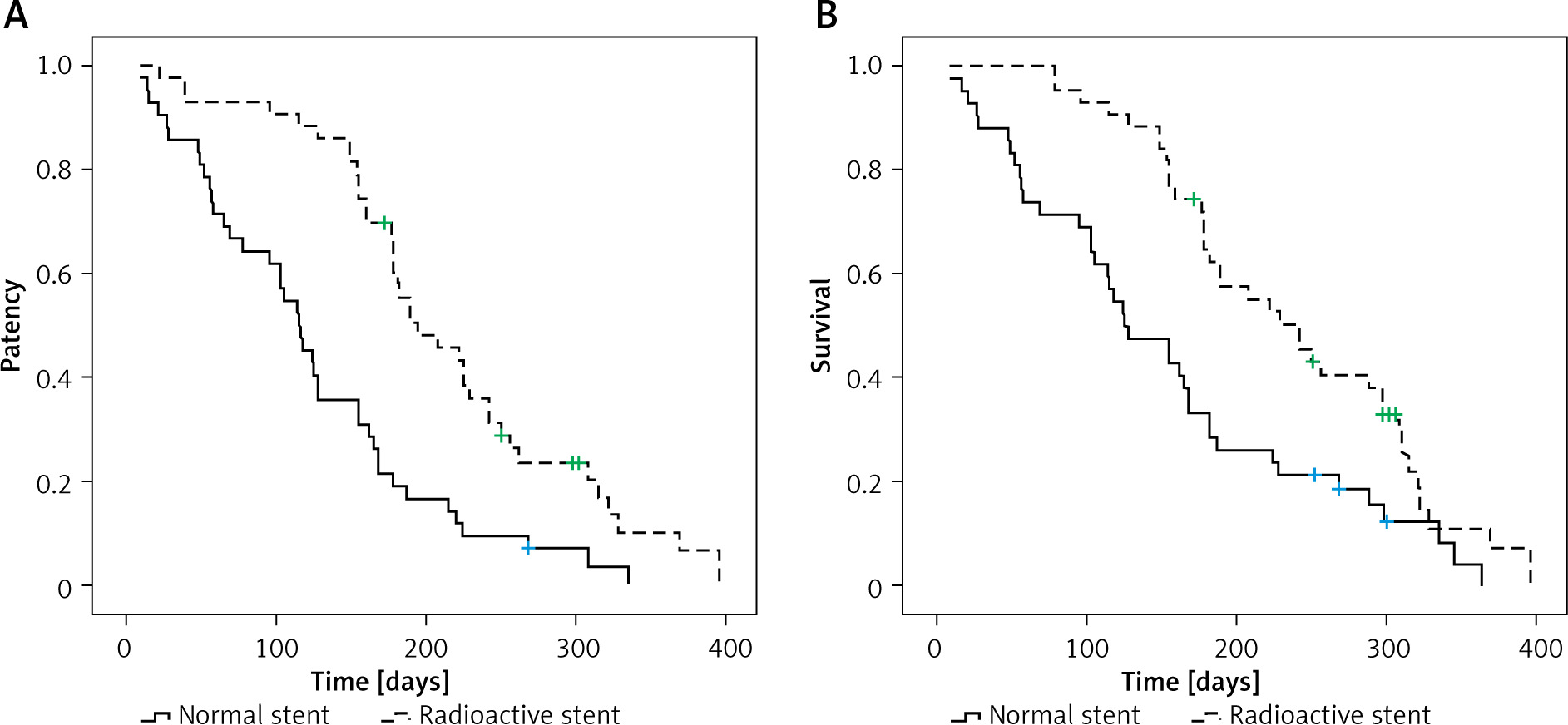
Table III
Predictors of stent patency
OS
Following stent placement, a transarterial chemo-infusion was conducted in 14 and 12 patients in the normal and radioactive groups. Postoperative chemotherapeutic treatment was based on each patient’s condition and approval. During the follow-up period, 39 and 37 patients in these two groups died, with 65 patients succumbing to tumor progression, 8 to severe abdominal infection, and 3 to acute renal failure.
Individuals who underwent radioactive stent insertion survived significantly longer than those who underwent normal stenting (242 days vs. 125 days, p = 0.002, Figure 2 B). Higher ECOG PS (p = 0.043), post-operative TBIL (p = 0.014), radioactive stent use (p < 0.001), and postoperative chemotherapy use (p = 0.003) were all associated with longer OS according to Cox regression analyses (Table IV).
Table IV
Predictors of overall survival
Postoperative complications
Of the patients in the normal stent group, early and late postoperative complications developed in 6 (14.3%) and 5 (11.9%) patients, respectively, with these complications including cholangitis (n = 7) and cholecystitis (n = 4). Similarly, 7 (16.3%) and 8 (18.6%) radioactive stent group patients, respectively, experienced early and late postoperative complications, including cholangitis (n = 8), cholecystitis (n = 6), and self-limited biliary bleeding (n = 1). Complication rates in these groups were not significantly different (Table V).
Table V
Post-operative complications
The 15 cases of cholangitis were managed through medical treatment (n = 10) or percutaneous catheter drainage (n = 5), with medical treatment (n = 8) or percutaneous catheter drainage (n = 2) also being used for the treatment of the 10 cases of cholecystitis.
Discussion
The present RCT was performed to examine the relative safety and efficacy of traditional and radioactive stenting in patients with HC. These two groups’ overall technical and clinical success rates were similar, suggesting that these stenting strategies are well-suited to provide rapid jaundice relief in individuals with HC. The technical (97.9%) and clinical (97.7%) success rates for individuals who underwent radioactive stenting in this study were also similar to those in prior reports focused on radioactive stent placement in patients with HC [3, 10, 13].
A percutaneous stent insertion approach may explain the high technical and clinical success rates. While endoscopic approaches are often used by groups inserting stents to treat distal biliary obstructions [14–16], the percutaneous approach is more appropriate in cases of hilar biliary obstruction [17, 18], improving respective technical and clinical success rates by 17.6% and 15.4% as compared to the endoscopic approach [17, 18].
Stent re-stenosis often results from tumor growth, sludge formation, and the proliferation of biliary epithelial cells [14–16], with stent re-stenosis as the most common cause [19]. Antitumor treatments are thus the most effective option for minimizing rates of re-stenosis. Since radioactive stenting allows for the simultaneous delivery of brachytherapy and stent dilation [20], it is ideally suited to use in this context. 125I seeds are effective radioactive sources capable of continuously releasing X and γ rays capable of killing tumor cells and slowing tumor growth [10] while surrounding normal tissue received a radioactive dose < 25% of that received by tumor cells [21].
Here, the insertion of radioactive stents did not contribute to any significant reduction in the rate of re-stenosis, although it was associated with significant prolongation of stent patency. Strikingly, radioactive stenting was associated with more prolonged patient OS. Since radioactive stent insertion was predictive of both longer stent patency and OS, and postoperative chemotherapy was also predictive of prolonged OS, chemotherapy may represent a practical option for the simultaneous adjuvant treatment of HC patients undergoing radioactive stent insertion.
Here, bilateral radioactive stent insertion was performed, whereas many prior studies have performed unilateral radioactive stenting in patients with HC [9, 10, 13]. Wang et al. [3] additionally reported comparable rates of technical (100% vs. 100%) and clinical success (100% vs. 100%), stent patency (208 days vs. 222 days), and OS (250 days vs. 246 days) when comparing unilateral and bilateral radioactive stent insertion in patients with HC. These results, however, were derived from a retrospective study [3]. Additional RCTs will thus be essential to test this possibility.
In this study, we found that Bismuth type III HC was another factor for increased stent patency. This finding is unexpected because Bismuth type III HC is more extensive infiltration of the biliary tree than Bismuth type II HC. The possible reason is that post-operative chemotherapy was mainly used for the Bismuth type III and IV patients.
The current findings demonstrated that the use of radioactive stents did not contribute to any incidence of postoperative complications. This is likely because the 125I seed strand has a diameter of only 1.33 mm (4F) and thus is unlikely to exert significant pressure on the biliary tract.
There are some limitations to these analyses. While this was an RCT, patients were not randomized with stratification based on tumor staging or Bismuth type, potentially contributing to selection bias. The open-label nature of this study may have also influenced the risk of bias. However, as different stent types were used for this study, achieving effective blinding was challenging. Third, exact radioactive stent dosimetry could not be calculated as the treatment planning system is unsuitable for lumen-shaped tumors [22]. Finally, using RECIST criteria to assess tumor responses to treatment was challenging given that the stent pressed directly on the tumor, thus limiting efforts to assess the ability of radioactive stent insertion to inhibit the tumor [4].