






Introduction
Despite improvements in balloon and stent technology, percutaneous coronary intervention (PCI) in calcified, tortuous, angulated or previously stented vessels is still a therapeutic challenge. The proper preparation of the vessel, confirmed by the smooth passage of smaller balloon catheters, often remains insufficient to deliver a larger, stiffer balloon or stent catheter in place of the target lesion.
We describe a modified buddy balloon catheter technique that facilitates the deliverability of larger balloons or stents to these challenging lesions when the routinely used buddy wire technique as the first step fails.
The small buddy balloon catheter technique is a simple extension of the buddy wire technique in which a small monorail uninflated balloon, of up to 1.5 mm, is positioned on the buddy wire distally or at the point where the balloon/stent becomes stuck. The small buddy balloon catheter appears to reduce the resistance of the rough surface, especially the angulated segment of the vessel, and facilitates other balloon or stent catheter passage. This does not concern a balloon inflation but rather catheter shaft properties. Since that technique is used in our high-volume catheterization laboratory with a surprisingly high success rate we think that it is worth sharing our experience with other operators. Consequently, we have decided to present these 2 cases.
Case reports
Case 1
A 76-year-old man with a history of previous PCI was readmitted with symptoms of recurrent angina. Three months earlier the patient in unstable condition was hospitalized. The coronary angiography revealed a severe left main (LM) bifurcation stenosis with proximal segments of left anterior descending (LAD) and left circumflex artery (LCx) involvement (Medina 1-1-1). Due to severe comorbidities he was disqualified from coronary artery bypass grafting by the Heart Team and treated with the two-stent strategy PCI of LM bifurcation involving long proximal segments of the LAD and LCx.
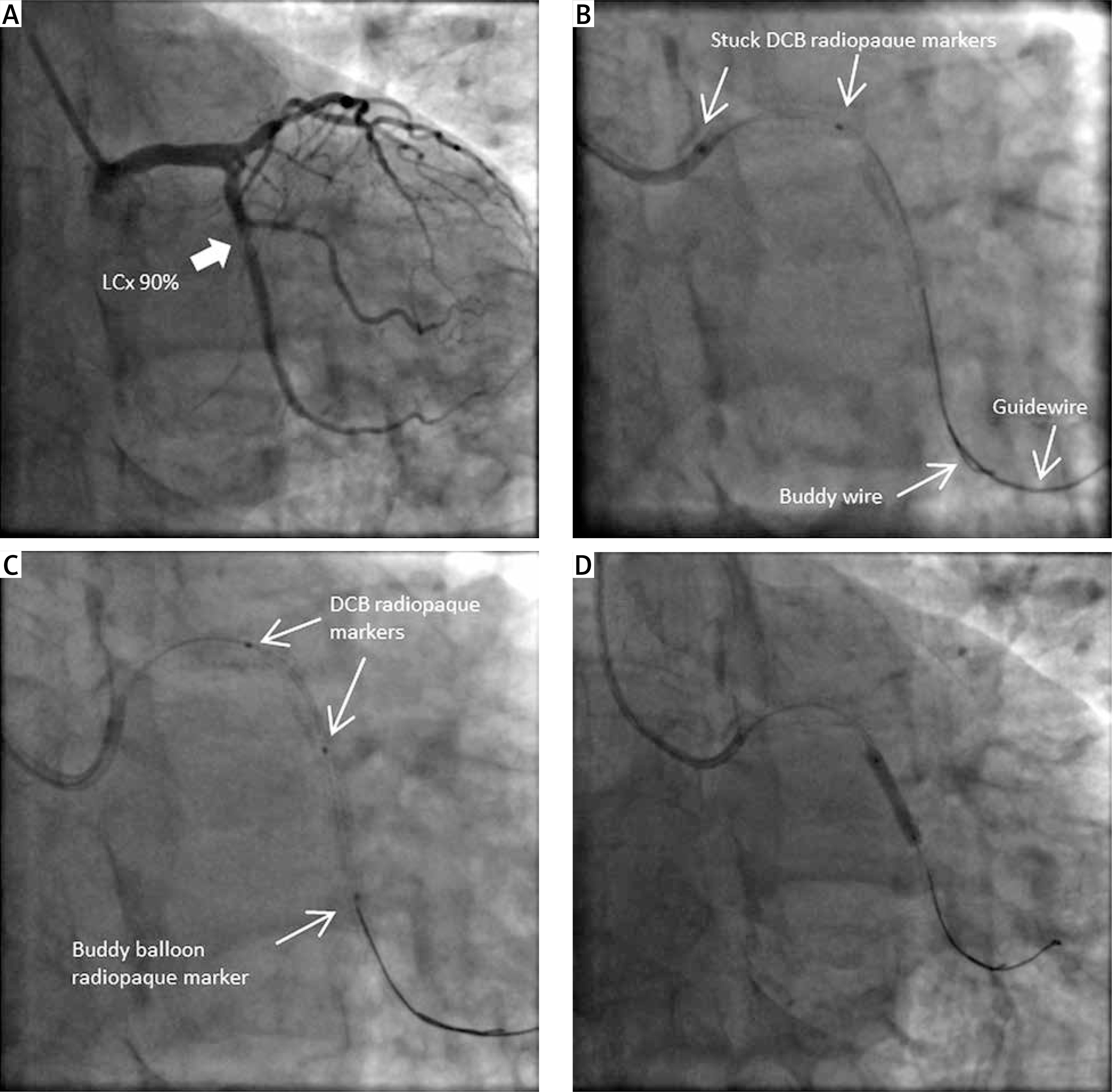
On current admission the coronary angiography showed in-stent restenosis in the medium LCx segment. The decision to perform drug-coated balloon (DCB) angioplasty by a radial approach and using the 6F JL 3.5 catheter was made. After crossing the lesion with a Sion Blue guidewire a successful pre-dilation with semi-compliant balloon Artimes 3.0 × 20 mm was performed. However, the DCB SeQuent Please Neo 3.0 × 20 mm stuck in the LM at the level of the previously stented LCx ostium (Figure 1 B). Therefore, another Sion Blue guidewire, as a buddy wire, was used to facilitate the DCB entering into the LCx through the calcified, stented angle. Due to the attempt being unsuccessful, a small buddy balloon (Mini Trek 1.2 × 8 mm, Abbott Vascular) was positioned on the guide wire distally to the stuck segment without inflation. This small buddy balloon catheter allowed for smooth delivery of the DCB to the lesion (Figure 1 C). Successful long inflation (60 s) was performed and the procedure was completed (Figure 1 D).
Figure 1
Right anterior oblique views: A – In-stent restenosis in medium LCx segment, B – DCB stuck at the edge of previously stented LCx ostium, despite buddy wire support (radiopaque markers of DCB, guidewire, buddy wire), C – Small buddy balloon catheter facilitates the DCB crossing (single radiopaque marker of buddy balloon) (radiopaque markers of DCB), D – Successful DCB inflation
LCx – left circumflex artery, DCB – drug-coated balloon.
Case 2
A 73-year-old woman was admitted to the hospital with deteriorating angina symptoms, CCS (Canadian Cardiovascular Society) functional class III, for coronary angiography. She had a history of coronary artery disease with PCI of the LAD as well as recanalization of LCx chronic total occlusion with proximal stent implantation using the T-stent technique.
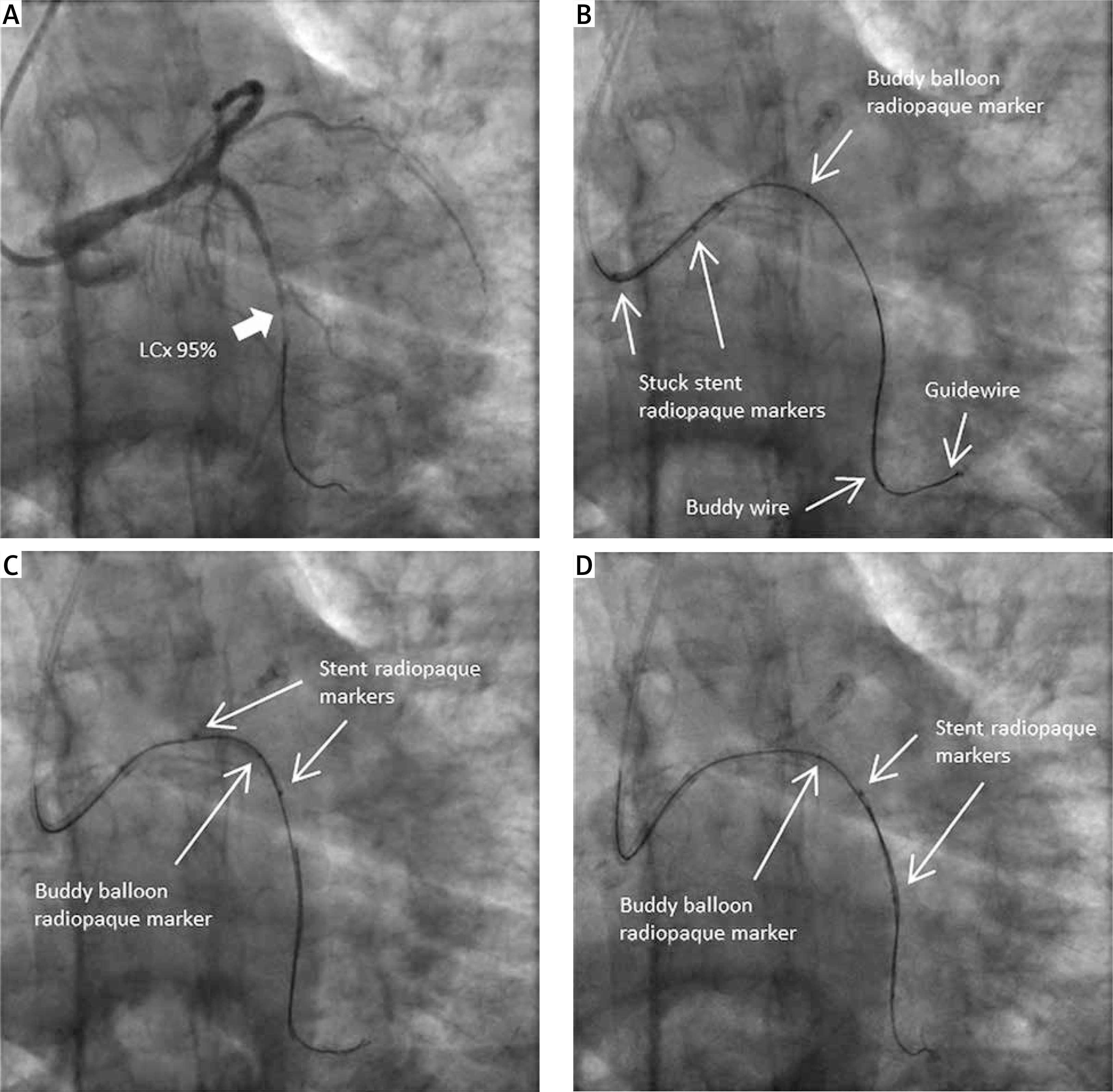
Coronary angiography revealed subtotal occlusion of the LCx distally to the previously implanted stent. The decision to revascularize the LCx with drug-eluting stent implantation by a radial approach and using a 6F EBU 3.5 guiding catheter was made. After crossing the lesion with a Sion Blue guidewire, pre-dilation with a semi-compliant TREK balloon (Abbott Vascular) 2.5 × 15 mm was performed. Surprisingly, the Xience Pro 2.25 × 23 mm stent was stuck at the proximal edge of the LCx stent (Figure 2 A). In the next step, a buddy wire was used to facilitate the stent deployment in the artery, but this technique also proved unsuccessful. Finally, the operator decided to use the small buddy balloon catheter technique with a Mini Trek 1.5 × 15 mm balloon positioned at the site of the stuck stent (Figure 2 B). This technique allowed for a smooth delivery of the stent to the lesion (Figures 2 C, D). After retrieving the buddy wire with the buddy balloon catheter, successful stent deployment was performed and the procedure was completed.
Figure 2
Right anterior oblique views: A – Subtotal occlusion of a medium LCx segment, B – Small buddy balloon via buddy wire at the stuck site (single radiopaque marker of buddy balloon, radiopaque stent markers), C – Small buddy balloon catheter facilitates the stent crossing, D – Successful stent delivery
LCx – left circumflex artery, DCB – drug-coated balloon.
Discussion
Buddy wire technique is commonly used during endovascular procedures to provide extra support for balloon or stent catheter passage through a tortuous, calcified or previously stented segment of the coronary vessel [1–3]. However, in some cases the deliverability of stents or less commonly balloons through well-prepared, relatively wide coronary vessels, despite the buddy wire application, still poses significant difficulties. In such cases, instead of inserting multiple buddy wires, using a small buddy balloon catheter over one buddy wire simplifies the procedure. The small buddy balloon catheter technique is not appropriate for passage through tight lesions, where cutting balloons, rotational atherectomy or shock wave balloons should be used. It does not refer to an arterial lumen issue but rather to the difficulties of crossing through a tough, tortuous segment, calcified eccentric plaque or edge of a previously implanted stent.
The key to this technique is the properties of the catheter shaft, not the balloon inflation. Contrary to the distal buddy balloon technique where the balloon has to be inflated, we avoid the risk of distal artery segment damage [4]. An additional small balloon catheter poses no risk of stent dislodgement and is easy to deliver through the routinely used 6F guiding catheter. In our center we used, as buddy balloon catheters, small monorail balloons of up to 1.5 mm with one radiopaque marker, which easily crosses the stuck segment, and still larger balloons could probably be used as well, as suggested by other authors [5]. Special types of guiding wires and guiding catheters are not required. However, it must be pointed out that unlike in the case of the buddy wire technique, where the buddy wire can be ‘jailed’, here the buddy balloon must be retrieved prior to stenting [1, 6].