





Introduction
Chronic skin diseases generally have a complex multifactorial pathogenesis which involves genetic predisposition, environmental factors and immune system hyperactivity [1]. Chronic dermatoses impair health-related quality of life (QoL) in affected patients, having an impact on multiple aspects of psychophysical functioning and patients’ well-being. Sleep is a physiological, fundamental, active process that takes around one-third of humans’ lives. It is regulated by two major processes – homeostatic sleep drive and circadian system [2, 3]. Skin plays an important role in proper sleep activity, which includes control of thermoregulation, core body temperature, sleep onset, and awakenings during sleep.
Impaired sleep quality is associated with systemic diseases, e.g. chronic obstructive pulmonary disease (COPD) [4], obstructive sleep apnea and hypopnea syndrome (OSAHS) [5], heart failure [6, 7], cancers [8–11], lymphoma [12], systemic lupus erythematosus [13, 14], psoriatic arthritis [15] and sarcoidosis [16].
Moreover, chronic dermatoses (commonly pruritic and/or painful) including atopic dermatitis [17], psoriasis [18, 19], chronic spontaneous urticaria [20], prurigo nodularis [21], hidradenitis suppurativa [22], acne vulgaris [23] and lichen planus [24], may also substantially interfere with sleep quality, resulting in deterioration of general well-being.
Nocturnal itch has a complex pathophysiologic mechanism, but still it is unclear. Underlying mechanisms accountable for nocturnal itch include e.g. changing of skin barrier function (increasing of trans-epidermal water loss (TEWL) at night) [25], thermoregulation (e.g. regulation of core body temperature which is maximal early in the evening and minimal early in the morning) [26], circadian rhythms (the hypothalamus-pituitary-adrenal axis is responsible for corticosteroid level regulation; corticosteroid level is minimal during the evening and night, which is reflected in a diminished anti-inflammatory reaction) [27], melatonin (associated with the support of circadian rhythm and the sleep cycle as a regulatory hormone) [28] and disruption of the endogenous molecules involved in physiologic circadian rhythm (prostaglandins (PG) – PGD2 and PGE2, opioids and opioid receptors, nerve growth factor (NGF), interleukins and cytokines – IL-2, IL-8, IL-31, INF-γ) [3, 27].
Nocturnal itch is undoubtedly associated with chronic skin diseases mentioned above (i.e. atopic dermatitis, psoriasis, prurigo nodularis, chronic spontaneous urticaria and lichen planus), but also with lichen simplex chronicus and bullous pemphigoid, conditions with severe symptoms (e.g. erythroderma) [3, 27, 29]. Skin infestations (e.g. bed bugs, scabies, pediculosis, pinworms) may also be accompanied by nocturnal itch [3, 27]. Moreover, Lavery et al. [3] reported non-dermatological conditions associated with nocturnal pruritus, including chronic kidney and liver disease, hematopoietic disorders, substance abuse, neurological (e.g. brachioradial pruritus) and psychological disorders (e.g. depression, schizophrenia, stress, delusional ideation), and restless legs syndrome.
The aim of this study was to review the published studies that have investigated the association between chronic dermatological conditions and sleep quality in adult patients.
Methods used to assess sleep quality
Subjective methods
Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index (PSQI) is a self-reported questionnaire which assesses sleep quality and disturbances over a 4-week time interval. The PSQI is used to evaluate seven domains of sleep quality: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication and daytime dysfunction. The questionnaire uses 14 questions based on a 0–3 scale (where 3 indicates the most negative outcome) and 4 open-ended questions. PSQI scores range from 0 to 21 points. A global score of ≥ 5 is a specific and sensitive indicator of poor sleep quality [30–32].
The Medical Outcomes Study – Sleep Scale
The Medical Outcomes Study Sleep Scale (MOS-SS) is a validated instrument with 12 self-reported questions on multiple facets of sleep quality and quantity within a 4-week period [33–35]. The average MOS-SS score in the general population has been estimated at 25.8. The questionnaire generates seven measures for sleep quality: sleep disturbance, snoring, awakening short of breath or with a headache, sleep adequacy, daytime somnolence, Sleep Problem Index I (SPI I) and Sleep Problem Index II (SPI II) [36]. Each of the 7 sleep-quality scores range from 0 to 100. Greater scores for the six domains indicate worse sleep quality, except for sleep adequacy, for which greater scores indicate better sleep quality [36].
Objective methods
Actigraphy
An actigraph is a small, wrist-worn device that tracks sleep-wake patterns (sleep latency, efficiency, and periods of awakening) by using activity-based monitoring. It has been validated to assess sleep parameters and highly correlates with polysomnography [37]. Actigraphy may be the preferred method of assessing sleep in dermatological patients because it reflects the home environment (can be performed at home), is easy to use, well accepted by patients and cost-effective, and assesses the most commonly affected sleep parameters in patients with AD (e.g. sleep disruption secondary to nocturnal awakenings and scratching) [17, 38].
Polysomnography
Polysomnography (PSG) consists of an electroencephalogram (EEG), an electrooculogram (EOG) and an electromyogram (EMG), which together make up the gold standard of sleep examinations. Using PSG has two major drawbacks – the discomfort of having multiple leads and equipment attached and the necessity to stay overnight at a sleep center [17].
Atopic dermatitis
The mean prevalence of atopic dermatitis (AD) in the general population ranges from 2.1% to 4.9% across countries [39]. The disease is characterized by erythema, lichenified lesions and is accompanied by severe itch, which is an essential symptom of AD. It negatively influences various aspects of AD patients’ well-being [40]. Sleep quality may be significantly disturbed in AD patients. A higher prevalence of sleep disturbance was reported in adults with AD compared to controls [17]. Five reviewed studies used the PSQI questionnaire [37, 41–44] one of which also used actigraphy [42], and one study used actigraphy and polysomnography in addition to PSQI [43]. Two additional studies were based only on actigraphy [38, 45]. The achieved mean PSQI score ranged from 7.0 to 8.5 points across the studies [37, 41, 42, 44] (figure 1), and was significantly higher compared to controls (p< 0.01) [42, 44]. Moreover, PSQI scores significantly correlated with QoL assessed by the Dermatology Life Quality Index (DLQI) [37, 41] and AD severity [41]. Bender et al. [42] established a significant influence on subjective sleep quality and daytime dysfunction domains. Nonetheless, a significant impact of all domains of the PSQI among AD patients was also reported [44]. Moreover, the study by Bender et al. [43] revealed moderately strong correlations between actigraphy score and both PSG scores (sleep efficiency, sleep latency) and the scratching index. Increased itch and scratching during the night [38] seem to play a significant role as factors negatively affecting patients’ sleep. Yano et al. [41] suggested that mood problems may also impair the quality of sleep. Detailed data are shown in Table 1 [37, 38, 41–45].
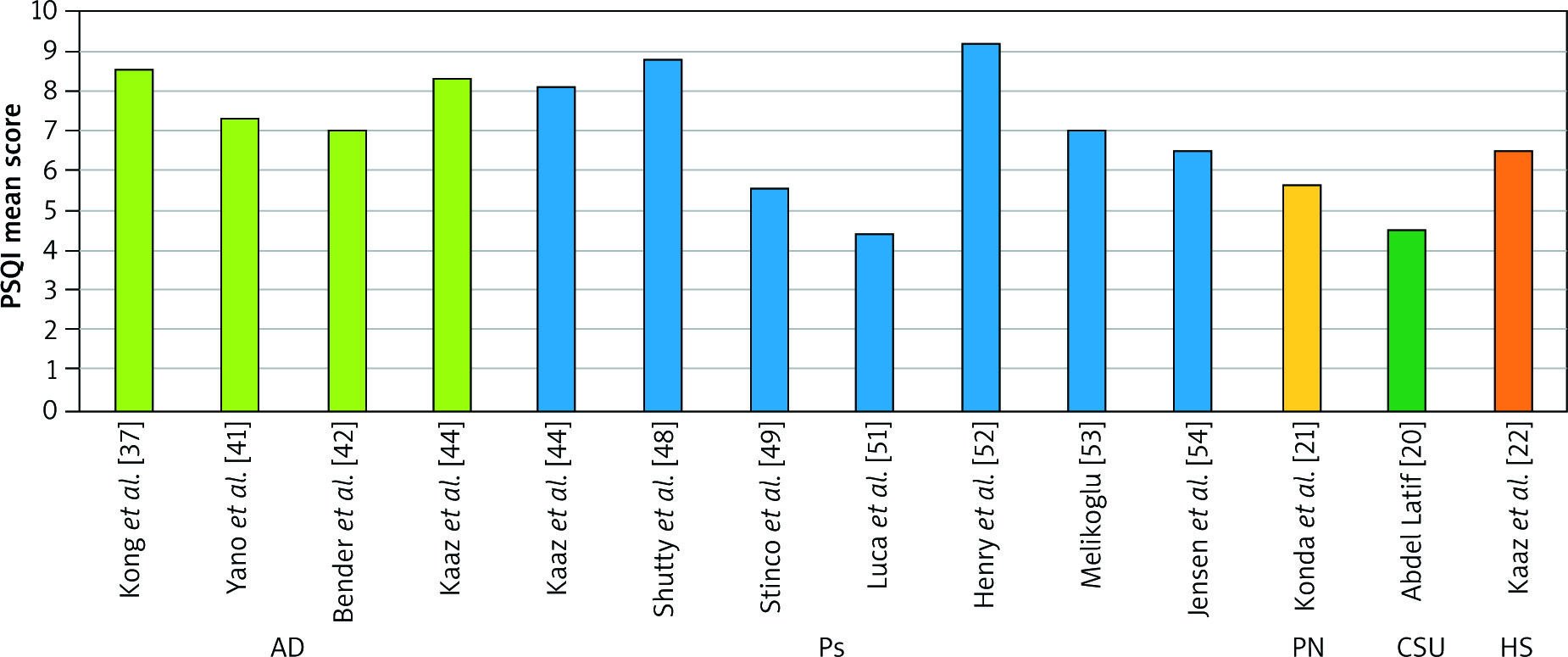
Table 1
Assessment studies of sleep quality among atopic dermatitis patients
| Study | Study design | Measure of sleep quality | Participants | Selected results |
|---|---|---|---|---|
| Bender et al., 2003 [42] | Case-control study | PSQI Actigraphy | 14 AD patients vs. 14 controls | PSQI mean scores: AD 7.0 ±0.75 points, control 3.42 ±0.81 points (p < 0.01) |
| Bender et al., 2008 [43] | Uncontrolled clinical study | PSQI Polysomnography Actigraphy | 20 AD patients | PSQI mean score – data not shown. Moderately strong correlations between actigraphy scores and both the scratching index and polysomnography scores, which included sleep latency, sleep efficiency, and stage-2 sleep, were revealed |
| Yano et al. 2013 [41] | Uncontrolled clinical study | PSQI | 112 AD patients | PSQI mean score: 7.3 ±2.8 points. PSQI score was significantly associated with DLQI (r = 0.43, p < 0.001) and with SCORAD (r = 0.33, p < 0.001) |
| Kong et al., 2016 [37] | Uncontrolled clinical study | PSQI | 50 AD patients | PSQI mean score: 8.51 ±7.32 points. PSQI scores significantly correlated with DLQI (p = 0.04) |
| Kaaz et al., 2018 [44] | Case-control study | PSQI | 100 AD patients vs. 50 controls | PSQI mean scores: AD patients 8.3 ±4.2 points, controls 3.1 ±1.9 points (p < 0.0001) |
| Bringhurst et al., 2004 [45] | Case-control study | Actigraphy | 15 AD patients vs. 30 controls | SCORAD score correlated with actigraphy activity score (per hour) (p < 0.05) |
| Sandoval et al., 2014 [38] | Uncontrolled clinical study | Actigraphy 14 days using wrist actigraphy monitors | 10 AD patients | AD severity positively correlated with sleep disturbances |
Plaque psoriasis
The average prevalence of psoriasis (Ps) in adults is assessed as 1–3% worldwide [46]. Skin lesions in Ps are typically scaly plaques covering the scalp, elbows and knees, but nails and any other skin areas can also be affected [47]. Psoriasis is associated with significant medical and psychological morbidity with a great impact on patients’ well-being. Sleep disturbance seems to be a common Ps-related problem in affected patients [18]. Eight reviewed studies were based on the PSQI questionnaire [44, 48–54], with six of them being case-control investigations [44, 48–50, 53, 54]. The mean PSQI scores ranged from 4.4 to 9.2 points (Figure 1) [44, 48, 49, 51–53], and were significantly higher compared to controls (p< 0.01) (Table 2) [44, 48, 53, 54]. In contrast to studies listed above, Stinco et al. [49] did not observe a link between psoriasis and poor sleep quality. In published data among Ps patients, a significant influence on subjective sleep quality [50, 53], daytime dysfunction [53] and sleep latency, sleep duration, sleep disturbances and use of sleeping medication domains [44] was established. Moreover, habitual sleep efficiency was significantly impaired in three studies [44, 50, 53]. PSQI scores were significantly correlated with severity of psoriasis assessed by the Psoriasis Area and Severity Index (PASI) (p = 0.03) [53] and itch severity (p< 0.001) [44]. The MOS-SS questionnaire was used in three studies, revealing comparable results [36, 48, 55]. Furthermore, Mrowietz et al. [56] reported that Ps patients complaining of severe itch were more prone to develop sleep impairment evaluated by mean MOS-SS score (p< 0.001). Psoriasis-related itch seems to play a substantial role in impairing sleep quality of Ps patients [44, 56]. The study based on polysomnography presented similar sleep structure with similar total sleep time and somnolence score among Ps patients with and without OSAHS [57]. Nonetheless, worse sleep quality and increased snoring frequency in Ps patients with OSAHS compared to Ps patients without OSAHS were revealed [57]. Furthermore, Pappadavid et al. [57] suggested that OSAHS may be a comorbidity in overweight Ps patients with hypertension, making this combination particularly unfavorable in the terms of sleep quality. Additionally, it was confirmed that adalimumab and etanercept treatment significantly improved sleep quality among Ps patients [36, 55, 56]. Detailed characteristics are shown in Table 2.
Table 2
Assessment studies of sleep quality among plaque psoriasis patients
| Study | Study design | Measure of sleep quality | Participants | Selected results |
|---|---|---|---|---|
| Strober et al., 2012 [36] | Clinical trial | MOS-SS SPI I and SPI II | 152 Ps patients | MOS-SS scores: – SPI I mean score 34.1 ±17.4 points – SPI II mean score 35.1 ± 17.4 points Adalimumab treatment improved sleep outcomes of Ps patients |
| Shutty et al., 2013 [48] | Case-control study | PSQI | 35 Ps patients vs. 44 controls | PSQI mean scores: Ps patients 8.8 ±4.4 points, controls 6.3 ±4.4 points (p = 0.008) |
| Stinco et al., 2013 [49] | Case-control study | PSQI | 202 Ps patients vs. 202 controls | PSQI mean score: Ps patients 5.56 ±3.93 points, controls 5.13 ±4.16 points |
| Mrowietz et al., 2014 [56] | Clinical trial | MOS-SS SPI II | 270 Ps patients | MOS-SS scores: 1. SPI II mean score: – No itch 22.17 ± 18.17 points, – Mild-to-moderate itch 29.60 ±15.86 points, Severe itch 37.52 ±19.86 points. MOS-SS scores were significantly associated with itch. Etanercept treatment significantly improved quality of sleep in patients with clinically meaningful improvement in itch versus with no clinically meaningful improvement in itch |
| Thaci et al., 2014 [55] | Clinical trial | MOS-SS SPI II | 270 Ps patients | MOS-SS mean score: SPI II mean score 34.0 points. Etanercept treatment significantly improved quality of sleep. Sleep improvement was associated with improved QoL |
| Balta et al., 2016 [50] | Case-control study | PSQI | 37 Ps patients vs. 42 controls | PSQI mean score – data not shown. The PSQI subscales for subjective sleep quality and habitual sleep efficiency (p = 0.04 and p = 0.01, respectively) |
| Luca et al., 2016 [51] | Uncontrolled clinical study | PSQI | 102 Ps patients | PSQI mean score 4.4 ±3.6 points |
| Henry et al. 2017 [52] | Uncontrolled clinical study | PSQI | 186 Ps patients | PSQI mean score: 9.2 ±4.3 points |
| Melikoglu, 2017 [53] | Case-control study | PSQI | 58 Ps patients vs. 58 controls | PSQI mean score: Ps patients 7.01 ±4.19 points, controls 4.18 ±2.76 points (p < 0.0001). PSQI and PASI were significantly correlated (p = 0.03) |
| Jensen et al., 2018 [54] | Case-control study | PSQI | 179 Ps patients vs. 105 controls | PSQI mean score: Ps patients 6.5 ±3.5 points, controls 4.2 ±2.4 points (p < 0.0001) |
| Kaaz et al., 2018 [44] | Case-control study | PSQI | 100 Ps patients vs. 50 controls | PSQI mean score: Ps patients 8.1 ±4.8 points, controls 3.1 ±1.9 points (p < 0.0001). The severity of itch was significantly correlated with PSQI scores (r = 0.59, p < 0.001) |
| Pappadavid et al., 2013 [57] | Uncontrolled clinical study | Polysomnography | 35 Ps patients | Ps patients with obstructive sleep apnea and hypopnea syndrome (OSAHS) presented more frequent snoring and lower sleep quality compared with those without OSAHS. OSAHS may be a comorbidity in obese psoriasis patients with hypertension |
Prurigo nodularis
Prurigo nodularis (PN) is a chronic skin condition of still unknown etiology. The PN is characterized by firm nodules, mostly localized symmetrically over the extensor surfaces of the lower extremities. Skin lesions are either primary or secondary to repeated traumatic manipulation due to chronic itch [58]. The PN is associated with a significant burden of disease, contributing to mood disorders and disrupting sleep quality [59]. Konda et al. [21] suggested that PN, itching, sleep disturbance and depression may be interrelated symptoms with the same underlying mechanism in the form of immune system activation and lower serum serotonin. In a case-control study among 39 PN patients and 39 controls, PSQI mean scores were assessed as 5.59 ±3.73 points and 4.46 ±2.82 points, respectively [21]. Moreover, sleep quality in PN patients assessed by PSQI significantly correlated with the outcomes of the 17-item version of the Hamilton Depression Rating Scale (HDRS-17) (r = 0.635, p< 0.01) [21]. Nonetheless, the quality of sleep did not correlate with itch severity [21].
Chronic spontaneous urticaria
Chronic spontaneous urticaria (CSU) is defined by the spontaneous appearance of wheals with or without edema that persist for more than 6 weeks [60]. The mean disease prevalence is estimated up to 1% of the general population [61]. The CSU can be very distressing and may severely impair the QoL [62]. Sleep quality estimated with the PSQI questionnaire among CSU patients (mean PSQI score: 4.5 points) was significantly impaired when compared to the controls (mean PSQI score: 4.0 points) (p< 0.001) [20]. Additionally, the severity of urticarial symptoms assessed with the Urticaria Activity Score over 7 days (UAS-7) significantly correlated with decreased sleep quality (i.e. PSQI scores) (p = 0.00001) [20]. Furthermore, a study by Abdel Latif showed a significant influence on sleep latency, sleep duration, sleep disturbance and daytime dysfunction domains [20]. Gimenéz-Arnau et al. [63], reporting the results of three randomized, double-blind, placebo-controlled studies, found a substantial improvement of sleep quality assessed by MOS-SS SPI-II under omalizumab treatment.
Hidradenitis suppurativa
Hidradenitis suppurativa (HS) is a chronic, recurrent, inflammatory, suppurative and debilitating disease of the hair follicle manifested by painful abscesses, fistulas and scarring lesions in the apocrine gland-bearing areas of the body, mostly the axillae, inguinal and anogenital regions [64]. The disease affects up to 1% of the general population with female predominance [65, 66]. The HS-related QoL impairment includes an impact on multiple aspects of psychophysical functioning and well-being in affected patients, resulting in decreased overall activity, depression, anxiety, fatigue and stigmatization [67, 68]. A case-control study, involving 108 HS patients and 50 controls, established a significantly decreased sleep quality among HS sufferers compared to controls (PSQI mean scores assessed as 6.5 ±3.6 points and 3.1 ±1.9 points, respectively (p< 0.0001)) [22]. Additionally, significant influences on sleep latency, sleep duration and sleep disturbance were revealed [22]. Of note, pain seems to play a crucial role in impairing sleep quality of HS patients [22].
Discussion
Chronic skin diseases, such as atopic dermatitis, psoriasis, prurigo nodularis, chronic urticaria and hidradenitis suppurativa, have a great impact on health-related QoL of affected individuals [40, 59, 62, 67–69]. Skin plays an important role in proper sleep physiology. Itch, pain, mood, cognitive and somatic arousal or anxiety were established as having a potential impact on sleep quality [18, 52]. The negative influence of itch on the quality of sleep was revealed in patients with chronic inflammatory dermatoses such as AD and Ps [70–72]. This study was undertaken to examine sleep quality in patients with chronic skin diseases, with a particular focus on atopic dermatitis, plaque psoriasis, prurigo nodularis, chronic urticarial and hidradenitis suppurativa. In available studies the quality of sleep was assessed by objective and/or subjective methods.
In atopic dermatitis patients the mean total PSQI scores ranged from 7.0 to 8.5 points (Table 1) [37, 41, 42, 44]. Affected sleep quality significantly correlated with reduced QoL [37, 41]. Furthermore, subjective sleep quality and daytime dysfunction were found to be the most affected parameters in AD patients as compared to the controls [42]. Nonetheless, a previously published study revealed that all PSQI domains were significantly affected in AD patients [44]. Poor sleep quality assessed by PSQI significantly correlated with AD severity estimated with SCORing of Atopic Dermatitis (SCORAD) [41]. The AD patients with more severe disease assessed with Investigator Global Assessment (IGA) and the Eczema Area and Severity Index (EASI) had worse sleep measured by actigraphy, as was demonstrated by the marker of sleep disruption wake after sleep onset (WASO) [38]. Moreover, the perception of itch assessed by actigraphy increased with poor efficiency of sleep and more minutes awake [42]. Furthermore, investigators suggested that the number of awakenings and increasing number of minutes awake are associated with increased itch and impaired QoL [42]. A study by Bender et al. [43] revealed moderately strong correlations between actigraphy scores and both the scratching index and PSG scores, which included sleep latency, sleep efficiency and stage-2 sleep. Furthermore, they found that sleep quality decreases as the severity of AD increases [43] and suggested that objective measures (actigraphy and polysomnography), contrary to self-reported questionnaires, are more useful to demonstrate that the increased AD severity results in the impairment of sleep quality and more scratching [43].
In psoriasis patients PSQI mean scores were assessed as 4.4–9.2 points (Table 2) [44, 48, 49, 52, 53]. The Ps significantly affected subjective sleep quality, daytime dysfunction and habitual sleep efficiency as compared to the controls [50, 53]. A recently published study showed a significant impact of Ps on sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances and use of sleeping medication [44]. In a study published by Melikoglu a significant association between global PSQI score and Ps severity assessed by PASI was established [53]. Balta et al. [50] suggested that poor sleep quality may be associated with the itch and pain caused by Ps-linked skin lesions. Nonetheless, only itch severity, but not pain, significantly correlated with PSQI total score [44]. Furthermore, it was found that improved psoriasis control with itch reduction may increase sleep quality of affected patients [54]. The Ps patients with moderate-to-severe disease have impaired sleep quality, which is linked to poor QoL [55]. Moreover, Shutty et al. [48] suggested that sleep disturbances associated with Ps may be secondary to depression rather than related to a Ps direct effect. The obstructive sleep apnea and hypopnea syndrome (OSAHS), which may be a comorbidity in obese psoriasis patients with hypertension, was indicated as a potential predictor of poor sleep quality [57]. It was also noted that sleep quality in Ps patients on adalimumab or etanercept treatment was improved [36, 55, 56].
In prurigo nodularis patients the mean PSQI score was 5.59 points [21]. Konda et al. [21] established no significant correlation between the severity of itch and depression severity or sleep quality. Nonetheless, a significant correlation between sleep quality and depression in PN patients was found (r = 0.635, p< 0.01).
In chronic spontaneous urticaria patients PSQI mean score was 4.5 points – a significantly higher result as compared to the controls (p< 0.001) [20]. Furthermore, increased severity of the urticaria symptoms assessed by UAS-7 correlated with poor sleep quality (PSQI mean score). Moreover, it was demonstrated that such parameters as sleep duration, sleep disturbance, sleep latency and day dysfunction due to sleepiness in CSU patients were significantly affected, as compared to the controls [20]. Gimenéz-Arnau et al. [63] established sleep improvement among CSU patients receiving omalizumab.
In hidradenitis suppurativa patients the mean PSQI score was assessed as 6.5 points and was significantly higher than in the control group (p< 0.0001) [22]. Sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances and daytime dysfunction were also significantly affected in HS patients, as compared to the controls. Moreover, pain seems to be a crucial factor affecting the sleep quality of HS patients.
Zachariae et al. [73] suggested that itch-related sleep impairment could be a significant partial mediator of the relationship between somatic and psychological symptoms and the severity of itch. It is recommended that clinicians ask patients about the current sleep quality during a routine evaluation of the clinical severity of a chronic skin disease and request further consultations when necessary. Polysomnography and actigraphy should be performed for the objective assessment of sleep quality. Nonetheless, a questionnaire-based evaluation of sleep quality is more useful in clinical practice and clinical studies. Moreover, further immunologic or neurologic clinical studies are necessary to investigate the relationship between chronic skin diseases and sleep disorders.
In conclusion, subjective symptoms such as itch and pain have a substantial impact on sleep quality and general quality of life in patients with chronic skin diseases.
Moreover, further investigation into objective measurements of the quality of sleep, such as long-term questionnaire-based epidemiological studies, is necessary to understand the nature and exact mechanism of poor sleep among sufferers with chronic skin diseases. Therefore, reliable guidelines concerning the evaluation and management of sleep disorders in chronic dermatological patients should be provided. Furthermore, the management of sleep disturbance in patients with chronic dermatoses should focus on effective disease control with strategies for itch and pain relief as well as on possible medical interventions to help improve sleep.